Aspirin and Colorectal Cancer Risk
Aspirin is the only drug for which a randomized controlled trial has demonstrated a statistically significant reduction in cancer incidence and cancer mortality in unselected adults. The Rothwell pooled analyses (PMID 20970847, PMID 21144578) of four long-term aspirin trials, totaling about 25,000 patients with up to 20 years of follow-up, established a 24% reduction in colorectal cancer incidence and a 35% reduction in colorectal cancer mortality after 5+ years of daily aspirin use. The CAPP2 trial (PMID 22122850, PMID 32534647) confirmed the benefit in Lynch syndrome carriers, where the genetic background makes the signal especially clear. Mechanism: aspirin inhibits cyclooxygenase-2 (COX-2) in colonic epithelium, reducing prostaglandin E2 production that otherwise drives epithelial proliferation, angiogenesis, and resistance to apoptosis. The latency requirement (benefit emerges only after 5-10 years of continuous use) creates a fundamental scheduling problem: it must be started early enough that the user lives long enough to accrue the benefit, but bleeding risk rises sharply with age. This page walks through the evidence, the proposed mechanisms, and the modern integration into chemoprevention strategy.
Table of Contents
- The Original Epidemiologic Signal
- Rothwell Pooled Analyses (2010-2011)
- CAPP2 Trial in Lynch Syndrome
- Mechanism: COX-2 and Prostaglandin E2 in Colonic Epithelium
- The Latency Requirement (5-10 Years)
- Dose-Response: Low-Dose Sufficient
- Aspirin After Colorectal Cancer Diagnosis
- Other Cancers: Smaller and Less Consistent Signals
- Current Guideline Status
- Key Research Papers
- Connections
- Featured Videos
The Original Epidemiologic Signal
The first hint that aspirin might reduce colorectal cancer came from a 1988 case-control study in Melbourne (Kune, Kune, and Watson) which observed lower colorectal cancer rates among aspirin users. Through the 1990s and early 2000s a series of cohort studies (the Nurses' Health Study, the Health Professionals Follow-up Study, and others) consistently observed reduced colorectal cancer risk in long-term aspirin users, with relative risks generally in the 0.6-0.8 range after 10+ years of use.
Chan and colleagues at Harvard, using prospective data from the Nurses' Health Study (PMID 16091571), showed a dose-response relationship: women taking 2-5 standard aspirin tablets (325 mg) per week had about a 21% reduced colorectal cancer risk, while those taking 6-14 per week had a 38% reduction. The benefit emerged only after 10 years of consistent use — a critical observation that would later be confirmed by the randomized trial latency analyses.
These observational findings were considered suggestive but not definitive, because aspirin users differ from non-users in many ways (likely better access to medical care, more attention to symptoms, different cardiovascular risk profiles) that observational adjustment cannot fully eliminate. The randomized trial confirmation that came in 2010 transformed the evidence base.
Rothwell Pooled Analyses (2010-2011)
Peter Rothwell at Oxford performed pooled individual-patient-data analyses of randomized aspirin trials originally designed for cardiovascular outcomes. By extracting cancer incidence and cancer mortality data from these trials (with up to 20 years of follow-up via cancer registry linkage), he was able to provide randomized-trial evidence for the aspirin cancer-prevention signal.
