Liver Cleansing — Glutathione Support
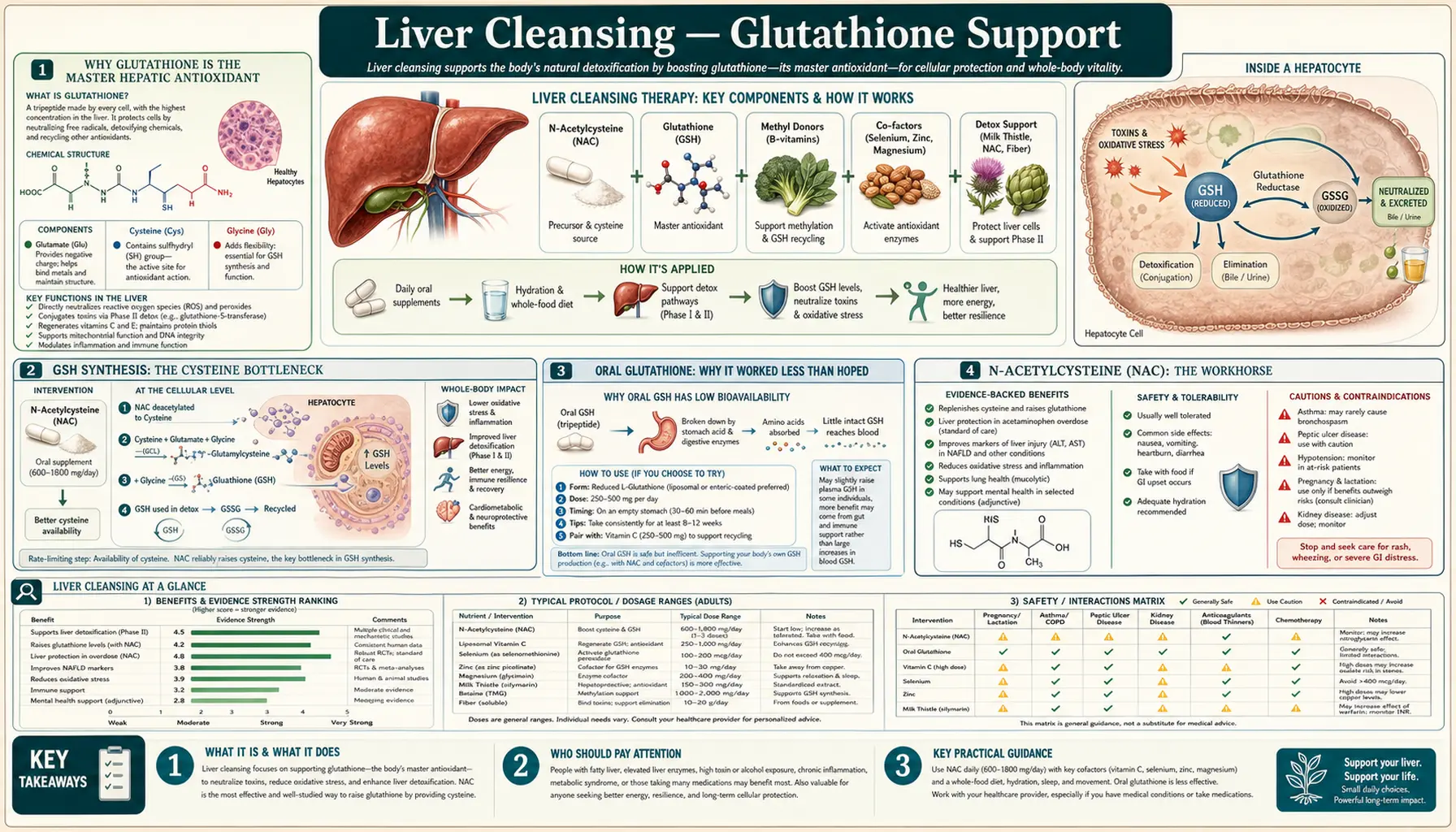
Glutathione (gamma-glutamyl-cysteinyl-glycine, GSH) is the master antioxidant and the obligate cofactor for Phase II conjugation of acetaminophen, aflatoxin, mercury, lipid peroxides, and many environmental electrophiles. The liver maintains the highest glutathione concentration of any organ (5-10 mM intracellularly), and depletion of hepatic glutathione is the central event in acetaminophen-induced acute liver failure, the leading cause of acute liver failure in the U.S. The classic finding that oral glutathione is poorly absorbed (it is hydrolyzed in the gut before reaching the portal circulation) is partially true but has been substantially revised by recent liposomal and sublingual formulation studies. The reliable approach is supplying precursors and cofactors: N-acetylcysteine (NAC) for the cysteine moiety (typically rate-limiting), glycine (rate-limiting in aging), and selenium for the glutathione peroxidase enzyme that uses GSH as substrate. The GlyNAC trial in aging adults raised red-blood-cell glutathione by 71% in 16 weeks — the largest oral-supplement-driven GSH increase ever documented.
