Exercise and Meal Timing for Blood Sugar
Two interventions produce the largest postprandial glucose effects of any non-pharmacologic approach after carbohydrate restriction itself: post-meal walking and meal sequencing. A 10-minute brisk walk starting 15-30 minutes after a carbohydrate-containing meal reduces peak glucose by 12-22% (Reynolds 2016, DiPietro 2013). Eating vegetables and protein before starch reduces peak glucose by 30-40% without changing what is eaten, only the order (Shukla 2015, Imai 2014). Resistance training increases insulin-independent muscle glucose uptake for 24-48 hours via GLUT4 translocation that does not require insulin signaling. Early time-restricted feeding (eating window aligned to the morning circadian rhythm) improves insulin sensitivity even without weight loss (Sutton 2018). This deep-dive covers the mechanism behind each effect, the evidence base, the practical timing parameters, the relevance for both diabetic and non-diabetic populations, and the interactions between exercise type, meal composition, and circadian timing.
Table of Contents
- Post-Meal Walking — The Largest Single Effect
- Meal Sequencing — Free 30-40% Reduction
- Resistance Training and GLUT4
- Aerobic vs Resistance Training Compared
- Early Time-Restricted Feeding
- The Dawn Phenomenon
- Vinegar, Fiber, and Acidity Tricks
- Stacking Interventions for Maximum Effect
- A Practical Daily Schedule
- Key Research Papers
- Connections
- Featured Videos
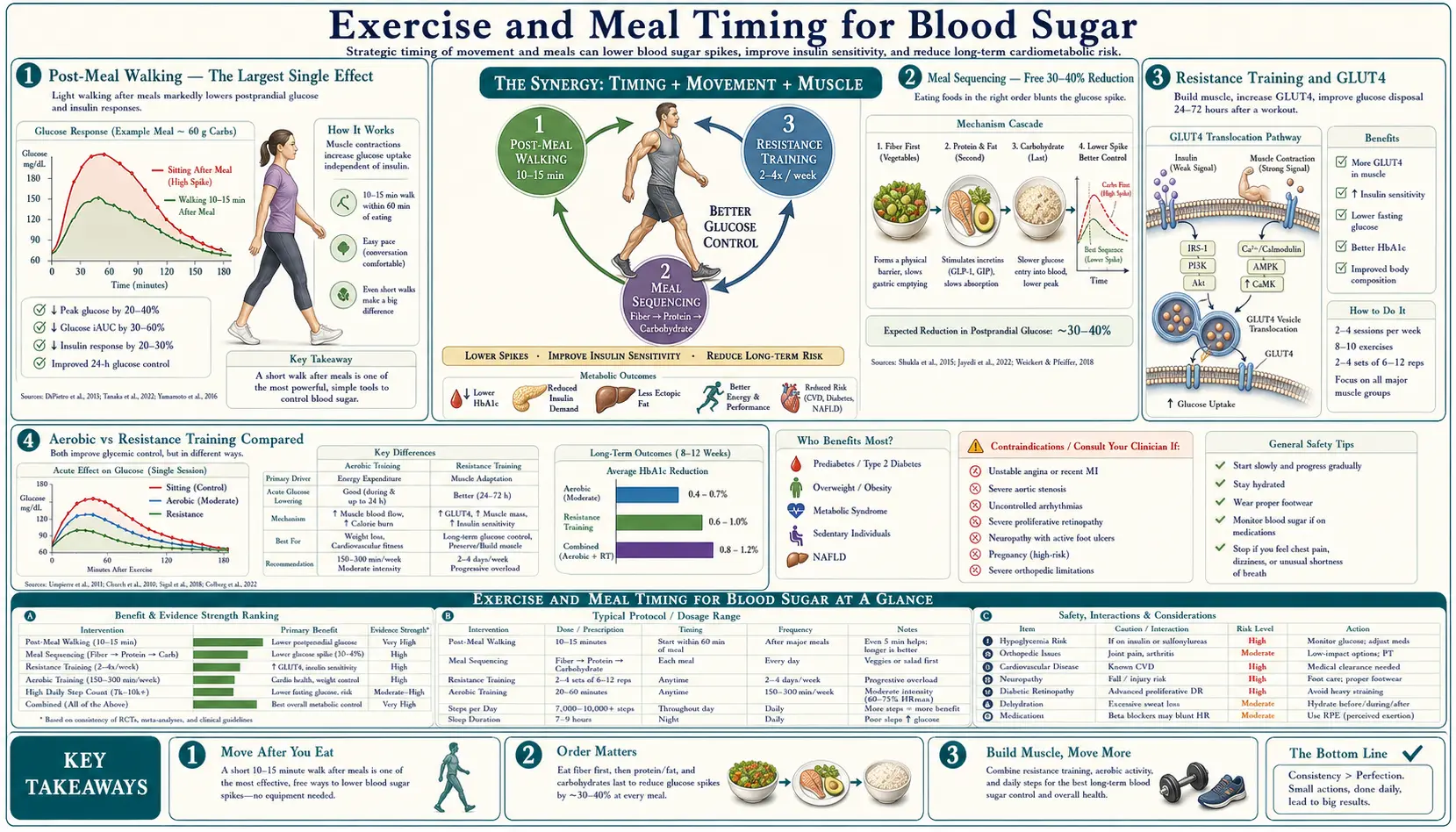
Post-Meal Walking — The Largest Single Effect
If a single non-pharmacologic intervention could be patented and marketed as a diabetes medication, post-meal walking would be one of the strongest candidates. The effect size in clinical trials is comparable to or larger than many oral hypoglycemic agents, costs nothing, and carries no side effects.
The Reynolds 2016 Diabetologia trial is the clearest demonstration. 41 adults with Type 2 diabetes were randomized in a crossover design to either:
- Walk 30 minutes per day, unspecified timing
- Walk 10 minutes after each meal (3× per day, total 30 minutes), starting within 5 minutes of finishing eating
