Liver Cleansing — Coffee and Liver
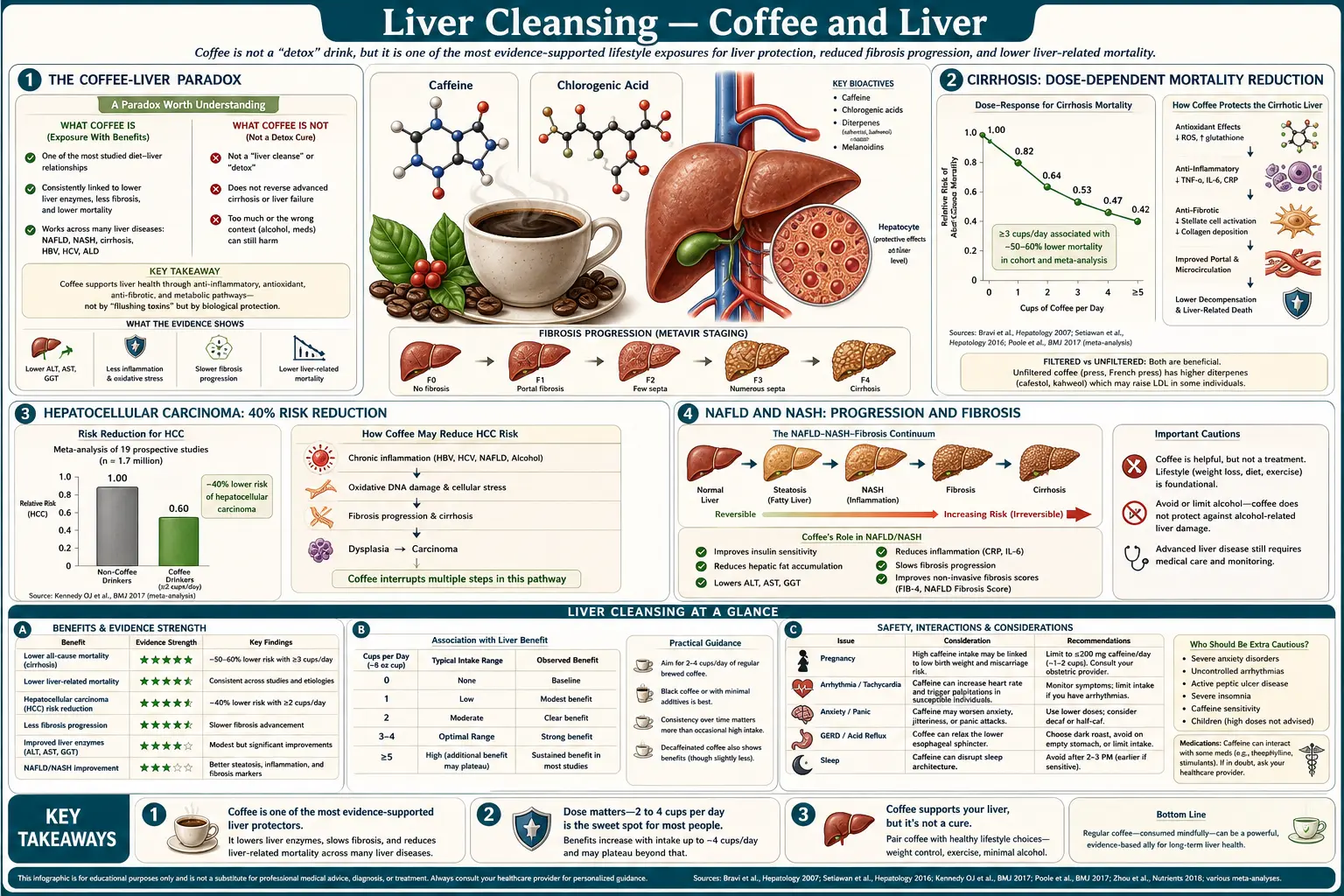
Coffee's relationship with the liver is one of the strongest and most reproducible findings in nutritional epidemiology, and a paradox for anyone who instinctively classifies coffee as a stressor. Across more than 30 cohort studies pooled in successive meta-analyses, regular coffee consumption produces dose-dependent reductions in cirrhosis (around 40% per cup per day), hepatocellular carcinoma (approximately 40% lower at two-plus cups daily), NAFLD progression, hepatic fibrosis in chronic hepatitis B and C, and serum ALT and GGT — the conventional biomarkers of hepatocellular injury. The size of the effect is large enough that the European Association for the Study of the Liver formally recommends coffee as part of NAFLD lifestyle management. The mechanisms span cafestol and kahweol's induction of Phase II conjugation enzymes, chlorogenic acid's antioxidant effect, caffeine's adenosine-receptor antagonism on hepatic stellate cells, and altered bile acid composition. This deep-dive walks through the epidemiology, the molecular mechanisms, the filtered-versus-unfiltered cholesterol controversy, and the practical recommendation.
