Elimination Diet: History and Origins
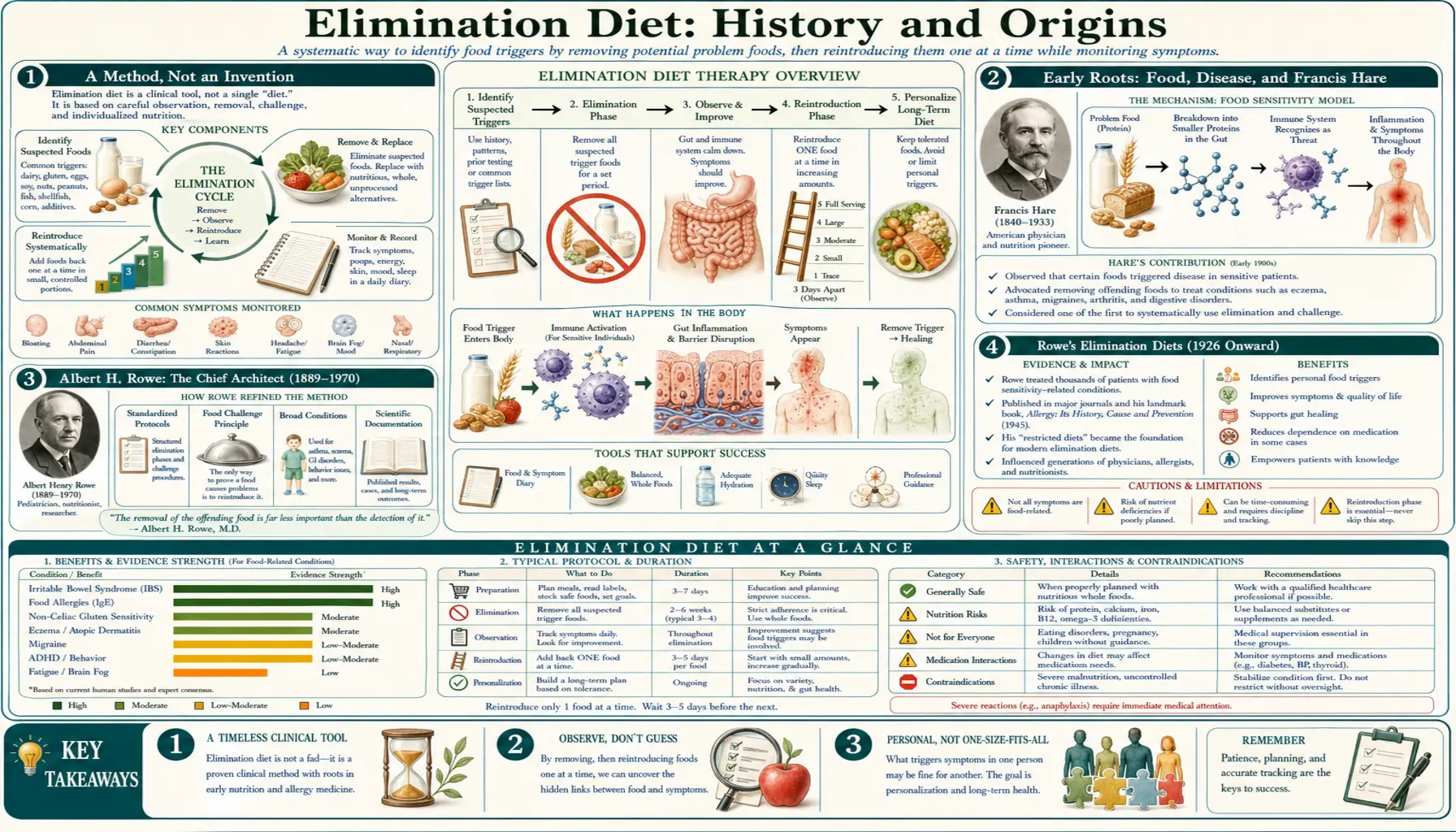
The elimination diet has no single inventor — it is a method, not a product, and like most clinical methods it was built up over a century by many hands. But its modern form does have a clear chief architect: Dr. Albert H. Rowe (1889–1970), an Oakland, California allergist who, beginning in 1926, turned a loose idea — remove the suspect foods, watch the patient improve, then add foods back one at a time — into a documented, named diagnostic procedure. This article traces what the historical record actually supports: the nineteenth- and early-twentieth-century roots in food-and-disease theory (including the Irish physician Francis Hare), Rowe's biography and the formal "elimination diets" he published, how the method spread and split into the variants used today (the Australian RPAH food-chemical diet, low-FODMAP, and consumer programs), and — just as important — how mainstream allergy and immunology now judge it. Where the record is firm we say so; where a claim is disputed, unproven, or rejected by professional bodies, we say that plainly. Truth comes before promotion here.