Table of Contents
- Why Glutathione Is the Master Hepatic Antioxidant
- GSH Synthesis: The Cysteine Bottleneck
- Oral Glutathione: Why It Worked Less Than Hoped
- N-Acetylcysteine (NAC): The Workhorse
- The GlyNAC Trial: 71% RBC GSH Increase
- Cofactors: Selenium, Riboflavin, B6, B12
- Milk Thistle (Silymarin) as Glutathione-Sparing
- Liposomal, Sublingual, and IV Glutathione
- A Practical Restoration Protocol
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Why Glutathione Is the Master Hepatic Antioxidant
Glutathione is a tripeptide of glutamate, cysteine, and glycine. The unusual gamma-glutamyl bond (rather than the standard peptide bond between glutamate's alpha-carboxyl and the next amino acid's amino group) makes glutathione resistant to most peptidases. It is synthesized intracellularly in nearly every human cell, with the liver as the primary biosynthetic site and net exporter to other tissues via the gamma-glutamyl cycle.
Glutathione's central role rests on its cysteine sulfhydryl (-SH) group. The thiol is a potent reducing agent (GSH/GSSG redox potential is -240 mV), making glutathione the dominant intracellular reductant in animal cells. The thiol participates in:
- Direct reduction of reactive oxygen species — hydrogen peroxide, organic hydroperoxides, and lipid peroxides are reduced to water or alcohol, with glutathione oxidized to GSSG (glutathione disulfide). The GSH/GSSG ratio (normally 100:1 in cytoplasm) is a sensitive index of oxidative stress.
- Phase II conjugation of electrophiles — glutathione S-transferase (GST) enzymes catalyze conjugation of glutathione with reactive electrophiles, neutralizing them. Acetaminophen's reactive metabolite NAPQI, aflatoxin B1's 8,9-epoxide, mercury, organophosphates, and many environmental chemicals are detoxified by this mechanism.
- Protein S-glutathionylation — reversible modification of cysteine residues on regulatory proteins, a major redox signaling mechanism
- Recycling of vitamin C and vitamin E — glutathione reduces oxidized ascorbate and tocopheryl radicals, regenerating the antioxidant pool
- Mercury and heavy-metal binding — glutathione-mercury complexes are the major export route for mercury via bile
The hepatic glutathione pool is approximately 5-10 mM intracellular concentration, with a total liver content of about 1-2 grams in an adult. Plasma glutathione concentrations are about 10,000-fold lower (around 5 micromolar) because GSH is rapidly metabolized in extracellular space — this is why direct measurement of plasma glutathione is a poor indicator of tissue stores.
The fasting hepatic glutathione content is depleted by approximately 30% after an overnight fast and rapidly replenished with feeding. Hepatic glutathione is depleted by approximately 70-90% in acute acetaminophen overdose; depletion below 30% of normal triggers hepatocyte necrosis. This is the basis of NAC's use as the FDA-approved antidote for acetaminophen poisoning.
GSH Synthesis: The Cysteine Bottleneck
Glutathione is synthesized in two ATP-requiring steps:
- Glutamate + cysteine → gamma-glutamyl-cysteine — catalyzed by glutamate-cysteine ligase (GCL, formerly gamma-glutamylcysteine synthetase). This is the rate-limiting step, regulated by feedback inhibition from GSH itself and by substrate availability (cysteine is typically the limiting amino acid).
- Gamma-glutamyl-cysteine + glycine → glutathione — catalyzed by glutathione synthetase. Not normally rate-limiting in young adults but can become limiting in aging and in conditions with low glycine intake.