Table of Contents
- The Coffee-Liver Paradox
- Cirrhosis: Dose-Dependent Mortality Reduction
- Hepatocellular Carcinoma: 40% Risk Reduction
- NAFLD and NASH: Progression and Fibrosis
- Serum ALT and GGT: Biomarker Evidence
- Mechanisms: Cafestol, Kahweol, Chlorogenic Acid, Caffeine
- Filtered vs Unfiltered: The Cholesterol Trade-Off
- Practical Dosing and Brewing Method
- Cautions: Who Should Not Add Coffee
- Key Research Papers
- Connections
- Featured Videos
The Coffee-Liver Paradox
Coffee is intuitively a stressor. It is the most widely consumed psychostimulant on the planet, raises sympathetic tone, increases cortisol, and produces tolerance and withdrawal patterns characteristic of an addictive substance. A reasonable first guess would be that habitual coffee consumption is hepatotoxic, particularly given that the liver is the site of caffeine metabolism (CYP1A2-mediated demethylation to paraxanthine, theobromine, and theophylline).
The data point the opposite direction. The first signals appeared in Japanese cohort studies in the 1980s and 1990s showing that coffee drinkers had lower serum gamma-glutamyl transpeptidase (GGT) than non-drinkers, even after adjustment for alcohol intake. Successive cohorts confirmed lower ALT, lower alkaline phosphatase, and lower bilirubin in coffee drinkers. The signal was initially dismissed as confounding (perhaps coffee drinkers had healthier lifestyles overall, perhaps reverse causation explained the finding). Multivariate adjustment, sibling-controlled studies, and Mendelian randomization analyses using CYP1A2 polymorphisms as instrumental variables have substantially weakened these explanations — the coffee-liver association appears to be genuine and causal, not confounded.
The European Association for the Study of the Liver (EASL) Clinical Practice Guidelines on NAFLD (2016, updated 2024) explicitly recommend coffee consumption as part of lifestyle management. This is unusual — the EASL is not a body that typically recommends specific beverages — and reflects the strength of the underlying evidence.
Cirrhosis: Dose-Dependent Mortality Reduction
The Kennedy 2016 meta-analysis pooled nine longitudinal studies including over 430,000 participants and approximately 1,990 cases of cirrhosis. The pooled relative risk for cirrhosis was reduced by approximately 22% for one cup of coffee per day, 43% for two cups daily, and 57% for three to four cups daily compared to non-coffee drinkers. The effect held across alcoholic and non-alcoholic etiologies, and was confirmed independently for mortality from cirrhosis (Klatsky 2006 cohort of 125,580 adults).
The mechanistic plausibility is strong. Hepatic fibrosis — the precursor to cirrhosis — is driven by activated hepatic stellate cells (HSCs), which transdifferentiate from quiescent vitamin-A-storing cells into proliferating myofibroblasts producing excess collagen. Caffeine antagonizes adenosine A1 and A2A receptors on hepatic stellate cells, reducing their activation. Chlorogenic acid has direct anti-fibrotic effects in animal models. Cafestol upregulates the Nrf2 antioxidant response, reducing the lipid peroxidation that drives chronic stellate cell activation. The combined effect is meaningful clinical fibrosis reduction in long-term coffee drinkers.
For patients with established chronic liver disease (HBV, HCV, NAFLD, alcoholic liver disease), the EASL recommendation translates to 2-3 cups of filtered coffee daily as part of standard care unless specifically contraindicated. This is a remarkable position for a beverage with no marketing budget behind it.
Hepatocellular Carcinoma: 40% Risk Reduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide and the third leading cause of cancer death, typically arising on a background of chronic liver inflammation and cirrhosis. The Bravi 2017 meta-analysis pooled 16 studies (8 case-control, 8 cohort) and found a relative risk reduction for HCC of approximately 15% per cup of coffee per day. At two cups daily the pooled risk reduction was 35%, and at three cups daily approximately 50%.