Table of Contents
- A Method, Not an Invention
- Early Roots: Food, Disease, and Francis Hare
- Albert H. Rowe: The Chief Architect (1889–1970)
- Rowe's Elimination Diets (1926 Onward)
- Spread, Controversy, and the Mid-Century Debate
- The Method Splits: RPAH, FODMAP, and Consumer Diets
- Evidence and Reception Today
- Honest Takeaways
- Research Papers and References
- Connections
- Featured Videos
A Method, Not an Invention
It is worth being clear at the outset about what kind of thing the elimination diet is. It is not a drug, a supplement, or a branded product with a patent and an inventor. It is a diagnostic procedure — a structured way of using the body itself as the test instrument. You remove a set of suspected foods, you wait for symptoms to settle, and then you reintroduce foods one at a time and watch what happens. Because it is a method rather than a substance, its history is the history of an idea being refined, formalised, named, argued over, and eventually folded into mainstream medicine in some forms while being firmly rejected in others.
That shape — many contributors, one chief organiser — is common in the history of clinical practice. The closest thing to a "founder" is Albert H. Rowe, the Oakland allergist who is consistently credited with proposing the formal elimination diet in 1926 and who spent the rest of his career systematising it. But Rowe did not work in a vacuum: he was reacting to a body of earlier nineteenth- and early-twentieth-century thinking about food and chronic illness, and the method he started has since branched into several distinct protocols developed by other people in other countries. This page gives Rowe his due as the central figure while being honest that the elimination diet, like the practice of medicine itself, was a collective achievement.
Early Roots: Food, Disease, and Francis Hare
Long before anyone spoke of "elimination diets," physicians had noticed that some chronic complaints eased when particular foods or drinks were withdrawn. One of the most ambitious early attempts to systematise that observation came from the Irish physician Francis Washington Everard Hare (1858–1928), who in 1905 published a sprawling two-volume work, The Food Factor in Disease. Hare had observed that complaints such as migraine improved when patients were placed on restricted diets that cut certain foods and alcohol, and he argued — far too broadly — that a long list of conditions (migraine, asthma, gout, hypertension, obesity, epilepsy, dyspepsia, eczema, and more) stemmed from an altered reaction to food, which he attributed to a state he called "hyperpyraemia," supposedly caused by excess carbohydrate.
Hare belongs in this history because he was among the first to insist, in print, that unexplained chronic illness might be driven by what people ate, and to try to argue it as science rather than folk wisdom. But honesty requires the rest of the story: mainstream medicine rejected his central theory. A 1906 review in the British Medical Journal concluded that "we cannot regard the theory of hyperpyraemia as possessing any sound basis," and other journals of the day made the same point — the proposed mechanism had no chemical evidence behind it. So Hare is best understood not as a proven pioneer but as an early, partly-wrong forerunner: he pointed at the right phenomenon (food can drive chronic symptoms) while explaining it with a mechanism that did not survive scrutiny. The lasting contribution of this era was the question, not the answer.
This pattern — a clinician noticing a real effect, then over-reaching to a sweeping theory that the evidence cannot support — recurs throughout the elimination diet's history, and it is exactly why the careful, food-by-food testing that came next mattered so much.