Both groups walked the same total time. The post-meal walking group had 12% lower postprandial glucose iAUC, with the largest effect after the evening meal (22% lower). The DiPietro 2013 Diabetes Care trial showed similar results with three 15-minute post-meal walks in older adults at risk for impaired glucose tolerance.
The mechanism operates at two levels:
- Insulin-independent muscle glucose uptake — muscle contraction itself triggers GLUT4 translocation to the muscle cell membrane via an AMPK-mediated pathway parallel to but independent of the insulin signaling cascade. During and shortly after exercise, working muscle can take up glucose at rates 5-10× baseline without requiring proportional insulin. This is the same mechanism that explains why exercise lowers blood glucose in Type 1 diabetics whose insulin levels are constant.
- Increased post-exercise GLUT4 expression — the muscle's capacity to take up glucose remains elevated for 24-48 hours after a single bout of moderate exercise, providing a sustained insulin-sensitizing effect beyond the immediate post-meal window.
Practical parameters:
- Timing — start within 15-30 minutes after finishing the meal, before peak glucose excursion. Walking that starts 60 minutes after eating misses much of the postprandial spike.
- Intensity — brisk walking pace (4-5 km/h, 100-120 steps/min), enough to slightly elevate breathing but still able to hold conversation. Light strolling is not sufficient.
- Duration — 10-15 minutes is enough to capture most of the benefit. Longer walks add benefit but with diminishing returns.
- Frequency — after each major meal is ideal. After the largest meal (typically dinner in Western diets) is the highest-priority single walk.
The Buffey 2022 meta-analysis extended the principle beyond walking specifically: even interrupting prolonged sitting with light-intensity activity (standing, casual walking) every 30 minutes improves postprandial glucose, fasting insulin, and triglycerides. The relevant variable is muscle activation, not exercise intensity per se.
