Aspirin Bleeding Risks and Cautions
Bleeding is the defining limit on aspirin's clinical utility. The same irreversible COX-1 inhibition in platelets that prevents arterial thrombi also reduces gastric prostaglandin protection and tilts hemostasis toward bleeding for the 7-10 days it takes new platelets to repopulate the circulation. The absolute bleeding rates are modest in individuals: roughly 0.3% per year for clinically significant gastrointestinal hemorrhage on low-dose aspirin, and about 0.05% per year for hemorrhagic stroke. But these small per-person rates accumulate over decades and grow steeply with age — doubling roughly every decade after 60. This is why the same risk-benefit calculation that favors aspirin in younger high-cardiovascular-risk patients shifts unfavorably in healthy older adults, and why every aspirin prescription must include a brief screen for bleeding-risk factors. This page covers risk quantification, risk stratification, the H. pylori interaction, PPI co-therapy, the dangerous NSAID-aspirin combination, perioperative management, and the absolute contraindications.
Table of Contents
- Mechanism: How Aspirin Causes Bleeding
- Gastrointestinal Bleeding: Quantitative Risk
- Intracranial Hemorrhage: A Rare but Serious Event
- Risk Stratification by Age and History
- The Helicobacter pylori Interaction
- Proton Pump Inhibitor Co-Therapy
- The NSAID + Aspirin Combination (Dangerous)
- Ibuprofen Blocks Aspirin's Antiplatelet Effect
- Perioperative Aspirin Management
- Absolute Contraindications
- Reye's Syndrome in Children and Teens
- Key Research Papers
- Connections
- Featured Videos
Mechanism: How Aspirin Causes Bleeding
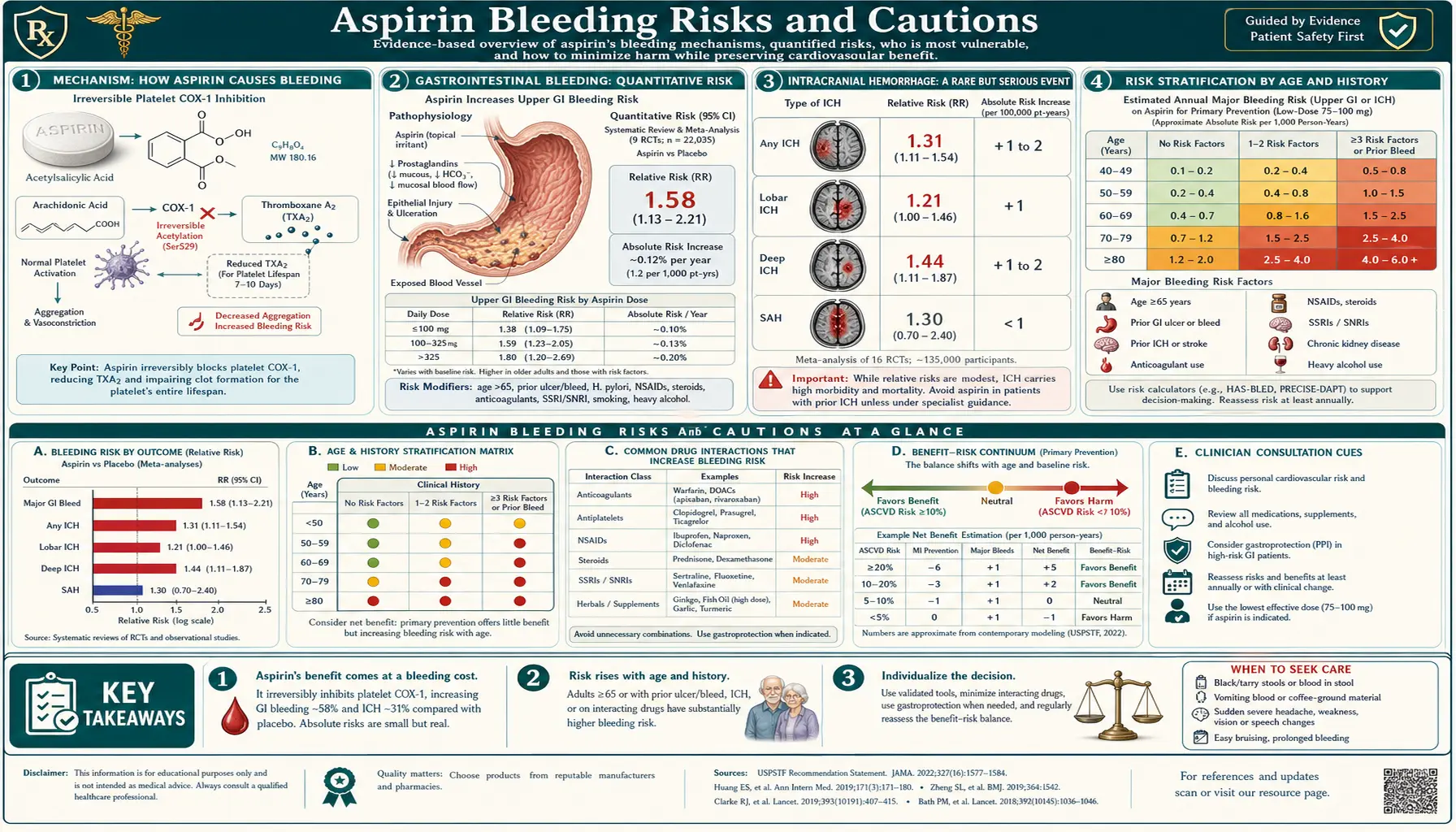
Aspirin causes bleeding through two interacting mechanisms. First, the antiplatelet effect: irreversible acetylation of platelet COX-1 abolishes thromboxane A2 production for the platelet's entire lifespan. Because platelets are anucleate and cannot synthesize new COX-1, full recovery of platelet function requires 7-10 days as new platelets replace the inhibited ones. During this period, primary hemostasis (the platelet plug that stops small-vessel bleeding) is impaired.
