Low Dose vs Full Dose Aspirin
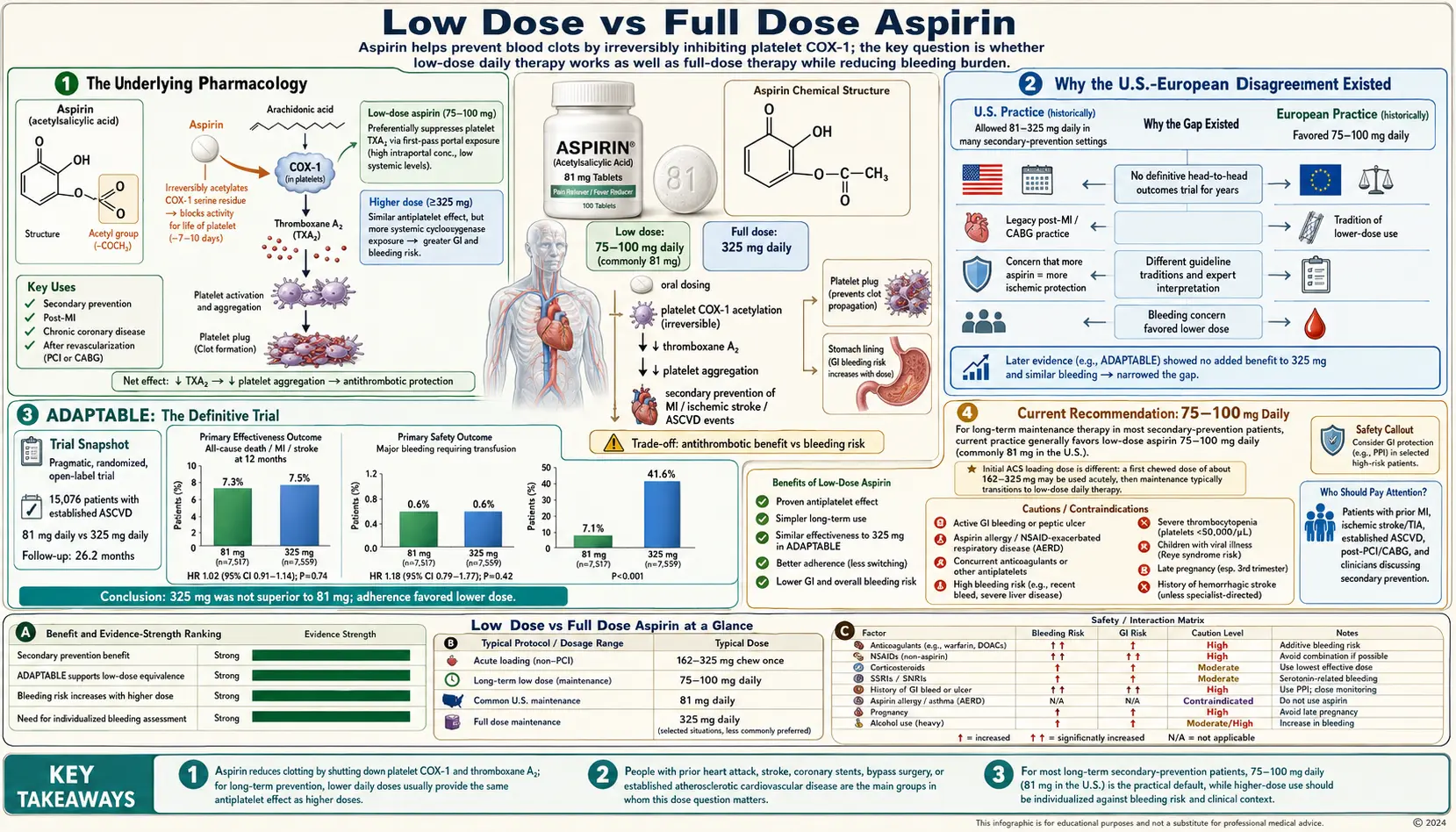
For 50 years, U.S. cardiologists prescribed 325 mg "regular" aspirin for cardiovascular prevention while European cardiologists prescribed 75-100 mg. Both groups argued from observational and mechanistic data that their dose was optimal. The question was finally settled in 2021 by the ADAPTABLE trial (PMID 33999547), which directly compared 81 mg and 325 mg in 15,076 patients with established atherosclerotic cardiovascular disease — finding no difference in cardiovascular events or major bleeding over a median 26 months of follow-up. The result confirms what mechanistic studies had long suggested: aspirin's platelet COX-1 inhibition is saturated at doses around 75 mg daily, and higher doses produce no additional antithrombotic benefit but do increase mucosal irritation. Modern practice therefore converges on 75-100 mg daily for cardiovascular prevention, with higher doses reserved for specific non-cardiovascular indications: 325-650 mg for analgesia, 81 mg twice daily during Kawasaki disease, and full-dose 325-650 mg as the acute MI loading dose. This page walks through the pharmacology, the historical disagreement, ADAPTABLE's resolution, and the residual situations where higher doses are still indicated.