Meal Sequencing — Free 30-40% Reduction
The Shukla 2015 Diabetes Care trial is the cleanest demonstration of meal sequencing. 11 patients with Type 2 diabetes ate identical meals (ciabatta bread, orange juice, chicken breast, lettuce/tomato salad with low-fat dressing, broccoli with butter) on three different days in three different orders:
- Carbohydrate first (bread, juice), 15 minutes later protein and vegetables
- Protein and vegetables first, 15 minutes later carbohydrate
- All together (control)
Results: the protein-and-vegetables-first order produced postprandial glucose 29% lower at 30 minutes, 37% lower at 60 minutes, and 17% lower at 120 minutes compared to the carbohydrate-first order. Insulin levels were also lower with the vegetable-first order. The all-together (control) condition fell in between.
The Imai 2014 Japanese trial replicated the finding in 333 Type 2 diabetes patients eating vegetables before carbohydrate as a daily practice for 24 months — with HbA1c reduction of 1.1% on average and improved fasting glucose, comparable to the effect of adding an oral hypoglycemic agent.
The mechanism operates through multiple parallel pathways:
- Slowed gastric emptying — fiber and fat in the vegetables and protein delay the rate at which the subsequent carbohydrate reaches the small intestine for absorption. Glucose that arrives at the absorptive surface over a longer period produces a smaller peak.
- Glucagon-like peptide 1 (GLP-1) preload — protein consumed first stimulates GLP-1 secretion from intestinal L cells before the carbohydrate arrives. GLP-1 enhances insulin secretion, suppresses glucagon, and further slows gastric emptying — the same mechanism exploited by semaglutide, liraglutide, and other GLP-1 receptor agonists.
- Increased viscosity in the gut lumen — soluble fiber from vegetables increases the viscosity of intestinal contents, slowing the diffusion of glucose to the brush border for absorption.
Practical implementation: the rule is simply "vegetables and protein first, starch and starchy fruit last". A reasonable target is to eat vegetables and protein for 5-10 minutes before any bread, rice, pasta, potato, or sweet fruit appears. The order matters more than the exact gap. The intervention is free, requires no behavior change other than chewing order, and produces effects comparable to medications costing hundreds of dollars per month.
Resistance Training and GLUT4
Skeletal muscle is the largest insulin-sensitive tissue by mass and the dominant site of postprandial glucose disposal in healthy adults. The total muscle mass directly determines the body's capacity to clear post-meal glucose. Resistance training increases this capacity through two parallel mechanisms.
Muscle mass increase — each kilogram of additional skeletal muscle can dispose of approximately 13 mg of glucose per minute during postprandial conditions. Adding 5 kg of muscle through 12-24 months of consistent resistance training produces meaningful improvement in 2-hour OGTT values and HbA1c independent of any weight loss.
GLUT4 expression and translocation — each bout of resistance exercise upregulates the GLUT4 glucose transporter in trained muscle. Muscle that has been exercised in the past 24-48 hours can take up glucose at higher rates per unit mass than untrained muscle. This is partially insulin-independent (AMPK-mediated) and partially insulin-sensitizing (increased response to a given insulin signal).
The Sigal 2007 Annals of Internal Medicine trial compared aerobic training, resistance training, and combined training in 251 Type 2 diabetes patients over 22 weeks. HbA1c reductions:
- Aerobic training alone: −0.51%
- Resistance training alone: −0.38%
- Combined aerobic + resistance: −0.97%
- Control (no exercise): +0.05%
The combined approach produced HbA1c reductions roughly equal to the sum of the individual effects, suggesting the two modalities operate through partially independent mechanisms (aerobic improves cardiovascular fitness and overall insulin sensitivity; resistance increases muscle mass and GLUT4 expression).
Practical parameters for resistance training oriented to blood-sugar benefit:
- Frequency — 2-3 sessions per week, alternating muscle groups or full-body splits.
- Volume — 8-12 working sets per major muscle group per week, sufficient to drive hypertrophy in the muscles that matter most for glucose disposal (quadriceps, hamstrings, glutes, latissimus dorsi).
- Intensity — sets of 6-15 repetitions to within 1-3 reps of failure. The total work matters more than absolute intensity for glucose disposal benefit.