Second, the direct mucosal effect: aspirin reduces gastric prostaglandins (PGE2 and PGI2 produced by COX-1 in gastric mucosal cells) that maintain the protective mucus and bicarbonate layer covering the stomach lining. The result is reduced mucosal defense against gastric acid, predisposing to erosions, ulcers, and bleeding from gastric and duodenal mucosa. This mucosal effect is dose-dependent and partly mediated locally; enteric-coated aspirin reduces it modestly but does not eliminate it (Maree 2005, PMID 16139140).
The bleeding consequences of aspirin therefore differ by site. Gastrointestinal bleeding reflects both effects (impaired platelet plug + mucosal injury) and is the most common clinically significant bleeding type. Intracranial hemorrhage reflects mainly the platelet effect on cerebral microvasculature. Bleeding from surgical sites, skin trauma, or invasive procedures reflects primarily impaired primary hemostasis.
Gastrointestinal Bleeding: Quantitative Risk
The McQuaid and Laine 2006 systematic review (PMID 16490465) pooled 14 randomized trials of low-dose aspirin (75-325 mg) for cardiovascular prevention and quantified GI bleeding risk: aspirin approximately doubles the rate of clinically significant GI bleeding, from a baseline of about 0.15% per year on placebo to 0.3% per year on aspirin. Absolute rates rise with age, prior GI history, concomitant medications, and dose.
The Lanas 2011 AJG paper (PMID 21931380) provided population-based estimates from Spanish primary care: hospitalization for upper GI bleeding occurred at 4.8 cases per 1000 patient-years on low-dose aspirin, versus 1.5 cases per 1000 on no antiplatelet therapy — an absolute increase of about 3.3 cases per 1000 person-years, or roughly 1 hospitalization per 300 patient-years.
The Garcia Rodriguez 2011 BMJ paper (PMID 21300722) found similar rates and identified concomitant NSAIDs (other than aspirin), anticoagulants, prior peptic ulcer disease, and age >75 as the dominant modifiable risk factors.