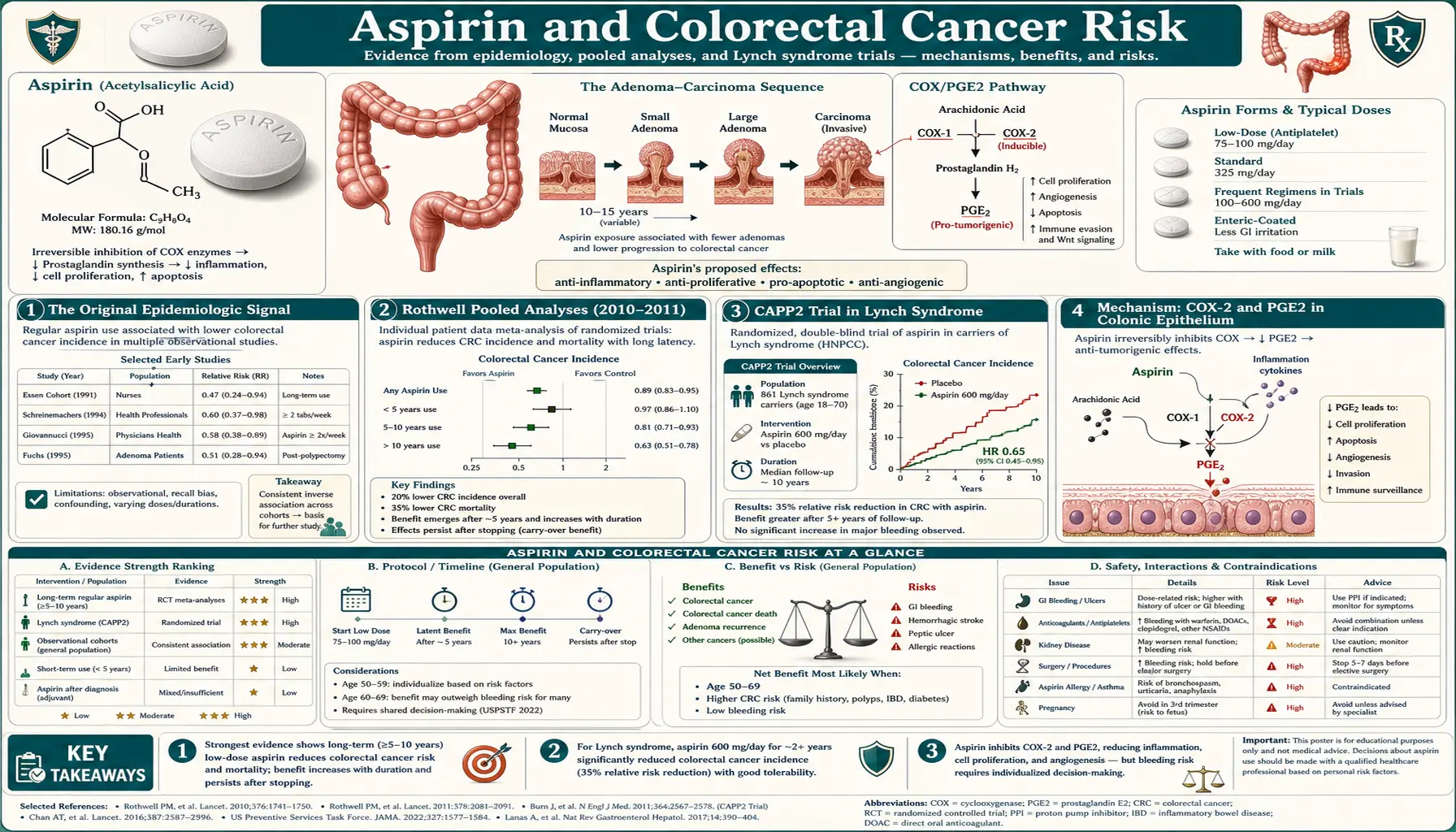
The first Lancet paper (PMID 20970847, 2010) pooled 4 trials (TPT, UK-TIA, BDAT, SALT) of aspirin given for primary or secondary cardiovascular prevention. With a median 18.3 years of follow-up, daily aspirin reduced colorectal cancer incidence by 24% (hazard ratio 0.76, 95% CI 0.60-0.96) and colorectal cancer mortality by 35% (hazard ratio 0.65, 95% CI 0.48-0.88). The benefit was concentrated in the proximal colon (right-sided cancers), with hazard ratio 0.45 for proximal disease and a non-significant effect on distal colon and rectum.