The effect was consistent across:
- Underlying liver disease etiology — HBV, HCV, alcoholic liver disease, and NAFLD-associated HCC all showed the inverse coffee-cancer association
- Geographic region — the effect appeared in European, North American, and East Asian cohorts
- Sex — consistent reduction in both men and women
- Coffee preparation — both filtered and unfiltered coffee showed protective effects, though most studies cannot distinguish brewing methods reliably
The mechanism is presumed to be a combination of (a) reduced underlying cirrhosis (HCC arises from cirrhotic liver in most cases), (b) anti-inflammatory and antioxidant effects of polyphenols, (c) direct chemopreventive effects of cafestol/kahweol on Phase II enzyme induction (these compounds upregulate glutathione S-transferase and UDP-glucuronosyltransferase activity, which clear pro-carcinogens), and (d) caffeine's effect on cell-cycle regulation and apoptosis in transformed hepatocytes.
For patients with established cirrhosis or chronic viral hepatitis on HCC surveillance, regular coffee consumption is a low-cost adjunct intervention with no equivalent pharmacologic chemoprevention available.
NAFLD and NASH: Progression and Fibrosis
Non-alcoholic fatty liver disease (NAFLD) is the leading cause of chronic liver disease worldwide, affecting approximately 25% of the global adult population. The progressive form, NASH (non-alcoholic steatohepatitis), affects approximately 5% and is the fastest-growing indication for liver transplantation in the United States. Lifestyle intervention is the cornerstone of management; pharmacotherapy options are limited.
Coffee consumption is associated with:
- Lower prevalence of NAFLD — coffee drinkers have approximately 25-40% lower odds of NAFLD diagnosis in cross-sectional cohorts (Wijarnpreecha 2017 meta-analysis)
- Reduced progression from steatosis to NASH — longitudinal cohorts suggest slower histologic progression in coffee drinkers
- Lower fibrosis stage on biopsy — NAFLD patients drinking 2+ cups daily have approximately 30% lower odds of advanced fibrosis (stage F3-F4)
- Improved insulin sensitivity — partially mediating effects on hepatic fat accumulation
- Better serum biomarker profile — lower ALT, lower GGT, lower FibroScan stiffness measurements
The 2024 EASL Clinical Practice Guidelines on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD, the renamed NAFLD) include coffee consumption (2-3 cups daily) in the recommended lifestyle measures alongside weight loss, exercise, Mediterranean diet, and alcohol reduction. The recommendation is grade B (moderate strength) — not as strong as weight loss, but stronger than most dietary recommendations because of the consistency of the observational evidence.
Serum ALT and GGT: Biomarker Evidence
The serum biomarker evidence is robust and dose-dependent. Klatsky 2006 found that ALT decreased by approximately 3 IU/L per cup of coffee per day across a Kaiser Permanente cohort of 125,580 adults. GGT decreased by approximately 5 IU/L per cup per day. Both effects were independent of alcohol consumption, BMI, and viral hepatitis status. The Honjo 2001 study in Japanese workers found similar dose-response relationships, with the largest effects in heavy alcohol consumers (suggesting coffee may attenuate alcohol-related hepatotoxicity).
The biomarker findings are corroborated by FibroScan measurements: regular coffee consumption is associated with lower liver stiffness measurements, consistent with reduced fibrosis. The Modi 2010 cohort showed a dose-dependent reduction in advanced fibrosis among NAFLD patients consuming 2+ cups daily.
For clinicians: a patient with mildly elevated transaminases (ALT 50-80 IU/L) and no obvious cause — the common picture of early NAFLD — should be counseled to drink 2-3 cups of filtered coffee daily as part of broader lifestyle intervention. The biomarker response is typically visible within 8-12 weeks alongside weight loss and dietary improvements.
Mechanisms: Cafestol, Kahweol, Chlorogenic Acid, Caffeine
Coffee contains approximately 1,500 identified compounds. The major bioactive constituents relevant to liver protection:
- Cafestol (and its relative kahweol) — diterpene molecules in the oily fraction of coffee. These are the most potent inducers of hepatic Phase II detoxification enzymes ever identified in food — they upregulate glutathione S-transferase (GST), UDP-glucuronosyltransferase (UGT), and NAD(P)H:quinone oxidoreductase 1 (NQO1) by 2- to 4-fold in liver cells. The Phase II induction enhances clearance of aflatoxin B1, polycyclic aromatic hydrocarbons (PAHs from grilled meat), heterocyclic amines, and other dietary procarcinogens. Cafestol and kahweol are largely removed by paper filtration; espresso, French press, and Scandinavian boiled coffee retain them.