Importantly, GI bleeding from low-dose aspirin is generally treatable. Mortality from upper GI bleeding is approximately 5-10%, and most cases resolve with endoscopic intervention. Hemorrhagic stroke from aspirin, by contrast, has much higher mortality and disability burden.
The ASPREE bleeding analysis (PMID 30221595) quantified bleeding in healthy older adults: major hemorrhage occurred in 3.8% of the aspirin group vs 2.8% of the placebo group over 4.7 years — an absolute increase of 1% over the trial duration, or about 8.6 events per 1000 person-years on aspirin vs 6.2 on placebo. Most of the excess was upper GI bleeding.
Intracranial Hemorrhage: A Rare but Serious Event
Intracranial hemorrhage on aspirin is rare but life-altering. Meta-analyses (Hochholzer 2011, PMID 21217142) estimate the absolute risk increase at about 0.03% per year for low-dose aspirin in primary prevention. Stratified by age, the rate roughly doubles per decade after 65, reaching 0.1-0.2% per year in adults over 75.
The case-fatality of intracranial hemorrhage approaches 40-50% in the first month, with substantial disability among survivors. The aspirin-attributable hemorrhagic stroke risk is one of the major reasons the USPSTF restricted primary-prevention aspirin to adults under 60 in its 2022 guidance — the rising hemorrhagic stroke risk with age tips the benefit-harm balance unfavorably.
Patients on aspirin who develop new severe headache, sudden neurological deficit, or altered consciousness should be evaluated for intracranial bleeding without delay. Cerebral amyloid angiopathy, a common condition in older adults that predisposes to lobar intracranial hemorrhage, is a particular concern; some authorities recommend imaging assessment (gradient echo MRI to identify microbleeds) before initiating aspirin in older patients with cognitive impairment.
Risk Stratification by Age and History
Modifiable and non-modifiable bleeding-risk factors on aspirin:
- Age >75 — the single largest risk factor. GI bleeding rate roughly doubles between ages 50 and 70, and again between 70 and 85.
- Prior peptic ulcer or upper GI bleeding — particularly within the past 5 years. Doubles to triples baseline risk.
- Concomitant non-aspirin NSAID — substantially elevates risk (see NSAID section below). Avoid co-administration when possible.
- Concomitant anticoagulant (warfarin, DOACs, heparin) — aspirin plus anticoagulant approximately doubles bleeding rates compared with anticoagulant alone. Combination should be avoided unless there is a strong indication (e.g., recent stent).
- Concomitant SSRI — SSRIs impair platelet serotonin uptake, modestly increasing bleeding risk in aspirin users.
- Active H. pylori infection — test-and-treat reduces ulcer/bleeding risk.
- Severe thrombocytopenia (platelet count <50,000) — relative contraindication.
- Significant chronic liver disease, alcohol use disorder, advanced chronic kidney disease — all elevate bleeding risk.
A 2022 retrospective derivation of the HAS-BLED score (originally designed for atrial fibrillation anticoagulation) has been adapted for aspirin bleeding-risk assessment, though no single score is widely standardized for the primary-prevention aspirin decision.
The Helicobacter pylori Interaction
Helicobacter pylori infection of the gastric mucosa is a major risk multiplier for aspirin-associated upper GI bleeding. H. pylori produces chronic gastritis and increases the baseline risk of peptic ulcer. The combination of H. pylori infection plus aspirin substantially raises ulcer-bleeding risk compared with either alone.
The Hawkey 2008 trial (PMID 18549457) and earlier work by Chan and colleagues showed that in patients with prior ulcer history starting low-dose aspirin, H. pylori eradication therapy reduced subsequent ulcer recurrence to a rate similar to that achieved by PPI co-therapy.
Clinical implication: in patients with prior peptic ulcer disease or upper GI bleeding who require aspirin, test for H. pylori (urea breath test or stool antigen) and treat if positive. Co-administer a PPI in high-risk patients. The 2022 American College of Gastroenterology guideline on aspirin/NSAID GI complications endorses this approach.