The cysteine bottleneck is the central practical issue in glutathione restoration. Cysteine is a sulfur-containing amino acid that can be either consumed directly in the diet (whey protein and animal protein sources) or synthesized from methionine via the transsulfuration pathway (methionine → SAM → SAH → homocysteine → cystathionine → cysteine, requiring vitamin B6 and serine). Free cysteine itself is unstable and somewhat cytotoxic; the body tightly regulates intracellular free cysteine concentration, which limits how much glutathione synthesis can be driven by simple cysteine supplementation.
N-acetylcysteine (NAC) is the workaround — the N-acetyl group is removed inside the cell, releasing cysteine in a more regulated manner than free cysteine would provide. This is why NAC, not cysteine, is the standard precursor used in hepatic medicine.
The glycine arm is generally considered non-limiting in most adults, but the GlyNAC research has called this assumption into question for older adults, where glycine supplementation alongside NAC produces synergistic glutathione restoration that NAC alone does not.
Oral Glutathione: Why It Worked Less Than Hoped
The conventional teaching for decades was that oral glutathione is useless because it is hydrolyzed in the gastrointestinal tract before reaching the portal circulation. This was based on early pharmacokinetic studies showing minimal increase in plasma glutathione after oral dosing of free reduced GSH.
The more nuanced reality:
- Plasma glutathione is the wrong endpoint — plasma GSH is rapidly degraded by gamma-glutamyl transpeptidase (GGT) on cell membranes, regardless of source. The relevant question is whether tissue glutathione (especially hepatic and red-blood-cell glutathione) increases.
- Tissue GSH does respond modestly — Richie 2015 showed that 1 g/day of oral reduced glutathione for 6 months increased erythrocyte glutathione by approximately 30% and natural killer cell function by approximately 50%. Smaller effects, but real.
- Liposomal encapsulation substantially improves bioavailability — the GSH is protected from gastric hydrolysis and absorbed intact via lymphatic uptake. Sinha 2018 showed liposomal GSH (500-1000 mg/day for 4 weeks) increased intracellular GSH in lymphocytes by 100-400%.
- Sublingual GSH — bypasses gut hydrolysis. Available as troches and dissolvable tablets at 100-200 mg doses. Pharmacokinetic data are limited but suggest meaningful absorption.
- The precursor approach (NAC + glycine + cofactors) is still cheaper and more reliable — oral glutathione products are expensive ($30-60/month for liposomal). NAC + glycine + selenium produces comparable or superior tissue glutathione increases for under $20/month.
Oral glutathione is not useless, but it is generally not the most cost-effective route to higher tissue glutathione. The precursor strategy is the first-line approach.
N-Acetylcysteine (NAC): The Workhorse
N-acetylcysteine is the most extensively studied glutathione precursor and an FDA-approved drug (the IV formulation Acetadote for acetaminophen overdose; the inhaled and oral formulations Mucomyst, Acetylcysteine for mucolysis and various off-label uses). Mechanism: oral NAC is deacetylated in enterocytes and hepatocytes, releasing cysteine for glutathione synthesis.
Dosing for hepatic glutathione support:
- 600 mg twice daily — the standard "wellness" dose, well tolerated, modestly raises tissue glutathione over 4-8 weeks
- 1800 mg/day divided — higher-dose protocol used in some integrative medicine practices for active liver-cleansing or post-toxic-exposure recovery
- Acute acetaminophen overdose (in-hospital) — the IV protocol delivers 150 mg/kg loading dose followed by 50 mg/kg over 4 hours then 100 mg/kg over 16 hours, or the simpler 21-hour regimen. This is the clinical pharmacology that demonstrated NAC's definitive efficacy.
NAC has documented benefits for:
- Acetaminophen overdose — FDA-approved indication, mortality reduction from approximately 5% to less than 1% when given within 8-10 hours of overdose
- Chronic obstructive pulmonary disease — reduces exacerbations as a mucolytic and antioxidant
- Polycystic ovary syndrome — improves insulin sensitivity and ovulation rates
- Obsessive-compulsive disorder and trichotillomania — modulates glutamatergic neurotransmission
- Non-alcoholic steatohepatitis — small trials show improvement in liver enzymes and histology
- Drug-induced liver injury — case-series evidence for non-acetaminophen DILI (anti-tuberculosis drugs, methotrexate)
Side effects are minimal at oral doses. The IV formulation can cause anaphylactoid reactions in 5-10% of recipients. Oral NAC has a sulfur smell that some patients find off-putting; capsule formulations minimize this.
