Liver Cleansing — Benefits Deep Dive
The liver is the body's primary site of biotransformation — the only organ capable of converting fat-soluble xenobiotics and endogenous hormones into water-soluble metabolites that can be excreted in bile and urine. "Liver cleansing" as a clinical concept is not the vague detox-tea marketing claim; it is a set of well-defined biochemical interventions that support Phase I (cytochrome P450) and Phase II (glucuronidation, sulfation, glutathione conjugation) detoxification pathways, restore bile flow, replenish glutathione, and reduce hepatic inflammation. The four deep-dive pages below explore the evidence-based interventions: TUDCA and bile-flow normalization (the missing third phase of detoxification), castor oil packs (traditional but with emerging mechanistic support), coffee's paradoxical hepatoprotective effects (lower cirrhosis, HCC, and ALT documented across more than 30 cohort studies), and glutathione precursor strategies (NAC, glycine, whey, and the often-overlooked role of selenium and B-vitamins).
Deep-Dive Articles
Bile Flow and TUDCA
Why bile flow is the often-forgotten third phase of detoxification, the enterohepatic circulation and why constipated patients reabsorb their own conjugated toxins, tauroursodeoxycholic acid (TUDCA) for cholestasis and primary biliary cholangitis, ursodeoxycholic acid (UDCA) as the FDA-approved parent compound, bile acid composition shifts in liver disease, and the practical dosing of TUDCA (250-1000 mg/day) for sluggish bile flow and gallstone-prone gallbladders.
Castor Oil Packs
The traditional Edgar Cayce protocol and its modern reappraisal: ricinoleic acid as an EP3 prostaglandin receptor agonist, lymphatic drainage effects measured in vagal-tone studies, the constipation-and-bile-flow effect documented in elderly RCTs, the transdermal delivery question (does it actually penetrate?), the contraindications (pregnancy, active GI bleeding), and the practical how-to: cold-pressed hexane-free oil, organic cotton or wool flannel, low-heat application 60-90 minutes, 3-4 nights weekly.
Coffee and Liver
The paradox: coffee, often viewed as a stressor, is one of the most consistently hepatoprotective beverages on record. Meta-analyses showing dose-dependent reduction in cirrhosis (40% per cup), hepatocellular carcinoma (40% lower at 2+ cups/day), NAFLD progression, and ALT/GGT levels; mechanism via cafestol/kahweol induction of Phase II enzymes, chlorogenic acid antioxidant effects, and adenosine receptor modulation; the filtered-versus-unfiltered question (cafestol cholesterol effect); and the practical recommendation: 2-3 cups/day filtered coffee for adults without contraindications.
Glutathione Support
Glutathione (GSH) is the master antioxidant and the obligate cofactor for Phase II conjugation of acetaminophen, aflatoxin, mercury, and lipid peroxides. Why oral GSH itself is poorly absorbed but precursors (NAC, glycine, glutamine) and cofactors (selenium, riboflavin) reliably restore tissue GSH; the GlyNAC trial in aging adults showing 71% rise in red-blood-cell GSH; the role of milk thistle (silymarin) as a glutathione-sparing agent; and the practical glutathione-restoration protocol: 600-1800 mg/day NAC + 3 g/day glycine + 200 mcg selenomethionine + B2/B6/B12.
Table of Contents
- Deep-Dive Articles
- Why "Liver Cleansing" Has a Real Biochemical Meaning
- The Three Phases of Detoxification
- Research Papers: Bile Flow & TUDCA
- Research Papers: Castor Oil Packs
- Research Papers: Coffee & Liver
- Research Papers: Glutathione Support
- Research Papers: Cross-Cutting (Phase I/II, NAFLD, Hepatoprotection)
- External Authoritative Resources
- Connections
- Featured Videos
Why "Liver Cleansing" Has a Real Biochemical Meaning
The phrase "liver cleanse" attracts justified skepticism because it has been hijacked by detox-tea marketing and the "liver flush" home remedies (large doses of olive oil and Epsom salts producing "stones" that are actually saponified bile-oil pellets, not gallstones). But a separate, legitimate clinical framework exists under the same name — the support of hepatic biotransformation, bile flow, and glutathione status in patients with documented sluggish detoxification, NAFLD, environmental chemical burden, or recovery from acute hepatotoxic exposure.
The liver is the central organ of xenobiotic metabolism. Every drug, every environmental chemical, every endogenous steroid hormone, and every gut-derived metabolite ultimately passes through hepatic biotransformation. The system has three sequential phases — oxidation, conjugation, and excretion — and a bottleneck at any phase produces clinical symptoms ranging from estrogen-dominance acne to multiple chemical sensitivity to drug-induced liver injury.