Proton Pump Inhibitor Co-Therapy
Proton pump inhibitors (omeprazole, pantoprazole, esomeprazole, etc.) reduce gastric acid secretion and substantially lower the risk of aspirin-associated upper GI bleeding. The COGENT trial (PMID 20925534) randomized 3,761 patients on aspirin plus clopidogrel to omeprazole or placebo and showed a 66% relative reduction in upper GI bleeding with PPI co-therapy, with no detectable adverse cardiovascular interaction (despite earlier concern that omeprazole might attenuate clopidogrel's antiplatelet effect through CYP2C19 inhibition).
Routine PPI co-therapy is not indicated for all aspirin users — only for those with elevated bleeding risk (prior ulcer, anticoagulant co-therapy, age >70 plus another risk factor, or dual antiplatelet therapy). The American College of Gastroenterology recommends PPI co-therapy in these subgroups. For low-risk aspirin users, routine PPI use exposes the patient to the small but real long-term PPI risks (vitamin B12 deficiency, magnesium deficiency, increased risk of Clostridioides difficile infection, possible bone density effects) without clear net benefit.
The NSAID + Aspirin Combination (Dangerous)
Concomitant non-aspirin NSAID use (ibuprofen, naproxen, diclofenac, celecoxib, etc.) is one of the most underrecognized aspirin-bleeding-risk multipliers. Adding an NSAID to aspirin roughly triples the risk of upper GI bleeding compared with aspirin alone. The mechanism is additive mucosal injury and additive platelet dysfunction (for non-selective NSAIDs).
Practical recommendation: patients on daily low-dose aspirin should be cautioned to avoid ibuprofen, naproxen, and other NSAIDs for pain or fever — acetaminophen is the safer first-line alternative. When NSAID use is unavoidable (e.g., gout flare, severe musculoskeletal pain), the lowest effective dose for the shortest necessary duration should be used, with PPI co-therapy.
This recommendation is especially important for older adults, who may take aspirin daily for cardiovascular prevention and OTC ibuprofen or naproxen for arthritis pain without recognizing the additive bleeding risk.
Ibuprofen Blocks Aspirin's Antiplatelet Effect
A separate but related concern: ibuprofen taken within 8 hours before low-dose aspirin can occupy the COX-1 active site and prevent aspirin's irreversible acetylation. The Catella-Lawson 2001 NEJM paper (PMID 11752352) demonstrated this pharmacodynamic interference: aspirin's antiplatelet effect was substantially blunted when ibuprofen was taken first.
The FDA issued a 2006 advisory addressing this: patients taking daily low-dose aspirin should take ibuprofen at least 30 minutes after aspirin or at least 8 hours before. Naproxen and celecoxib do not appear to produce the same interference to the same degree, though data are more limited.
This interaction matters most for patients relying on aspirin for cardiovascular protection — the protective effect can be eliminated by a single morning dose of ibuprofen taken before the morning aspirin.
Perioperative Aspirin Management
Perioperative aspirin management is one of the most contested areas of antiplatelet management. The traditional approach was to discontinue aspirin 7-10 days before elective surgery to allow platelet recovery. More recent evidence, including the POISE-2 trial (Devereaux 2014 NEJM), has shown that continuing aspirin perioperatively in patients without recent cardiac stents produces no clear reduction in cardiovascular events but does increase major bleeding.
Current general approach:
- Low-bleeding-risk surgery (cataract, dental procedures, dermatologic) — continue aspirin.
- Most non-cardiac, non-neurosurgical surgery in patients without recent stents — can typically be performed without holding aspirin, or with brief 5-7 day hold if surgeon prefers.
- Cardiac surgery (CABG) — aspirin typically continued through surgery.
- Recent coronary stent (especially DES <6-12 months) — aspirin should NOT be held; bridging strategy required if anticoagulation is also held.
- Neurosurgery, ophthalmologic posterior chamber surgery, prostate surgery, certain spine surgeries — aspirin typically held 5-7 days pre-op due to high bleeding consequence.