Table of Contents
- The Underlying Pharmacology
- Why the U.S.-European Disagreement Existed
- ADAPTABLE: The Definitive Trial
- Current Recommendation: 75-100 mg Daily
- Acute MI: 162.5-325 mg Loading Dose
- Enteric-Coated vs Uncoated
- Body-Weight and Dose Adjustment
- Non-CV Indications Requiring Higher Doses
- Aspirin "Resistance" and Variability
- Key Research Papers
- Connections
- Featured Videos
The Underlying Pharmacology
Aspirin's elimination half-life is about 15-20 minutes — it is rapidly hydrolyzed in plasma and the liver to salicylic acid, which has a much longer half-life (3-6 hours at low doses, 12-15 hours at higher doses due to saturable elimination). The clinically relevant pharmacodynamic effect, however, is not the plasma concentration of aspirin or salicylate, but the irreversible acetylation of platelet COX-1.
Patrono and colleagues, in their landmark NEJM 2005 review (PMID 15917386), summarized the dose-response data: 75 mg daily produces approximately 95-99% suppression of platelet thromboxane B2 production after steady state (5-7 days). Higher doses produce only marginal additional suppression. Single-dose pharmacodynamics show that 30 mg of aspirin acutely produces about 90% platelet TxA2 suppression; 162 mg produces 97%; 650 mg produces 99%. The dose-response curve is steeply saturating, with most of the platelet effect achieved by doses well below 100 mg.
This pharmacology explains why the cardiovascular benefit plateaus at low doses. The ATT 2002 meta-analysis (PMID 12096097) showed essentially flat dose-response for vascular events across 75-150 mg, 160-325 mg, and 500-1500 mg dose ranges. By contrast, GI bleeding rises monotonically with dose — the McQuaid 2006 systematic review (PMID 16490465) found GI bleeding rates of about 1.4% per year at <200 mg, 1.6% at 200-325 mg, and 2.3% at >325 mg.
Why the U.S.-European Disagreement Existed
The U.S. tradition of 325 mg daily (or 80 mg "baby aspirin" originally introduced as a pediatric fever-reducer) emerged from the earliest U.S. cardiovascular prevention trials, which used doses in the 100-325 mg range. The Physicians' Health Study (PMID 2664509) used 325 mg every other day. ISIS-2 (PMID 2899772) used 162.5 mg daily for 1 month in acute MI. The CURE trial (PMID 11519503) randomized between 75-100 mg and 200-325 mg in its aspirin background therapy.
European trials, by contrast, used lower doses (75-100 mg) more uniformly — reflecting both different aspirin tablet sizes available (75 mg is the standard small tablet in many European countries, vs 81 mg in the U.S.) and different early-mechanism work emphasizing the saturating dose-response.
Multiple observational and head-to-head comparisons accumulated through the 1990s and 2000s suggesting low-dose was equivalent in efficacy with less bleeding. The 2011 CURRENT-OASIS 7 trial directly compared 75-100 mg vs 300-325 mg in ACS patients and found no difference in cardiovascular outcomes but increased major bleeding with the higher dose. The 2008 AHA scientific statement (PMID 18768461) endorsed 75-100 mg as the preferred chronic dose, but U.S. cardiologists continued to prescribe 325 mg as a holdover from earlier trials.
ADAPTABLE: The Definitive Trial
The ADAPTABLE trial (Aspirin Dosing — A Patient-centric Trial Assessing Benefits and Long-term Effectiveness; PMID 33999547) was a pragmatic, open-label, randomized trial of 15,076 patients with established atherosclerotic cardiovascular disease (prior MI, prior stroke/TIA, prior coronary revascularization, peripheral arterial disease, or coronary calcium score >400). Patients were randomized to 81 mg or 325 mg aspirin daily and followed for a median 26.2 months for the primary composite outcome of death, hospitalization for MI, or hospitalization for stroke.
Primary outcome: 7.28% in the 81 mg group and 7.51% in the 325 mg group (hazard ratio 1.02, 95% CI 0.91-1.14). Major bleeding requiring transfusion was also similar (0.63% vs 0.60%). There was no detectable difference in any clinical outcome.