The 2011 Lancet paper (PMID 21144578) extended the analysis to all cancer mortality across 8 trials and 25,570 patients. Daily aspirin reduced 20-year all-cancer mortality by 20%, with reductions in esophageal (60%), pancreatic (35%), brain (35%), lung adenocarcinoma (30%), and colorectal cancer mortality. Benefits required 5+ years of daily use; the longer the use, the larger the absolute mortality reduction. Doses as low as 75 mg daily were sufficient — higher doses did not produce greater benefit but did produce more bleeding.
These findings represent the strongest evidence base for any pharmacologic cancer-chemoprevention agent. The 2012 Algra and Rothwell Lancet Oncology paper (PMID 22440112) further extended the analysis to cancer metastasis: aspirin reduced the risk of metastatic spread of adenocarcinomas by ~36%, suggesting an effect not only on tumor initiation/progression but on the metastatic cascade itself.
CAPP2 Trial in Lynch Syndrome
Lynch syndrome (hereditary nonpolyposis colorectal cancer, HNPCC) is caused by germline mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, PMS2). Carriers have a lifetime colorectal cancer risk of approximately 50-80%. Because the genetic background creates a high baseline risk, chemoprevention trials in this population can achieve statistical power with smaller sample sizes and shorter follow-up than primary-prevention trials in the general population.
The CAPP2 trial (Colorectal Adenoma/carcinoma Prevention Programme 2; PMID 22122850) was an international randomized double-blind trial in 861 Lynch syndrome carriers, randomized to 600 mg aspirin daily or placebo. After a mean 55.7 months of intervention plus extended follow-up, aspirin reduced colorectal cancer incidence by 35-44% (depending on the analysis), with the benefit not appearing until after 5 years of follow-up. The dose was deliberately higher than the cardioprotective range, reflecting earlier thinking about dose requirements; subsequent analyses suggest lower doses likely produce similar benefit.
The CAPP2 10-year follow-up paper (PMID 32534647, 2020) confirmed the durability of the effect: a single 2.5-year course of 600 mg daily aspirin (taken between 25 and 55 years of age in most participants) produced a 50% reduction in colorectal cancer incidence 10 years later. This delayed, durable effect is unusual in chemoprevention and points to aspirin acting on early-stage adenoma transformation rather than late-stage tumor growth.
CAPP3, an ongoing follow-up trial, is testing different doses (100 mg, 300 mg, 600 mg) in Lynch carriers to identify the lowest effective dose.
Mechanism: COX-2 and Prostaglandin E2 in Colonic Epithelium
The leading mechanistic explanation centers on cyclooxygenase-2 (COX-2). COX-2 is the inducible isoform of cyclooxygenase, expressed at low levels in healthy tissue but upregulated dramatically in inflammation and in many epithelial tumors. Colorectal adenomas and carcinomas show 5-50-fold elevated COX-2 expression compared with normal colonic mucosa, and the degree of overexpression correlates with adenoma size, dysplasia grade, and likelihood of progression.
The downstream product, prostaglandin E2 (PGE2), promotes several pro-tumor processes in colonic epithelium:
- Increased cell proliferation via EP2/EP4 receptor signaling.
- Decreased apoptosis (resistance to programmed cell death).
- Promotion of angiogenesis (new blood vessel growth supplying the developing tumor).
- Immunosuppression in the tumor microenvironment (suppressing CD8 T-cell anti-tumor responses, promoting M2 tumor-associated macrophage polarization).
- Increased invasiveness via matrix metalloproteinase upregulation.
Aspirin's inhibition of COX-2 reduces tumor PGE2 production. Because aspirin acetylates COX irreversibly, even the low circulating concentrations achieved with 75-100 mg daily produce sustained partial COX-2 inhibition in rapidly dividing tissues like colonic epithelium. Additional mechanisms have been proposed, including direct effects on NF-κB signaling, induction of apoptosis via mitochondrial pathways, effects on Wnt/β-catenin signaling (a key driver of colorectal carcinogenesis), and platelet-mediated effects (platelets contribute to tumor metastasis, and aspirin's antiplatelet effect may reduce metastatic spread).