- Compound movements — squats, deadlifts, presses, rows, and chin-ups recruit the largest muscle mass per movement and produce the largest glucose-disposal benefit per unit time.
Aerobic vs Resistance Training Compared
Both modalities have distinct mechanisms and complementary benefits:
- Aerobic exercise (walking, cycling, swimming, running) — produces immediate post-exercise glucose lowering via insulin-independent muscle uptake during the activity, with continued insulin-sensitizing effects for 12-48 hours afterward. Improves cardiovascular fitness, reduces visceral fat, and improves endothelial function. The dominant evidence base for diabetes prevention (Diabetes Prevention Program intervention was aerobic).
- Resistance exercise (weight training, calisthenics, resistance bands) — increases muscle mass and GLUT4 expression, producing longer-duration (24-72 hour) insulin sensitizing effects. Particularly important for older adults to counter sarcopenia. Improves bone density and functional capacity.
- High-intensity interval training (HIIT) — combines elements of both. Short bouts of intense effort (typically 30 seconds to 4 minutes) alternated with recovery periods. Produces large improvements in mitochondrial function and insulin sensitivity per unit time, but less hypertrophy than dedicated resistance training.
The optimal approach combines all three over the course of a week:
- 150 minutes per week of moderate aerobic activity (the ADA/USPSTF target)
- 2-3 resistance training sessions per week (covering all major muscle groups)
- 1-2 short HIIT sessions per week (optional but high time-efficiency)
For adults whose only time available is 30 minutes per day, alternating days of brisk walking with days of resistance training produces excellent metabolic health with manageable time commitment.
Early Time-Restricted Feeding
Time-restricted eating (TRE) refers to consuming all daily calories within a compressed daily window (typically 8-12 hours) without specifically restricting caloric intake. Early time-restricted feeding (eTRF) further specifies that the eating window should be in the early/mid day, with last meal completed by mid-afternoon. The motivation is alignment with the circadian rhythm of insulin sensitivity, which is highest in the morning and declines through the day.
The Sutton 2018 Cell Metabolism trial is the cleanest mechanistic demonstration. 8 men with prediabetes were randomized in a crossover design to:
- 5 weeks of eTRF: all calories consumed between 7 AM and 3 PM (8-hour window in early day)
- 5 weeks of standard control: all calories consumed between 7 AM and 9 PM (12-hour window)
Both groups consumed identical calories. The eTRF group showed:
- Improved insulin sensitivity (HOMA-IR decreased)
- Lower blood pressure (~10/11 mmHg systolic/diastolic reduction)
- Reduced oxidative stress markers
- Improved appetite regulation
These improvements occurred without weight loss, demonstrating that the circadian alignment itself produced the metabolic benefit. The Jamshed 2019 Nutrients replication study confirmed similar findings with improved 24-hour glucose profiles, circadian clock gene expression, and autophagy markers.
The relevance for blood-sugar management: insulin sensitivity is approximately 30-50% higher in the morning than in the evening for most adults. A given carbohydrate load produces a larger postprandial spike at 8 PM than at 8 AM. Compressing the eating window to the morning hours leverages this circadian peak.
Practical implementation:
- Conservative eTRF — eating window 8 AM to 6 PM (10 hours). Less disruptive of social meals but captures most of the benefit.
- Standard eTRF — eating window 7 AM to 3 PM (8 hours). The Sutton protocol; produces the largest documented effects but requires substantial behavior change.
- Skip-dinner approach — large breakfast and lunch, minimal or no dinner. Aligns with traditional Mediterranean and Middle Eastern eating patterns historically.
See our Intermittent Fasting page for broader context on time-restricted and fasting approaches.
The Dawn Phenomenon
The dawn phenomenon is the physiologic morning rise in blood glucose driven by the circadian release of growth hormone, cortisol, and catecholamines in the pre-waking hours (typically 4 AM to 8 AM). This release prepares the body for activity by increasing hepatic gluconeogenesis and decreasing insulin sensitivity. In a healthy person, the pancreas compensates by increasing insulin secretion, keeping glucose stable. In a person with insulin resistance or beta-cell dysfunction, the compensation is incomplete and fasting morning glucose rises.