Albert H. Rowe: The Chief Architect (1889–1970)
Albert H. Rowe was born in 1889 and earned his medical degree from the University of California, San Francisco, in 1914. According to the archival record of his papers (held by the University of California, Davis), he joined the staff of Merritt Hospital in Oakland, California, around 1916 and practised there for the rest of his long career, also lecturing at UCSF. He devoted roughly six decades to the treatment of allergy, building one of the country's best-known allergy clinics and dying in 1970.
There is a striking personal thread in Rowe's story that is frequently noted in biographical accounts: after finishing medical school he himself developed ulcerative colitis, and his effort to understand and manage his own illness is described as part of what drew him into allergy and the study of food reactions. Whether or not one reads that as the decisive spark, it fits the man the record describes — a physician unusually willing to treat diet as a serious clinical variable at a time when his specialty was increasingly defined by skin testing.
Rowe's importance rests on more than the diet plans themselves. He was an early and persistent advocate of the idea — ordinary today, contested then — that food reactions need not be classic immediate allergies to matter clinically, and that a structured diet could reveal foods contributing to chronic, hard-to-pin-down disease. He laid this out at length in his books, including Food Allergy: Its Manifestations, Diagnosis and Treatment (1931) and, most famously, Elimination Diets and the Patient's Allergies (first edition 1941; a revised edition followed in 1944). It is this body of work that earns him the label of chief architect of the modern elimination diet.
Rowe's Elimination Diets (1926 Onward)
Rowe is credited with first proposing the formal elimination diet in 1926. His motivation was practical and, in hindsight, prescient: he distrusted the cutaneous (scratch) skin tests of his era for food allergy, observing that they produced frequent false-negative results and that a patient's real-world symptoms often failed to match the test outcome. Rather than trust an unreliable test, he proposed letting the body answer the question directly — remove the likely offenders until the patient is symptom-free, then reintroduce foods one at a time and watch for the symptoms to return. That two-phase logic — elimination, then deliberate reintroduction — is the procedure people still follow today, and it is essentially Rowe's.
Rowe was also methodical to the point of severity about compliance, because he understood that a single hidden exposure could ruin the whole experiment. Historical accounts describe him insisting on detailed patient interviews and on near-total control of ingredients — to the point of advising that a physician might even watch a patient's baker prepare bread, and that patients bring their own oils, breads, and baked goods when eating away from home. He paired this rigour with a genuine concern for nutrition, stressing that whatever foods were removed had to be nutritionally replaced so the diet did not harm the patient — a caution that remains central to safe elimination dieting.
It is worth noting how Rowe's stance read at the time. The medical historian Matthew Smith has observed that to reject skin testing in favour of patient-driven dietary diagnosis was, in that era, almost to "sever the link between allergy and legitimate science," setting Rowe somewhat apart from orthodox allergists. The irony is considerable: the very approach that once looked like a step away from rigorous medicine — carefully removing and then challenging foods one at a time — is the logical ancestor of the oral food challenge that mainstream allergy now regards as its diagnostic gold standard.
Spread, Controversy, and the Mid-Century Debate
Through the mid-twentieth century, Rowe's elimination diets spread among allergists and, later, among the practitioners of what came to be called clinical ecology — a movement that took the food-and-environment idea in directions far broader than the mainstream would accept. This is where the elimination diet's reputation became genuinely mixed, and it is important to separate the two strands. The core method — remove suspected foods, reintroduce them under observation — is sound and is used in conventional medicine to this day. The expansive claims that some proponents attached to it — that diet and food sensitivity could explain an almost unlimited range of conditions — outran the evidence, much as Hare's "hyperpyraemia" had decades earlier.
As reviewers of the field have repeatedly noted, the elimination diet has historically suffered from a lack of universally agreed definitions, diagnostic criteria, and standardised treatment. Different clinicians eliminated different foods for different durations and judged "a reaction" differently, which made results hard to compare and the literature hard to interpret. That ambiguity — not the basic logic of the method — is the source of most of the controversy that still surrounds elimination diets, and it set the stage for two responses: a push to standardise the procedure with controlled food challenges, and the development of more tightly-defined protocols aimed at specific problems.