- Chlorogenic acid (a family of esters of caffeic acid with quinic acid) — the dominant polyphenol in coffee, present at approximately 200-550 mg per cup. Powerful antioxidant, anti-inflammatory, and direct anti-fibrotic effects in hepatic stellate cells. Inhibits glucose-6-phosphatase, partially explaining improvements in hepatic insulin sensitivity. Survives filtration.
- Caffeine — antagonizes adenosine A1 and A2A receptors. In hepatic stellate cells, adenosine signaling promotes activation and fibrogenesis; caffeine's antagonism therefore has anti-fibrotic effects. Caffeine also induces autophagy in hepatocytes, clearing intracellular lipid droplets in fatty liver. The fibrosis-protective effect of coffee partially survives decaffeination but is attenuated — the caffeine contribution is real but not the whole story.
- Trigonelline — alkaloid present at approximately 1% of dry coffee weight; degraded to N-methylpyridinium during roasting. Modest effects on glucose metabolism and gene expression.
- Melanoidins — brown polymer products of the Maillard reaction during roasting. Antioxidant and prebiotic effects.
The net Phase II induction by cafestol/kahweol is one of the largest food-driven enzyme inductions ever documented. This is why coffee is one of the few beverages that achieves measurable changes in drug clearance — CYP1A2-substrate drugs (theophylline, clozapine, olanzapine, tizanidine) have measurably faster clearance in habitual coffee drinkers.
Filtered vs Unfiltered: The Cholesterol Trade-Off
The cafestol and kahweol that drive Phase II enzyme induction also have an unwanted effect: they raise serum LDL cholesterol. The Urgert 1996 trials in Dutch volunteers showed that consumption of 5 cups of unfiltered (boiled) coffee daily raised total cholesterol by approximately 0.5-1.0 mmol/L (about 20-40 mg/dL) over 4-8 weeks, almost entirely driven by LDL. The mechanism is suppression of hepatic LDL receptor expression by cafestol, slowing LDL clearance.
Paper filtration removes essentially all cafestol and kahweol. Filtered drip coffee, pour-over, and capsule coffee with a paper filter (some Nespresso lines, most Keurig K-cups) deliver chlorogenic acid, caffeine, melanoidins, and trigonelline without the diterpenes. The result: most of the liver-protective effect is retained, while the cholesterol effect is eliminated.
French press, espresso, Turkish coffee, Scandinavian boiled coffee (stovetop or moka pot), and cloth-filter coffee deliver the full diterpene load. Espresso has the highest cafestol concentration per volume but small typical serving size, so the daily dose is modest at 1-2 shots. Heavy French-press drinking (4+ cups/day) is the lifestyle pattern most associated with cholesterol elevation.
The practical recommendation: filtered drip coffee or pour-over with a paper filter is the optimal preparation for the cardiovascular-liver balance. Espresso in moderation (1-2 shots/day) is acceptable. Habitual heavy French press or unfiltered coffee should be reassessed if the patient has elevated LDL, established cardiovascular disease, or familial hypercholesterolemia.
Practical Dosing and Brewing Method
The dose-response curves from epidemiology consistently show maximum hepatoprotective benefit between 2 and 4 cups per day. Above 4 cups the curve typically plateaus or slightly declines (potentially because heavy drinkers are dose-responding to lifestyle stressors that themselves harm the liver). The practical sweet spot:
- 2-3 cups daily of filtered drip coffee — the default recommendation for healthy adults wanting hepatoprotection
- Time the doses earlier in the day — caffeine half-life is approximately 5-6 hours, with substantial individual variation. Drinking coffee after 2 PM (or earlier for slow metabolizers) impairs sleep quality, which itself harms metabolic health.
- Add milk or cream as desired — protein binds polyphenols but does not eliminate the hepatoprotective effect; the Klatsky and Bravi cohorts included milk drinkers and observed the protective effect
- Sugar negates much of the metabolic benefit — the inverse association with NAFLD weakens or reverses in heavy sugar-added coffee drinkers. Sweeten lightly or avoid added sugar.