This explains a common observation: fasting glucose can be 110-130 mg/dL in the morning despite no food consumption since dinner the night before. The glucose did not come from anywhere external; the liver produced it under hormonal stimulation during the pre-dawn hours.
Practical implications:
- Fasting morning glucose is influenced by the dawn phenomenon, not just by what was eaten the previous day. A high morning value does not necessarily mean the previous evening's meal was bad.
- Breakfast may produce a larger-than-expected glucose response in some people because it stacks on top of the dawn-phenomenon elevation already present.
- Late-evening exercise can blunt the dawn phenomenon the following morning by depleting hepatic glycogen, reducing the liver's substrate for early-morning gluconeogenesis.
- For some people with prominent dawn phenomenon, skipping breakfast and eating later in the morning gives time for the cortisol surge to subside before adding dietary glucose load — producing a flatter overall morning curve than a conventional 7 AM breakfast.
Vinegar, Fiber, and Acidity Tricks
Several low-cost dietary additions consistently blunt postprandial glucose:
- Vinegar — the Johnston 2010 trial showed that 2 tablespoons (30 mL) of apple cider vinegar consumed 5 minutes before a high-carbohydrate meal reduced postprandial glucose iAUC by approximately 20%. The mechanism involves α-amylase inhibition (slowing starch breakdown) plus slowed gastric emptying. Any vinegar (apple cider, red wine, balsamic, white) appears to work; the acetic acid is the active ingredient. Practical delivery: vinegar in salad dressing eaten before the starch portion of the meal.
- Lemon juice — same mechanism as vinegar via citric acid. 30 mL of lemon juice before a meal produces effects comparable to vinegar in some trials.
- Soluble fiber — psyllium husk (5-10 g before a meal), chia seeds, glucomannan, and oat beta-glucan all increase gut luminal viscosity and reduce glucose absorption rate. Effect size of approximately 15-25% reduction in postprandial glucose. See our Food section for fiber-rich options.
- Cinnamon — 1-3 g per day of Ceylon cinnamon (true cinnamon, not the cheaper cassia which contains hepatotoxic coumarin in high doses) modestly reduces postprandial glucose. Effect size is smaller than vinegar or fiber but additive. See our Cinnamon page.
- Berberine — 500 mg before each major meal lowers postprandial glucose via AMPK activation (the same mechanism as metformin). Larger effect than the dietary additions above, with HbA1c reductions of 0.7-1.0% in clinical trials. See our Berberine page.
- Whey protein preload — 20-30 g whey protein consumed 15-30 minutes before a high-carbohydrate meal stimulates GLP-1 and insulin release that blunts the subsequent glucose excursion. Effect size of 20-30% reduction.
Stacking Interventions for Maximum Effect
The individual interventions above can be stacked for additive benefit. A meal eaten with all of the following techniques simultaneously typically produces 50-70% reduction in postprandial glucose iAUC compared to the same meal eaten without any intervention:
- 2 tbsp vinegar in salad dressing 5 minutes before eating
- Salad and protein first; carbohydrate 5-10 minutes later
- 10-minute walk starting 15 minutes after finishing the meal
- Cinnamon sprinkled on the carbohydrate portion (e.g., on oatmeal, fruit)
For someone with established insulin resistance or Type 2 diabetes, stacking all four of these is the practical equivalent of adding a second-line oral hypoglycemic agent — without cost or side effects.
A Practical Daily Schedule
An evidence-based daily schedule for optimal blood-sugar management in a typical working adult:
- 6:30 AM — wake; 16-ounce glass of water; no food yet. Cortisol and growth hormone are peaking; insulin sensitivity is good but the dawn phenomenon is still resolving.
- 7:00 AM — 20-minute resistance training session OR brisk walk. Glycogen depletion at this time enhances glucose disposal capacity for the rest of the day.