The four interventions explored in the deep-dive pages below each target a specific phase or substrate:
- TUDCA and bile flow — addresses the Phase III excretion bottleneck. Conjugated toxins leave the hepatocyte in bile; if bile flow is sluggish, conjugates back up into circulation.
- Castor oil packs — a traditional intervention with modern mechanistic support for lymphatic drainage and bile-flow stimulation via ricinoleic acid's EP3 receptor activity.
- Coffee — a dietary intervention with the largest population-scale evidence base for hepatoprotection, working through Phase II enzyme induction and anti-fibrotic effects.
- Glutathione precursor support — addresses the Phase II conjugation bottleneck. Glutathione is the limiting substrate for conjugation of many lipophilic toxins.
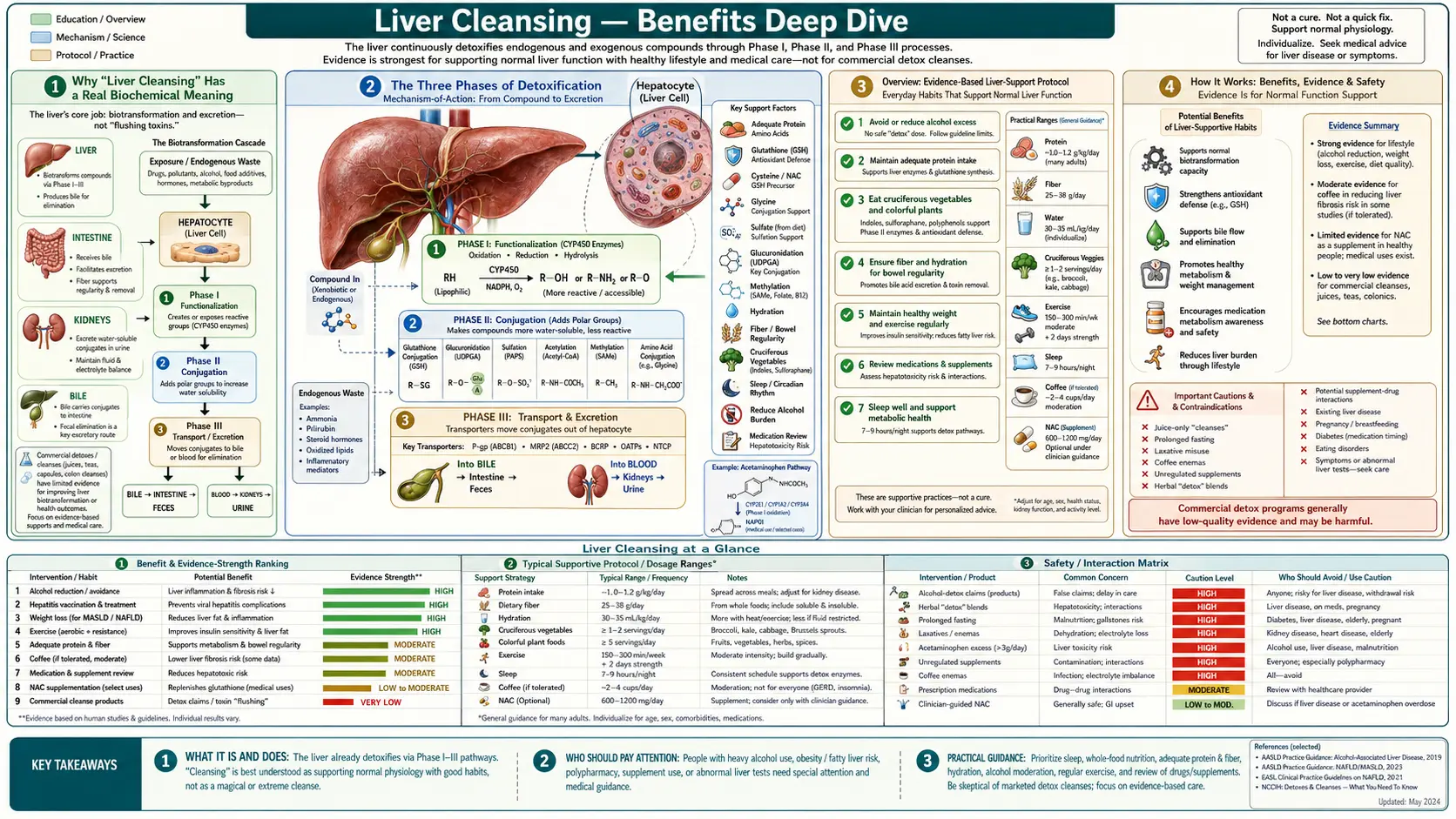
The Three Phases of Detoxification
Hepatic biotransformation is conventionally divided into three sequential phases. Each phase has its own enzymes, cofactors, substrate preferences, and clinically relevant bottlenecks.