The Drew, Cao, and Chan 2016 Nature Reviews Cancer review (PMID 27009395) provides the canonical summary of the mechanistic data.
The Latency Requirement (5-10 Years)
The most clinically consequential feature of the aspirin-colorectal cancer relationship is the latency requirement. Across the Rothwell pooled analyses and the observational studies, the cancer-prevention benefit does not appear in the first 5 years of use; it emerges between years 5 and 10 and continues to accumulate. This time course is biologically plausible — aspirin appears to act on the early stages of adenoma initiation and transformation, and 5-10 years is the typical adenoma-to-carcinoma sequence.
The latency requirement collides with two clinical realities. First, bleeding risk increases sharply with age. A patient who starts aspirin at age 70 is unlikely to accrue full cancer-prevention benefit before age 80, by which time bleeding risk has roughly doubled. Second, the ASPREE trial (where median age at enrollment was 74 and follow-up was only 4.7 years) likely captured the bleeding harms without yet capturing the cancer-prevention benefit, partly explaining the unexpected mortality signal in that trial. Whether ASPREE extended follow-up will eventually show emerging cancer-prevention benefit is being actively studied.
For practical chemoprevention, the latency requirement implies that aspirin must be started at a younger age (typically 40s-50s) and continued for decades to extract the colorectal cancer benefit. This horizon also aligns with the USPSTF's 2022 restriction of primary prevention to adults aged 40-59, where remaining life expectancy is long enough to make the latency tractable.
Dose-Response: Low-Dose Sufficient
The Rothwell pooled analyses found that doses as low as 75 mg daily were sufficient for the cancer-prevention benefit, and that higher doses (300-600 mg) did not produce greater benefit. This is the same dose-response pattern as the antiplatelet effect — saturated at 75-100 mg — and is consistent with the platelet-mediated metastasis hypothesis as well as with steady-state inhibition of COX-2 in rapidly turning over epithelium.
The 2018 Lancet paper by Rothwell and colleagues on aspirin body-weight-dose interaction (PMID 30017552) suggested that low-dose (75-100 mg) aspirin produced cardiovascular and cancer benefits in lower-weight individuals (<70 kg) but not in higher-weight individuals, raising the possibility that some patients require dose escalation. This finding has not yet changed guideline recommendations and requires confirmation.
Aspirin After Colorectal Cancer Diagnosis
Chan et al. published an influential 2009 JAMA paper (PMID 19690313) showing that patients who began regular aspirin use after colorectal cancer diagnosis had improved survival, particularly in those with COX-2-positive tumors. Subsequent observational studies and meta-analyses have confirmed the post-diagnosis benefit, with relative risk reductions in colorectal cancer-specific mortality of 25-30% in regular aspirin users.
Several ongoing randomized trials are testing whether to formalize this into post-diagnosis chemoprevention. ASCOLT (Aspirin for Dukes C and High-Risk Dukes B Colorectal Cancers) and ADD-ASPIRIN are large adjuvant trials in early colorectal cancer; the results, expected through the mid-2020s, will inform whether aspirin should be added to standard adjuvant therapy.
Other Cancers: Smaller and Less Consistent Signals
Beyond colorectal cancer, the aspirin cancer-prevention signal is smaller and less consistent. The Rothwell 2011 pooled analysis (PMID 21144578) showed reductions in esophageal, pancreatic, brain, and lung adenocarcinoma mortality at 20 years of follow-up. Esophageal cancer mortality reduction (~60%) was the largest, possibly reflecting reduced Barrett's esophagus progression. Pancreatic cancer mortality reduction was substantial but is harder to act on clinically because there is no chemoprevention indication for this rare cancer.
For prostate cancer, the Mahmud 2010 JNCI paper (PMID 20668233) and subsequent analyses suggest a small reduction in prostate cancer mortality with long-term aspirin use, but the effect is smaller than for colorectal cancer and not consistently found.
For breast cancer, observational data have been mixed, with some studies suggesting benefit (especially in postmenopausal women with hormone receptor-positive tumors) and others showing no effect. The randomized trial evidence is too sparse to draw strong conclusions.