The Method Splits: RPAH, FODMAP, and Consumer Diets
From the late twentieth century onward, Rowe's general method branched into several distinct, named protocols — each developed by identifiable people for a particular purpose. These are the elimination diets most people encounter today.
The RPAH (food-chemical) elimination diet, Australia. Beginning in the late 1970s, researchers at the Allergy Unit of Royal Prince Alfred Hospital in Sydney developed a diagnostic elimination diet aimed not at whole foods but at naturally occurring and added food chemicals — salicylates, amines, glutamates, and certain additives — thought to trigger reactions in sensitive people. The work is associated with the hospital's allergy researchers, including Robert Loblay, Anne Swain, and Velencia Soutter, whose RPAH Elimination Diet Handbook codified the approach (it is also widely known as the "FAILSAFE" diet). Wikipedia and the diet's own literature place the foundational publication in 1978. This protocol is influential, particularly in Australia, but it remains a clinical tool used under dietitian supervision rather than a universally validated test.
The low-FODMAP diet, Monash University. The most rigorously studied modern descendant of the elimination idea is the low-FODMAP diet, developed at Monash University in Melbourne by a team led by gastroenterologist Peter Gibson with dietitian-researchers Sue Shepherd and Jane Muir. The team coined the acronym FODMAP — Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols — around 2004 and published the foundational concept in 2005, going on to measure the FODMAP content of thousands of foods. Structured as a temporary elimination followed by systematic reintroduction, it targets irritable bowel syndrome and related gut symptoms, and it has accumulated a substantial evidence base — making it the clearest example of the elimination method maturing into mainstream, evidence-supported care. It is covered in depth in the companion Low-FODMAP article.
Consumer programs (Whole30 and others). The same two-phase logic also moved into popular culture through structured 30-day consumer programs such as Whole30, which remove grains, legumes, dairy, sugar, and alcohol for a month before a guided reintroduction. These are best understood as accessible, lifestyle-oriented adaptations of the clinical method rather than validated diagnostic tests; the dedicated Whole30 article discusses what they can and cannot do.
Evidence and Reception Today
So how does mainstream medicine view the elimination diet now? The honest answer is nuanced, and it depends entirely on how the method is used.
As a supervised diagnostic method, the core approach is respected. A medically supervised oral food challenge — reintroducing a food under observation, ideally in a double-blind, placebo-controlled format — is regarded by allergists as the most definitive way to confirm whether a specific food causes a reaction. In other words, the disciplined reintroduction step that Rowe championed survives, in refined form, as the field's diagnostic gold standard. A short, structured elimination followed by careful reintroduction is a legitimate clinical tool, and for IBS the low-FODMAP version is supported by a real evidence base.
But the popular "food sensitivity" testing built around it is rejected by the major professional bodies. This is the point where truth must override marketing. The widely sold IgG (and IgG4) "food sensitivity" blood panels — often used to decide which foods to eliminate — are explicitly not recommended by the leading allergy and immunology organisations. The European Academy of Allergy and Clinical Immunology (EAACI) concluded in a 2008 task-force report that food-specific IgG4 does not indicate food allergy or intolerance and should not be used as a diagnostic tool; rather, IgG/IgG4 to a food generally reflects ordinary exposure and tolerance. The Canadian Society of Allergy and Clinical Immunology (CSACI) issued a position statement in 2012 against testing food-specific IgG, and the American Academy of Allergy, Asthma & Immunology (AAAAI) likewise states there is no reliable evidence that IgG antibodies indicate food allergy or sensitivity. The practical danger these bodies warn about is real: because such panels routinely flag common staples like wheat, dairy, and eggs, they can push people into unnecessarily broad, nutritionally risky elimination diets chasing "sensitivities" that the body does not actually have.
The honest synthesis is this. The elimination diet's method — remove, observe, reintroduce one food at a time — is sound, century-tested, and lives on in the oral food challenge and in evidence-backed protocols like low-FODMAP. What is not supported is the more sweeping promise — that elimination dieting (especially when guided by IgG testing) can diagnose and cure a wide sprawl of chronic conditions. That promise has recurred at every stage of this history, from Hare's "hyperpyraemia" to the broadest claims of clinical ecology, and the evidence has never caught up to it.