An important methodological note: ADAPTABLE was pragmatic with patient-reported dose adherence, and substantial crossover occurred (41.6% of the 325 mg group switched to 81 mg over the trial, while only 7.1% of the 81 mg group switched to 325 mg). This crossover pattern itself reflects clinical practice convergence on the lower dose and was one of the reasons the trial leadership communicated the null result with confidence: even with crossover diluting any potential dose-effect difference, the as-treated analyses also showed no benefit difference.
ADAPTABLE settled the question. Subsequent guideline updates (including the 2022 USPSTF recommendation and updated ACC/AHA documents) consistently endorse 81 mg daily as the standard dose for chronic cardiovascular prevention.
Current Recommendation: 75-100 mg Daily
The modern recommendation for chronic cardiovascular prevention (either secondary prevention with established disease, or the narrow primary-prevention indications described in the Cardiovascular Prevention deep-dive) is 75-100 mg daily. In the United States, this is essentially always 81 mg (the standard "low-dose" or "baby" aspirin tablet). In Europe and most of the rest of the world, the standard low-dose tablet is 75 mg or 100 mg.
The numerical difference between 75, 81, and 100 mg is clinically meaningless — all three produce essentially complete platelet COX-1 inhibition at steady state. The choice is driven by tablet availability rather than any documented benefit difference.
For dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) after acute coronary syndrome or coronary stent, the aspirin component is also 75-100 mg daily, with the P2Y12 inhibitor providing the additional antiplatelet effect.
Acute MI: 162.5-325 mg Loading Dose
The exception to "always 81 mg" is the acute MI or acute coronary syndrome loading dose. When acute MI is suspected, an immediate dose of 162.5-325 mg should be chewed and swallowed (chewable formulation is preferred to accelerate absorption through the buccal mucosa). The higher loading dose ensures rapid, complete platelet inhibition at the moment of acute thrombus formation when even a few minutes of inhibition delay can mean more myocardial necrosis.
After the loading dose, the chronic 81 mg daily dose is sufficient. The mistake to avoid: telling patients to swallow an enteric-coated 81 mg tablet during suspected MI. Enteric coating delays therapeutic platelet inhibition by 1-2 hours, which can be life-altering during acute coronary thrombosis. Chewed uncoated aspirin acts within minutes.
For acute ischemic stroke, the analogous loading dose is 160-300 mg given within 48 hours of symptom onset (after intracranial hemorrhage has been excluded by CT). Daily 81 mg is then continued.
Enteric-Coated vs Uncoated
Enteric coating is a polymer film designed to delay tablet dissolution until the tablet reaches the small intestine, in theory reducing direct gastric mucosal irritation. The clinical-effect literature is mixed: enteric coating may modestly reduce minor dyspepsia symptoms, but does not clearly reduce major GI bleeding rates (because the bleeding mechanism is predominantly systemic, not local).
The Maree 2005 JACC paper (PMID 16139140) and subsequent work have documented that enteric-coated aspirin produces lower and more variable peak platelet inhibition compared with uncoated formulations, particularly in obese patients and in those with rapid gastric emptying. This raises a concern that enteric coating could contribute to apparent "aspirin resistance."
For chronic prevention in patients who tolerate uncoated aspirin without significant dyspepsia, plain uncoated low-dose aspirin is likely preferable. For acute MI, chewable uncoated aspirin is essential. Enteric-coated formulations remain reasonable for patients with significant GI symptoms on uncoated aspirin, with the understanding that PPI co-therapy (in those with bleeding risk factors) is the more effective intervention for reducing serious GI complications than enteric coating alone.
Body-Weight and Dose Adjustment
The Rothwell 2018 Lancet paper (PMID 30017552) reported a post-hoc analysis of body-weight effect on aspirin response across multiple primary-prevention trials. Low-dose aspirin (75-100 mg) appeared effective in adults weighing <70 kg but not in those weighing ≥70 kg, where higher doses (300-325 mg) were associated with better cardiovascular outcomes. The proposed mechanism is dilution of the fixed dose across larger circulating plasma volumes.
This finding is intriguing but has not been incorporated into guideline recommendations. It conflicts with the saturation pharmacology of platelet COX-1 inhibition, where 75-100 mg should fully inhibit platelets regardless of body weight. Confirmation in prospective randomized trials is needed before clinical practice should change. For now, 81 mg remains the default chronic dose regardless of body weight.
Non-CV Indications Requiring Higher Doses
- Analgesia and anti-pyresis — 325-650 mg every 4-6 hours (max 4 g/day) for adult pain or fever. This is the original 19th-century indication, now largely supplanted by acetaminophen and ibuprofen due to better tolerability.