Phase I — Functionalization (Cytochrome P450). The CYP450 enzyme superfamily (approximately 57 functional human enzymes; CYP3A4, CYP2D6, CYP2C9, CYP1A2 do most of the work) introduces or unmasks a polar functional group on the substrate (typically a hydroxyl). The reaction generates reactive intermediates that are more toxic than the parent compound in many cases — acetaminophen's NAPQI metabolite, benzo[a]pyrene's diol-epoxide, and aflatoxin's 8,9-epoxide are all Phase I products more dangerous than their precursors. Phase I requires NADPH (from the pentose phosphate pathway), riboflavin (FAD), and iron (heme prosthetic group).
Phase II — Conjugation. The Phase II reactions attach a polar group (glucuronate, sulfate, glutathione, acetyl, methyl, glycine) to the Phase I product, converting the reactive intermediate to a water-soluble, biologically inert conjugate ready for excretion. The major Phase II pathways and their cofactors:
- Glucuronidation — UGT enzymes attach glucuronic acid from UDP-glucuronate. Requires intact glucose metabolism. Handles bilirubin, opioids, NSAIDs, many drug metabolites.
- Sulfation — SULT enzymes attach sulfate from PAPS (3'-phosphoadenosine-5'-phosphosulfate). Limited by dietary sulfur (cysteine, methionine, MSM). Handles many steroid hormones, phenols.
- Glutathione conjugation — GST enzymes attach glutathione directly. Critical for acetaminophen detoxification, heavy metal binding, lipid peroxide cleanup. Discussed in depth in the glutathione deep-dive.
- Methylation — SAM-dependent transfer of methyl groups; depends on folate, B12, B6, betaine.
- Acetylation — NAT enzymes; subject to fast/slow acetylator genetic polymorphism.
- Amino-acid conjugation — glycine and glutamine conjugation; depends on dietary glycine.
Phase III — Excretion. Conjugates must leave the hepatocyte. Active transport via MRP2, P-glycoprotein, and BCRP transporters carries conjugates into bile, which carries them to the gut for fecal excretion. If bile flow is sluggish (cholestasis, gallstones, gallbladder removal, opioid use), Phase II conjugates back up into the blood, get deconjugated by intestinal beta-glucuronidase, and recirculate via enterohepatic circulation. This is why bile-flow support matters as much as Phase I/II enzymes themselves.
Research Papers: Bile Flow & TUDCA
- TUDCA mechanism in cholestatic liver disease (Beuers et al.) — PubMed: TUDCA cholestasis mechanism
- Ursodeoxycholic acid for primary biliary cholangitis — PubMed: UDCA for PBC
- Endoplasmic reticulum stress and TUDCA as a chemical chaperone — PubMed: TUDCA ER stress
- Bile acid composition shifts in liver disease (cholestasis, NAFLD) — PubMed: Bile acid pool
- Enterohepatic circulation and beta-glucuronidase deconjugation — PubMed: Enterohepatic deconjugation
- FXR (farnesoid X receptor) and bile acid signaling — PubMed: FXR signaling
- TGR5 (GPBAR1) receptor and bile acid metabolic effects — PubMed: TGR5 receptor
- Cholestasis-induced hepatocyte apoptosis and TUDCA cytoprotection — PubMed: Cholestasis apoptosis
- Post-cholecystectomy bile dynamics and digestive effects — PubMed: Post-cholecystectomy
- Bile acid sequestrants and serum bile acid pharmacology — PubMed: Bile acid sequestrants
Research Papers: Castor Oil Packs
- Ricinoleic acid as EP3 prostaglandin receptor agonist (Tunaru 2012 PNAS) — PubMed: Ricinoleic EP3 mechanism
- Castor oil pack effects in elderly constipation (Arslan 2011 RCT) — PubMed: Castor oil pack RCT
- Topical ricinoleic acid and anti-inflammatory effects — PubMed: Topical anti-inflammatory
- Lymphatic drainage and abdominal manual therapy — PubMed: Lymphatic drainage
- Vagal tone and parasympathetic activation in topical abdominal therapies — PubMed: Vagal tone