Honest Takeaways
Three things are worth carrying away from this history. First, there is no lone founder, but there is a chief architect: Albert H. Rowe (1889–1970) turned a scattered idea into a documented, named diagnostic procedure starting in 1926, and the elimination-then-reintroduction logic we use today is essentially his. He built on earlier food-and-disease thinkers such as Francis Hare, and his method was later refined and specialised by others — the RPAH researchers in Sydney and the Monash FODMAP team in Melbourne.
Second, a long history of use is not proof of broad effectiveness. The careful, supervised version of the method is genuinely useful and, in the case of oral food challenges and low-FODMAP, is endorsed or evidence-supported. The expansive claims — that elimination dieting can identify and fix a vast range of chronic ailments, especially via IgG "sensitivity" testing — are not supported, and the testing itself is advised against by EAACI, CSACI, and AAAAI.
Third, the practical detail Rowe insisted on still matters most: any elimination diet must be done carefully, kept time-limited, completed with a proper reintroduction, and planned so that removed foods are nutritionally replaced — ideally with professional guidance, and with particular caution in children, pregnancy, and anyone with a history of disordered eating. The practical "how" is covered in the main Elimination Diet page and the Benefits articles; this page has been concerned only with where the method came from and how honestly it has been judged.
Research Papers and References
The list below pairs key peer-reviewed and authoritative sources on the elimination diet's history, methodology, and current evidence with curated topic-search links. Historical primary works — Francis Hare's The Food Factor in Disease (1905) and Albert Rowe's Elimination Diets and the Patient's Allergies (1941/1944) — are named in the article as historical sources. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab.
- Stapel SO, Asero R, Ballmer-Weber BK, Knol EF, Strobel S, Vieths S, Kleine-Tebbe J; EAACI Task Force. Testing for IgG4 against foods is not recommended as a diagnostic tool: EAACI Task Force Report. Allergy. 2008;63(7):793-796. — doi:10.1111/j.1398-9995.2008.01705.x (PMID: 18489614)
- Carr S, Chan E, Lavine E, Moote W. CSACI Position statement on the testing of food-specific IgG. Allergy, Asthma & Clinical Immunology. 2012;8(1):12. — doi:10.1186/1710-1492-8-12 (PMID: 22835332)
- Sampson HA, Gerth van Wijk R, Bindslev-Jensen C, et al. Standardizing double-blind, placebo-controlled oral food challenges: American Academy of Allergy, Asthma & Immunology–European Academy of Allergy and Clinical Immunology PRACTALL consensus report. Journal of Allergy and Clinical Immunology. 2012;130(6):1260-1274. — doi:10.1016/j.jaci.2012.10.017 (PMID: 23195525)
- Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. Journal of Gastroenterology and Hepatology. 2010;25(2):252-258. — doi:10.1111/j.1440-1746.2009.06149.x (PMID: 20136989)
- Review of Hare F. The Food Factor in Disease. Bristol Medico-Chirurgical Journal. 1906;24(92):160-162. (Contemporary review of Hare's 1905 work.) — PMC5046463
- Hare F. The Food Factor in Disease (1905), Vol. 1. (Historical primary source.) — Internet Archive: foodfactorindise01hare
- Albert H. Rowe (1889–1970) Papers — biographical and archival finding aid. University of California, Davis / Online Archive of California. — OAC finding aid (ark:/13030/c8zp47vq)
- Elimination diet history and food allergy diagnosis — PubMed: elimination diet, food allergy diagnosis, and oral food challenge
- IgG food sensitivity testing — clinical validity — PubMed: IgG food-sensitivity testing and its clinical validity
External Authoritative Resources
- AAAAI — IgG food sensitivity testing (patient guidance)
- NCCIH — Irritable Bowel Syndrome and dietary approaches
- Monash University — FODMAP / low-FODMAP diet program
Connections
- All Remedies
- Elimination Diet
- Elimination Diet Benefits
- Low-FODMAP
- Whole30
- Gut Healing
- Irritable Bowel Syndrome
- Food Intolerance
- Allergies