- Anti-inflammatory dosing (rheumatic conditions) — historically 2400-4000 mg per day in divided doses, but rarely used in modern rheumatology due to better-tolerated NSAIDs and disease-modifying agents.
- Kawasaki disease (acute febrile vasculitis in children) — high-dose aspirin (30-80 mg/kg/day in 4 divided doses, depending on era and protocol) during the acute febrile phase, then transition to low-dose 3-5 mg/kg/day for the convalescent phase to provide antiplatelet protection during coronary aneurysm risk window. See Newburger 2004 AHA guideline (PMID 15505111).
- Polycythemia vera — 100 mg daily was shown effective in the ECLAP trial (PMID 14711909) for reducing thrombosis without unacceptable bleeding.
- Pregnancy preeclampsia prevention — 81 mg or 100 mg daily from 12-16 weeks gestation to delivery, in women at elevated preeclampsia risk. This is a low-dose indication, but worth noting separately because the indication is so different from cardiovascular prevention.
- Carotid endarterectomy — 81 to 325 mg pre-operatively per surgeon preference, then standard 81 mg post-operatively.
Aspirin "Resistance" and Variability
"Aspirin resistance" refers to either pharmacodynamic failure (laboratory evidence that platelet COX-1 is not fully inhibited despite standard aspirin therapy) or clinical failure (recurrent cardiovascular events despite aspirin therapy). The literature is heterogeneous because the term has been used both ways.
Pharmacodynamic resistance is uncommon (1-5% of patients on standard low-dose aspirin) and is often explained by poor adherence, enteric coating malabsorption, concomitant ibuprofen interference, or genetic variants in platelet receptors. The Cox 2006 Stroke paper (PMID 16690893) and the Eikelboom 2002 Circulation paper (PMID 12451000) suggested that laboratory-defined aspirin resistance was associated with worse cardiovascular outcomes, but routine platelet function testing to identify these patients has not become standard practice because the evidence for an effective alternative intervention is lacking.
Clinical failure (recurrent events on aspirin) is more common and reflects the fact that aspirin reduces but does not eliminate cardiovascular risk — even with full platelet COX-1 inhibition, atherosclerotic disease can progress and acute events can occur. In high-risk patients, dual antiplatelet therapy with a P2Y12 inhibitor provides additional risk reduction.
The practical implication: most "aspirin failure" is best addressed by confirming adherence, treating concomitant risk factors aggressively (statin, blood pressure, diabetes management), and considering escalation to DAPT in appropriate patients, rather than dose escalation of aspirin itself.
Key Research Papers
- ADAPTABLE trial (NEJM 2021): 81 mg vs 325 mg Search PubMed
- Patrono C et al., NEJM 2005: low-dose aspirin pharmacology Search PubMed
- Antithrombotic Trialists' Collaboration (BMJ 2002) — Search PubMed
- Roth GJ & Majerus PW (J Clin Invest 1975): COX-1 acetylation mechanism Search PubMed
- Vane JR (Nat New Biol 1971): aspirin and prostaglandin synthesis — PubMed PMID 5284360
- Patrono C (NEJM 1994): aspirin as antiplatelet drug review Search PubMed
- McQuaid KR & Laine L (Am J Med 2006): GI bleeding dose-response Search PubMed
- Maree AO et al., JACC 2005: enteric-coated aspirin pharmacology Search PubMed
- Newby LK et al., AHA 2008: aspirin dose scientific statement Search PubMed
- Rothwell PM et al., Lancet 2018: body-weight-dose effect Search PubMed
- Cox D et al., Stroke 2006: aspirin resistance and outcomes Search PubMed
- Eikelboom JW et al., Circulation 2002: aspirin resistance and clinical outcomes Search PubMed
- Newburger JW et al., AHA 2004: Kawasaki disease aspirin dosing Search PubMed
- Landolfi R et al., ECLAP trial NEJM 2004: aspirin in polycythemia vera Search PubMed
- ISIS-2 trial (Lancet 1988): aspirin loading dose in acute MI — PubMed PMID 2899772
Live PubMed Searches
- Aspirin dose cardiovascular prevention
- Aspirin 81 vs 325 mg comparison
- Aspirin enteric-coated absorption
- Aspirin resistance and platelet response
- Aspirin pharmacology and thromboxane
Connections
- Aspirin Benefits Hub
- Cardiovascular Prevention
- Colorectal Cancer Risk
- Bleeding Risks and Cautions
- Aspirin Heart Attack Prevention
- Aspirin Stroke Prevention
- Aspirin Main Hub
- Cardiology
- Heart Attack
- All Remedies