For these reasons, colorectal cancer remains the primary cancer-prevention indication being discussed in chemoprevention guidelines.
Current Guideline Status
The 2016 USPSTF recommendation (PMID 27064677) was the first major guideline to incorporate colorectal cancer prevention into its aspirin recommendation rationale. It suggested aspirin for adults 50-59 with elevated cardiovascular risk who were willing to take aspirin for at least 10 years and at low bleeding risk — with the colorectal cancer benefit explicitly cited as part of the favorable benefit-harm balance.
The 2022 USPSTF recommendation (PMID 35471505) substantially restricted this. The 2018 trials had not changed the cancer-prevention evidence base, but they had weakened the cardiovascular benefit in primary prevention. The USPSTF concluded that the colorectal cancer benefit alone was not sufficient to recommend population-level aspirin use; the chemoprevention indication is best discussed in the context of individual cardiovascular risk and bleeding risk.
Cuzick et al. (PMID 25096604) published an influential 2015 Annals of Oncology benefit-risk modeling analysis suggesting that for adults aged 50-65, 10 years of daily aspirin reduces colorectal cancer incidence by 35% and mortality by 40%, with all-cancer mortality reductions of 7-9% in women and 9-15% in men, weighed against bleeding-related mortality of ~1%. The model conclusion was that the benefit-risk ratio favors aspirin in this age range for those at moderately elevated cardiovascular and cancer risk.
For Lynch syndrome carriers specifically, professional society guidelines (NCCN, European hereditary cancer guidelines) now recommend offering aspirin chemoprevention based on the CAPP2 data, with patient-individualized dose selection pending the CAPP3 results.
Key Research Papers
- Rothwell PM et al., Lancet 2010 — long-term aspirin and CRC incidence/mortality — PubMed PMID 20970847
- Rothwell PM et al., Lancet 2011 — effect of daily aspirin on 20-year cancer mortality — PubMed PMID 21144578
- Algra AM & Rothwell PM, Lancet Oncol 2012 — aspirin and cancer metastasis — PubMed PMID 22440112
- Burn J et al., CAPP2 trial Lancet 2011 — Lynch syndrome carriers Search PubMed
- Burn J et al., CAPP2 10-year follow-up Lancet 2020 — PubMed PMID 32534647
- Chan AT et al., JAMA 2005 — aspirin dose and CRC in women (NHS) — Search PubMed
- Chan AT et al., JAMA 2009 — aspirin and survival after CRC diagnosis Search PubMed
- Cole BF et al., NEJM 2003 — aspirin for prevention of colorectal adenomas Search PubMed
- Baron JA et al., NEJM 2003 — low-dose aspirin and adenoma prevention Search PubMed
- Cuzick J et al., Annals of Oncology 2015 — benefit-risk modeling Search PubMed
- Drew DA et al., Nature Reviews Cancer 2016 — mechanism review — PubMed PMID 27009395
- Mahmud SM et al., JNCI 2010 — aspirin and prostate cancer mortality Search PubMed
- Bibbins-Domingo K, USPSTF 2016 modeling Search PubMed
- USPSTF 2022 aspirin recommendation — PubMed PMID 35471505
- ASPREE primary outcome (NEJM 2018) — aspirin in older adults — PubMed PMID 30221597
Live PubMed Searches
- Aspirin colorectal cancer prevention
- Aspirin colorectal adenoma
- Aspirin COX-2 colon cancer
- Aspirin Lynch syndrome
- Aspirin cancer chemoprevention meta-analysis
Connections
- Aspirin Benefits Hub
- Cardiovascular Prevention
- Bleeding Risks and Cautions
- Low Dose vs Full Dose
- Aspirin Cancer Prevention
- Aspirin Main Hub
- Oncology
- Gastroenterology
- Colonoscopy
- Colorectal Cancer — the disease itself: staging, screening, symptoms and treatment behind the chemoprevention data on this page.
- All Remedies