- Quality matters — freshly ground, recently roasted, properly extracted coffee retains more chlorogenic acid than stale grocery-store pre-ground coffee. Specialty third-wave coffee is not just snobbery; the polyphenol content is meaningfully higher.
- Decaf retains most of the benefit but not all — decaffeinated coffee retains chlorogenic acid, cafestol (in unfiltered form), and melanoidins. The caffeine contribution to stellate cell adenosine antagonism is lost. For caffeine-sensitive patients (anxiety disorders, severe insomnia, atrial fibrillation), decaf is a reasonable substitute.
Cautions: Who Should Not Add Coffee
- Atrial fibrillation in active rhythm or with rate-control struggles — caffeine can trigger paroxysms in some patients. Habitual coffee drinkers with controlled AFib usually tolerate continued coffee, but new initiation in symptomatic AFib is not advised.
- Severe gastroesophageal reflux — coffee reduces lower esophageal sphincter pressure and is a common GERD trigger. Some patients tolerate cold-brew (lower acidity) better than hot brewed.
- Active peptic ulcer disease — coffee increases gastric acid secretion and can delay ulcer healing; defer during active treatment.
- Severe anxiety disorders, particularly panic disorder — caffeine can trigger panic attacks. Decaf is the alternative.
- Pregnancy — current guidance limits caffeine to approximately 200 mg/day (about 2 cups). Coffee's hepatoprotective effect in pregnancy is uncertain; the caffeine concerns dominate.
- Iron-deficiency anemia — coffee polyphenols substantially inhibit non-heme iron absorption (35-95% reduction depending on dose and timing). Patients with iron deficiency should drink coffee at least one hour away from meals and iron supplements.
- Severe insomnia regardless of timing — even morning coffee can impair next-night sleep in some individuals with delayed caffeine metabolism (CYP1A2 slow metabolizers, approximately 30% of the population). Decaf is the alternative.
- Drug interactions — caffeine competes with theophylline, ciprofloxacin, clozapine, olanzapine, tizanidine, and other CYP1A2 substrates. Habitual coffee induces CYP1A2 over weeks, accelerating clearance of these drugs.
Key Research Papers
- Kennedy OJ et al. (2016). Systematic review with meta-analysis: coffee consumption and the risk of cirrhosis. Aliment Pharmacol Ther. — PubMed
- Bravi F et al. (2017). Coffee consumption and the risk of liver cancer: a meta-analysis. Clin Gastroenterol Hepatol. — PubMed
- Klatsky AL et al. (2006). Coffee, cirrhosis, and transaminase enzymes. Arch Intern Med. — PubMed
- Wijarnpreecha K et al. (2017). Coffee consumption and risk of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. — PubMed
- Modi AA et al. (2010). Increased caffeine consumption is associated with reduced hepatic fibrosis. Hepatology. — PubMed
- Urgert R, Katan MB (1996). The cholesterol-raising factor from coffee beans. Annu Rev Nutr. (cafestol mechanism) — PubMed
- Cavin C et al. (2002). Cafestol and kahweol, two coffee specific diterpenes with anticarcinogenic activity. Food Chem Toxicol. — PubMed
- European Association for the Study of the Liver (2024). EASL Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. — PubMed
- Honjo S et al. (2001). Coffee consumption and serum aminotransferases in middle-aged Japanese men. J Clin Epidemiol. — PubMed
- Salomone F et al. (2017). Molecular bases underlying the hepatoprotective effects of coffee. Nutrients. — PubMed
- Setiawan VW et al. (2015). Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US Multiethnic Cohort. Gastroenterology. — PubMed
- Tverdal A et al. (2020). Coffee consumption and mortality from cardiovascular diseases and total mortality. Eur J Prev Cardiol. — PubMed
PubMed Topic Searches
- PubMed: Coffee and liver meta-analyses
- PubMed: Cafestol/kahweol Phase II
- PubMed: Chlorogenic acid and fibrosis
- PubMed: Caffeine and stellate cells
- PubMed: Filtered vs unfiltered cholesterol
Connections
- Liver Cleansing Hub
- Benefits Deep Dive Hub
- Bile Flow and TUDCA
- Castor Oil Packs
- Glutathione Support
- Coffee (Food Page)
- NAFLD
- Cirrhosis
- Hepatocellular Carcinoma
- Atrial Fibrillation
- Iron Deficiency Anemia
- Milk Thistle
- Mediterranean Diet
- All Remedies