- Castor oil as ancient and traditional remedy historical review — PubMed: Historical castor oil
- Ricinus communis pharmacology and ricin toxicology — PubMed: Ricinus pharmacology
- Cold-pressed vs hexane-extracted oils, contaminant profile — PubMed: Cold-pressed oils
- Heat therapy and visceral blood flow — PubMed: Heat and visceral flow
- Skin absorption of fatty acids and topical penetration — PubMed: Skin penetration
Research Papers: Coffee & Liver
- Coffee consumption and cirrhosis mortality meta-analysis (Kennedy 2016) — PubMed: Coffee and cirrhosis
- Coffee and hepatocellular carcinoma (HCC) risk reduction meta-analysis — PubMed: Coffee and HCC
- Coffee and NAFLD progression — PubMed: Coffee and NAFLD
- Coffee and serum ALT/GGT in epidemiologic studies — PubMed: Coffee and ALT/GGT
- Cafestol and kahweol induction of Phase II enzymes — PubMed: Cafestol/kahweol Phase II
- Chlorogenic acid and hepatic antioxidant effects — PubMed: Chlorogenic acid
- Filtered vs unfiltered coffee and serum cholesterol (cafestol effect) — PubMed: Cafestol cholesterol
- Caffeine adenosine receptor antagonism and hepatic stellate cells — PubMed: Caffeine and stellate cells
- Coffee and hepatic fibrosis in chronic hepatitis C — PubMed: Coffee and HCV fibrosis
- Coffee and gallstone disease risk — PubMed: Coffee and gallstones
Research Papers: Glutathione Support
- GlyNAC trial in aging adults: 71% rise in RBC GSH (Kumar 2021) — PubMed: GlyNAC trial
- N-acetylcysteine for acetaminophen overdose (FDA-approved) — PubMed: NAC for acetaminophen
- Glycine as the rate-limiting amino acid for glutathione synthesis — PubMed: Glycine and GSH synthesis
- Selenium and glutathione peroxidase enzyme activity — PubMed: Selenium and GPx
- Silymarin (milk thistle) and hepatic glutathione preservation — PubMed: Silymarin GSH
- Oral glutathione bioavailability and liposomal forms — PubMed: Oral GSH bioavailability
- Sublingual and intravenous glutathione pharmacokinetics — PubMed: GSH pharmacokinetics
- Glutathione depletion in NAFLD and chronic liver disease — PubMed: GSH depletion in liver disease
- NAC and idiosyncratic drug-induced liver injury (DILI) — PubMed: NAC and DILI
- Cysteine availability and rate-limiting role in GSH synthesis — PubMed: Cysteine and GSH
Research Papers: Cross-Cutting (Phase I/II, NAFLD, Hepatoprotection)
- Cytochrome P450 induction and inhibition by dietary phytochemicals — PubMed: CYP450 dietary
- Cruciferous vegetables and Phase II enzyme induction (sulforaphane) — PubMed: Sulforaphane and Nrf2
- Nrf2/Keap1 pathway as master regulator of antioxidant response — PubMed: Nrf2/Keap1
- NAFLD prevalence and current management guidelines — PubMed: NAFLD management
- Methionine cycle, SAM, homocysteine and hepatic methylation — PubMed: Methionine cycle
- Choline deficiency and fatty liver pathogenesis — PubMed: Choline and fatty liver
- Berberine for NAFLD and metabolic syndrome — PubMed: Berberine for NAFLD
- Vitamin E (mixed tocopherols) for biopsy-proven NASH — PubMed: Vitamin E for NASH
- Gut-liver axis: dysbiosis, LPS endotoxemia, and hepatic inflammation — PubMed: Gut-liver axis
- Alcohol metabolism, ALDH2 polymorphism, and hepatic toxicity — PubMed: ALDH2 polymorphism
External Authoritative Resources
- AASLD — American Association for the Study of Liver Diseases Practice Guidelines
- NIDDK — Liver Disease Information
- Linus Pauling Institute — Phytochemicals and Detoxification
- LiverTox (NIH) — Drug-Induced Liver Injury Database
- PubMed — Liver detoxification & hepatoprotection
Connections
- Liver Cleansing (Main Page)
- Bile Flow and TUDCA
- Castor Oil Packs
- Coffee and Liver
- Glutathione Support
- All Remedies
- Milk Thistle (Silymarin)
- N-Acetyl-Cysteine (NAC)
- Glycine
- Selenium
- NAFLD (Non-Alcoholic Fatty Liver Disease)
- Gallstones
- Heavy Metals
- Coffee