Decisions should be individualized and made jointly between cardiology, the surgical service, and anesthesia.
Absolute Contraindications
- Known aspirin or salicylate hypersensitivity (including aspirin-exacerbated respiratory disease — the Samter's triad of asthma, nasal polyps, and aspirin sensitivity).
- Active gastrointestinal or genitourinary bleeding.
- Severe thrombocytopenia (platelet count typically <50,000/µL for routine therapy; <20,000 for any therapy).
- Recent intracranial hemorrhage.
- Hemorrhagic diathesis (hemophilia, severe von Willebrand disease).
- Children and adolescents with febrile viral illness (Reye's syndrome risk).
- Third-trimester pregnancy at full anti-inflammatory dose (increased risk of premature ductus arteriosus closure, peripartum hemorrhage). Low-dose 81 mg aspirin is widely used in pregnancy for preeclampsia prevention; the third-trimester contraindication applies to higher anti-inflammatory doses.
Reye's Syndrome in Children and Teens
Reye's syndrome is a rare but devastating illness consisting of acute encephalopathy and hepatic dysfunction, occurring almost exclusively in children and teenagers recovering from viral infections (especially influenza and varicella) who received aspirin. The Belay 1999 NEJM paper (PMID 10228191) describes the U.S. epidemiology: incidence fell from over 500 cases per year in 1980 to fewer than 2 per year by the mid-1990s, paralleling the public-health campaign to avoid aspirin in children with viral illness.
Mortality of Reye's syndrome historically approached 30-40%. Because the pathophysiology is incompletely understood, the recommendation is absolute avoidance: aspirin should not be given to children or adolescents under 19 with febrile viral illness. Acetaminophen and ibuprofen are the appropriate alternatives. The only pediatric indication for aspirin is Kawasaki disease (acute febrile vasculitis), where the benefit-risk calculation favors short-term high-dose aspirin under specialist supervision.
Key Research Papers
- McQuaid KR & Laine L, Am J Med 2006 — systematic review of low-dose aspirin GI bleeding Search PubMed
- Lanas A et al., AJG 2011 — GI bleeding population study Search PubMed
- Mahady SE et al., ASPREE bleeding analysis NEJM 2018 — Search PubMed
- Garcia Rodriguez LA et al., BMJ 2011 — upper GI bleeding population study Search PubMed
- Hochholzer W et al., Eur Heart J 2011 — intracranial hemorrhage with antiplatelet therapy Search PubMed
- Hawkey CJ et al., Aliment Pharmacol Ther 2008 — H. pylori eradication and aspirin GI risk Search PubMed
- Bhatt DL et al., COGENT trial NEJM 2010 — PPI co-therapy Search PubMed
- Catella-Lawson F et al., NEJM 2001 — ibuprofen blocks aspirin antiplatelet effect Search PubMed
- Sostres C & Lanas A, Best Pract Res Clin Gastroenterol 2012 — GI effects of aspirin Search PubMed
- Belay ED et al., NEJM 1999 — Reye's syndrome epidemiology Search PubMed
- Maree AO et al., JACC 2005 — enteric-coated aspirin pharmacology Search PubMed
- Bibbins-Domingo K, USPSTF 2016 benefit-harm modeling Search PubMed
- USPSTF 2022 aspirin recommendation (with bleeding analysis) — PubMed PMID 35471505
- ARRIVE trial bleeding outcomes (Lancet 2018) — Search PubMed
- ASCEND bleeding outcomes in diabetes (NEJM 2018) — PubMed PMID 30146931
Live PubMed Searches
- Aspirin gastrointestinal bleeding
- Aspirin intracranial hemorrhage
- Aspirin H. pylori ulcer
- Aspirin NSAID drug interaction bleeding
- Aspirin perioperative management
Connections
- Aspirin Benefits Hub
- Cardiovascular Prevention
- Colorectal Cancer Risk
- Low Dose vs Full Dose
- Aspirin Side Effects
- Aspirin and Kidneys
- Aspirin Main Hub
- Gastroenterology
- Cardiology
- All Remedies