- 8:00 AM — breakfast. Protein and fat dominant (eggs, Greek yogurt, nuts). Modest carbohydrate, eaten last. No added sugar.
- 8:30 AM — 10-minute walk (commute, dog walk, errand). Captures the post-meal glucose excursion.
- 12:30 PM — lunch. Salad with vinegar dressing first. Protein second. Starch (if any) last. Vegetables and protein should occupy 75% of the plate by volume.
- 1:00 PM — 10-minute post-meal walk.
- 3:00 PM — optional small protein-and-fat snack if hungry (handful of nuts, hard-boiled egg). Avoid carbohydrate snacks; they break the morning insulin-sensitive window.
- 6:00 PM — dinner. Same sequencing rules. This is the meal where post-meal walking has the largest benefit (Reynolds 2016).
- 6:30 PM — 15-minute brisk walk after dinner. Largest single intervention of the day.
- 8:00 PM — eating window closes. No food for the next 12+ hours. Allows liver glycogen to deplete overnight, supports autophagy and insulin sensitivity.
- 10:30 PM — lights out. Sleep deprivation acutely worsens insulin resistance; sleep duration < 6 hours predicts increased Type 2 diabetes risk.
This schedule operates a roughly 12-hour eating window (8 AM to 8 PM), with post-meal walks at each major meal, vegetable-first sequencing throughout, and morning exercise to depleting hepatic glycogen. None of the individual components require special equipment or cost. The cumulative effect on HbA1c is typically 0.8-1.5% reduction in patients with established insulin resistance — comparable to adding metformin — while also improving cardiovascular fitness, body composition, sleep quality, and mood.
Key Research Papers
- Reynolds AN et al. (2016). Advice to walk after meals is more effective for lowering postprandial glycaemia in type 2 diabetes mellitus than advice that does not specify timing: a randomised crossover study. Diabetologia. — PubMed
- DiPietro L et al. (2013). Three 15-min bouts of moderate postmeal walking significantly improves 24-h glycemic control in older people at risk for impaired glucose tolerance. Diabetes Care. — PubMed
- Buffey AJ et al. (2022). The acute effects of interrupting prolonged sitting time in adults with standing and light-intensity walking on biomarkers of cardiometabolic health. Sports Med. — PubMed
- Shukla AP et al. (2015). Food order has a significant impact on postprandial glucose and insulin levels. Diabetes Care. — PubMed
- Imai S et al. (2014). Eating vegetables before carbohydrates improves postprandial glucose excursions in Japanese patients with type 2 diabetes. Asia Pac J Clin Nutr. — PubMed
- Sutton EF et al. (2018). Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metabolism. — PubMed
- Jamshed H et al. (2019). Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy. Nutrients. — PubMed
- Sigal RJ et al. (2007). Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: a randomized trial. Ann Intern Med. — PubMed
- Holloszy JO (2005). Exercise-induced increase in muscle insulin sensitivity. J Appl Physiol. — PubMed
- Johnston CS et al. (2010). Vinegar and peanut products as complementary foods to reduce postprandial glycemia. J Am Diet Assoc. — PubMed
- Frank LL et al. (2005). Effects of exercise on metabolic risk variables in overweight postmenopausal women: a randomized clinical trial. Obes Res. — PubMed
- Hawley JA, Lessard SJ (2008). Exercise training-induced improvements in insulin action. Acta Physiol. — PubMed
PubMed Topic Searches
- PubMed: Post-meal walking and glucose
- PubMed: Meal sequencing
- PubMed: TRE/IF and glucose
- PubMed: Resistance training and insulin
- PubMed: Vinegar and postprandial glycemia
Connections
- Blood Sugar Benefits Hub
- Blood Sugar (Main)
- Glycemic Index & Load
- Insulin Resistance
- Continuous Glucose Monitoring
- Intermittent Fasting
- Ketogenic Diet
- Cinnamon
- Berberine
- Chromium
- Magnesium
- Endocrinology
- Food
- Lab Tests
- All Remedies