The GlyNAC Trial: 71% RBC GSH Increase
The most important glutathione restoration study in recent years is the Kumar et al. 2021 GlyNAC trial, published in Clinical and Translational Medicine. The investigators (Baylor College of Medicine) randomized older adults (age 70-80) to receive glycine (1.33 mmol/kg/day) plus N-acetylcysteine (0.81 mmol/kg/day) or placebo, for 16 weeks.
Results in the GlyNAC arm versus placebo:
- Red blood cell glutathione increased by 71% (the primary endpoint)
- Plasma oxidative stress markers (F2-isoprostanes) decreased by 59%
- Plasma inflammation markers (IL-6, TNF-alpha, CRP) decreased significantly
- Insulin sensitivity (HOMA-IR) improved by 23%
- Mitochondrial function (PBMC ATP production) improved
- Endothelial function improved (flow-mediated dilation)
- Body composition improved (waist circumference decreased)
- Strength and gait speed improved
- Cognitive function improved (executive function tests)
The size of the GSH response (71% increase in RBC glutathione) is the largest documented for any oral supplement intervention. The clinical effects beyond GSH itself — insulin sensitivity, inflammation, mitochondrial function, cognition — map onto the constellation of changes that characterize biological aging.
The key insight from GlyNAC is that both glycine and NAC are needed. Earlier studies of NAC alone in aging produced modest GSH increases; earlier studies of glycine alone produced modest effects. The combination is synergistic because aging produces deficits in both the cysteine arm (driven by reduced dietary cysteine intake and reduced transsulfuration efficiency) and the glycine arm (driven by reduced dietary glycine intake; modern industrial diets are low in collagen and connective tissue, the main glycine sources).
Practical translation: for adults over 60 with concerns about aging, recurrent illness, or compromised liver function, a daily regimen of 1200-1800 mg NAC + 3-5 g glycine is the closest available approximation to the GlyNAC protocol. Cost is approximately $15-25 per month.
Cofactors: Selenium, Riboflavin, B6, B12
Glutathione without its supporting cofactors is incomplete. The key cofactors:
- Selenium — obligate cofactor for glutathione peroxidase (GPx), the enzyme that uses GSH to reduce hydrogen peroxide and lipid peroxides. Selenium is incorporated as selenocysteine into the GPx active site. Without adequate selenium, GSH cannot be deployed by GPx and accumulates uselessly while peroxide-driven oxidative stress continues. Dose: 100-200 mcg/day from selenomethionine or selenium yeast. The U.S. RDA is 55 mcg/day; functional repletion typically uses higher doses. Avoid exceeding 400 mcg/day chronically.
- Riboflavin (vitamin B2) — cofactor for glutathione reductase, the enzyme that recycles GSSG back to GSH using NADPH. Mild riboflavin deficiency reduces GSH/GSSG ratio. Dose: 25-50 mg/day. See our Vitamin B2 page.
- Vitamin B6 (pyridoxal 5-phosphate) — cofactor for cystathionine beta-synthase and cystathionase, the transsulfuration enzymes that produce cysteine from methionine. B6 deficiency can limit cysteine supply for glutathione synthesis.
- Vitamin B12 and folate — required for the methionine cycle that ultimately feeds the transsulfuration pathway. Functional B12 or folate deficiency impairs methionine availability and indirectly impairs cysteine and glutathione synthesis.
- Magnesium — cofactor for glutamate-cysteine ligase (GCL), the rate-limiting enzyme of GSH synthesis. Magnesium deficiency is associated with reduced hepatic GSH in animal models.
- NADPH — the obligate electron donor for glutathione reductase, generated primarily by the pentose phosphate pathway. NADPH availability depends on glucose-6-phosphate dehydrogenase activity and pentose phosphate pathway throughput.
The combined supplementation approach: NAC + glycine + 100-200 mcg selenomethionine + a B-complex providing 25-50 mg of B2/B6 and methylcobalamin/methylfolate addresses the full pathway in a way that any single supplement cannot.
Milk Thistle (Silymarin) as Glutathione-Sparing
Silymarin, the standardized extract of Silybum marianum, is the most-studied hepatoprotective herbal medicine. Its mechanism is multimodal — antioxidant, anti-fibrotic, membrane-stabilizing, and pro-regenerative — but one key mechanism is glutathione-sparing. Silymarin reduces the rate of glutathione consumption during oxidative stress by directly scavenging reactive species before they can react with GSH, and indirectly by stabilizing hepatocyte membranes and reducing the cellular damage that depletes GSH.
In animal models of carbon tetrachloride, acetaminophen, and ethanol-induced hepatotoxicity, silymarin pretreatment preserves hepatic glutathione despite ongoing toxicant exposure. In human studies of chronic hepatitis C and alcohol-related liver disease, silymarin reduces transaminase elevations and may slow fibrosis progression.
The standard dose is 420 mg/day of silymarin (typically delivered as 140 mg three times daily of a standardized extract containing approximately 80% silymarin). For practical clinical use, the combination of milk thistle + NAC + glycine + selenium provides multimodal coverage: the herb stabilizes hepatocyte membranes and scavenges reactive species; NAC and glycine replenish the precursor pool; selenium activates the deployable peroxidase. See our Milk Thistle page for the full pharmacology.
Liposomal, Sublingual, and IV Glutathione
Beyond precursor supplementation, several direct glutathione delivery routes are available:
- Liposomal glutathione (oral) — reduced glutathione encapsulated in phosphatidylcholine liposomes that protect it from gastric hydrolysis and deliver it to enterocytes intact. The Sinha 2018 RCT (90 days, 500-1000 mg/day) showed substantial increases in lymphocyte intracellular GSH, NK cell activity, and reductions in 8-iso-prostaglandin F2-alpha. Cost: $30-60/month. Reasonable for patients who do not tolerate NAC or who want belt-and-suspenders coverage.
- Sublingual glutathione — troches or rapidly dissolving tablets at 100-200 mg per dose. Bypasses gastric hydrolysis but absolute bioavailability is uncertain. Less expensive than liposomal.
- Intravenous glutathione — 600-2400 mg pushed slowly over 5-15 minutes. Bypasses absorption questions entirely. Used in some integrative practices for acute toxic exposures, Parkinson's disease (modest evidence), and chronic fatigue. Not FDA-approved for any indication; insurance does not cover. Cost: $50-150 per IV session.
- Inhaled glutathione — nebulized GSH (typically 600 mg) delivers GSH directly to the respiratory epithelium. Some evidence in cystic fibrosis and chronic respiratory inflammation. Off-label use.
- Transdermal glutathione — creams marketed for skin and systemic absorption. The skin penetration of intact GSH is minimal; these products are mostly marketing.
A Practical Restoration Protocol
A reasonable consolidated regimen for an adult wanting to restore hepatic glutathione and Phase II detoxification capacity:
- NAC 600 mg twice daily with meals — the foundation
- Glycine 3 grams twice daily — convenient as glycine powder dissolved in water; sweet-tasting and pleasant
- Selenomethionine 100-200 mcg/day — or 2-3 Brazil nuts daily as food source (each contains approximately 70-90 mcg)
- A high-quality B-complex daily — providing methylated B12, methylfolate, P5P (active B6), and riboflavin
- Milk thistle 420 mg/day — standardized silymarin extract, especially during periods of higher hepatic stress (alcohol exposure, medication, environmental exposure)
- Magnesium glycinate 400 mg at bedtime — supplies both the magnesium cofactor and additional glycine; promotes sleep, which itself supports glutathione recycling
- Whey protein concentrate (undenatured) 20-30 g/day — rich source of cysteine in the alpha-lactalbumin and bovine serum albumin fractions, plus a major source of glutamate. Whey is unusually effective at raising tissue glutathione in comparison to other protein sources.
- Cruciferous vegetables 1+ cups daily — sulforaphane induces Nrf2 and glutathione S-transferase expression, increasing the effective deployment of glutathione for conjugation. See Cruciferous Vegetables page.
- Filtered coffee 2-3 cups/day — for Phase II enzyme induction via cafestol/kahweol, as discussed in the Coffee deep-dive
- Reassess at 8-12 weeks — clinical improvement (energy, sleep, skin, digestion) and lab markers (ALT, GGT, fasting glucose) provide feedback. Some clinicians measure RBC glutathione directly via specialty labs.
Cost of the full regimen: approximately $40-60 per month for the supplements. The whey protein, cruciferous vegetables, and coffee are food costs that overlap with general nutrition.
Cautions and Drug Interactions
- NAC and nitroglycerin — NAC potentiates nitroglycerin's vasodilatory effect and can produce severe hypotension and headache. Avoid combination.
- NAC and asthma — rare paradoxical bronchospasm with nebulized NAC. Oral form generally well tolerated even in asthmatics.
- NAC and bleeding — NAC has mild antiplatelet effects at high doses; theoretical interaction with anticoagulants. Generally well tolerated even with warfarin or DOACs at standard 600 mg BID dosing.
- Glycine and clozapine — high-dose glycine (20-30 g/day for schizophrenia research) reduces clozapine efficacy. Routine 3-5 g/day glycine for GSH support is unlikely to cause clinically significant interaction.
- Selenium upper limit — tolerable upper intake limit is 400 mcg/day. Chronic intake above 800-1000 mcg/day produces selenium toxicity (hair loss, nail brittleness, garlic breath, neuropathy). Do not stack a selenium supplement with daily multiple Brazil nuts without thinking through total intake.
- Liposomal GSH and shellfish allergy — some liposomal preparations use sunflower-derived phosphatidylcholine; others use soy or marine sources. Read labels if you have severe allergies.
- Pregnancy — NAC has been used in pregnancy for acetaminophen overdose with apparent safety. Routine high-dose glutathione precursor supplementation in pregnancy lacks rigorous safety data; defer to obstetric supervision.
- Acetaminophen overdose requires emergency care, not supplements — the IV NAC protocol must be initiated within 8-10 hours of overdose ingestion for full mortality benefit. Suspected overdose is an emergency department visit, not a home-supplement problem.
Key Research Papers
- Kumar P et al. (2021). Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition. Clin Transl Med. — PubMed
- Prescott LF et al. (1979). Intravenous N-acetylcysteine: the treatment of choice for paracetamol poisoning. BMJ. (classic protocol study) — PubMed
- Richie JP et al. (2015). Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. Eur J Nutr. — PubMed
- Sinha R et al. (2018). Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. Eur J Clin Nutr. — PubMed
- Lu SC (2013). Glutathione synthesis. Biochim Biophys Acta. — PubMed
- Sekhar RV et al. (2011). Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. Am J Clin Nutr. — PubMed
- Saller R et al. (2008). The use of silymarin in the treatment of liver diseases. Drugs. — PubMed
- Brigelius-Flohe R (2006). Glutathione peroxidases and redox-regulated transcription factors. Biol Chem. (selenium-GPx mechanism) — PubMed
- Mischley LK et al. (2017). Phase IIb study of intranasal glutathione in Parkinson's disease. J Parkinsons Dis. — PubMed
- Atkuri KR et al. (2007). N-acetylcysteine — a safe antidote for cysteine/glutathione deficiency. Curr Opin Pharmacol. — PubMed
- Bunchorntavakul C, Reddy KR (2018). Acetaminophen (APAP or N-acetyl-p-aminophenol) and acute liver failure. Clin Liver Dis. — PubMed
- Dean O et al. (2011). N-acetylcysteine in psychiatry: current therapeutic evidence and potential mechanisms of action. J Psychiatry Neurosci. — PubMed
PubMed Topic Searches
- PubMed: Glutathione hepatic detoxification
- PubMed: NAC clinical trials
- PubMed: Glycine and GSH synthesis
- PubMed: GPx and selenium
- PubMed: Silymarin hepatoprotection
Connections
- Liver Cleansing Hub
- Benefits Deep Dive Hub
- Bile Flow and TUDCA
- Castor Oil Packs
- Coffee and Liver
- N-Acetyl-Cysteine (NAC)
- Glycine
- Cysteine
- Glutamine
- Selenium
- Vitamin B2 (Riboflavin)
- Milk Thistle (Silymarin)
- NAFLD
- Mercury