Molybdenum Toxicity: What the Evidence Shows
Here is the honest bottom line first: in everyday life, molybdenum toxicity in humans is rare. Molybdenum is an essential trace mineral, but the amount you get from food — mostly from beans, grains, and nuts — is nowhere near a harmful dose, and your kidneys are very good at flushing out any excess in the urine. There is no recognized syndrome of "molybdenum poisoning" from a normal diet. The few real signals of harm come from unusual situations: people living where the soil is extraordinarily rich in molybdenum, certain industrial exposures, and the occasional misuse of high-dose supplements. Even then, the picture is mostly mild — the best-documented effect in people is a gout-like rise in uric acid with achy joints. The clearest, most predictable risk is not toxicity at all in the usual sense but a slow squeeze on copper: high molybdenum, especially with high sulfur, can drive copper down, which is exactly why a molybdenum-based drug is used on purpose to treat copper overload in Wilson's disease. This page lays out, candidly, what the evidence actually supports — and what it does not — so you are neither alarmed by a non-problem nor blind to the narrow situations that genuinely matter. This is not a common clinical problem; most people never need to think about it.
Table of Contents
- What the Evidence Actually Says
- Why Toxicity Is So Uncommon (The Biology)
- The Real Risk: Molybdenum vs. Copper
- Who, If Anyone, Is at Risk
- The Numbers: Intakes, Limits, and Context
- What to Do (Practical, Low-Key)
- When to Seek Care / Red Flags
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
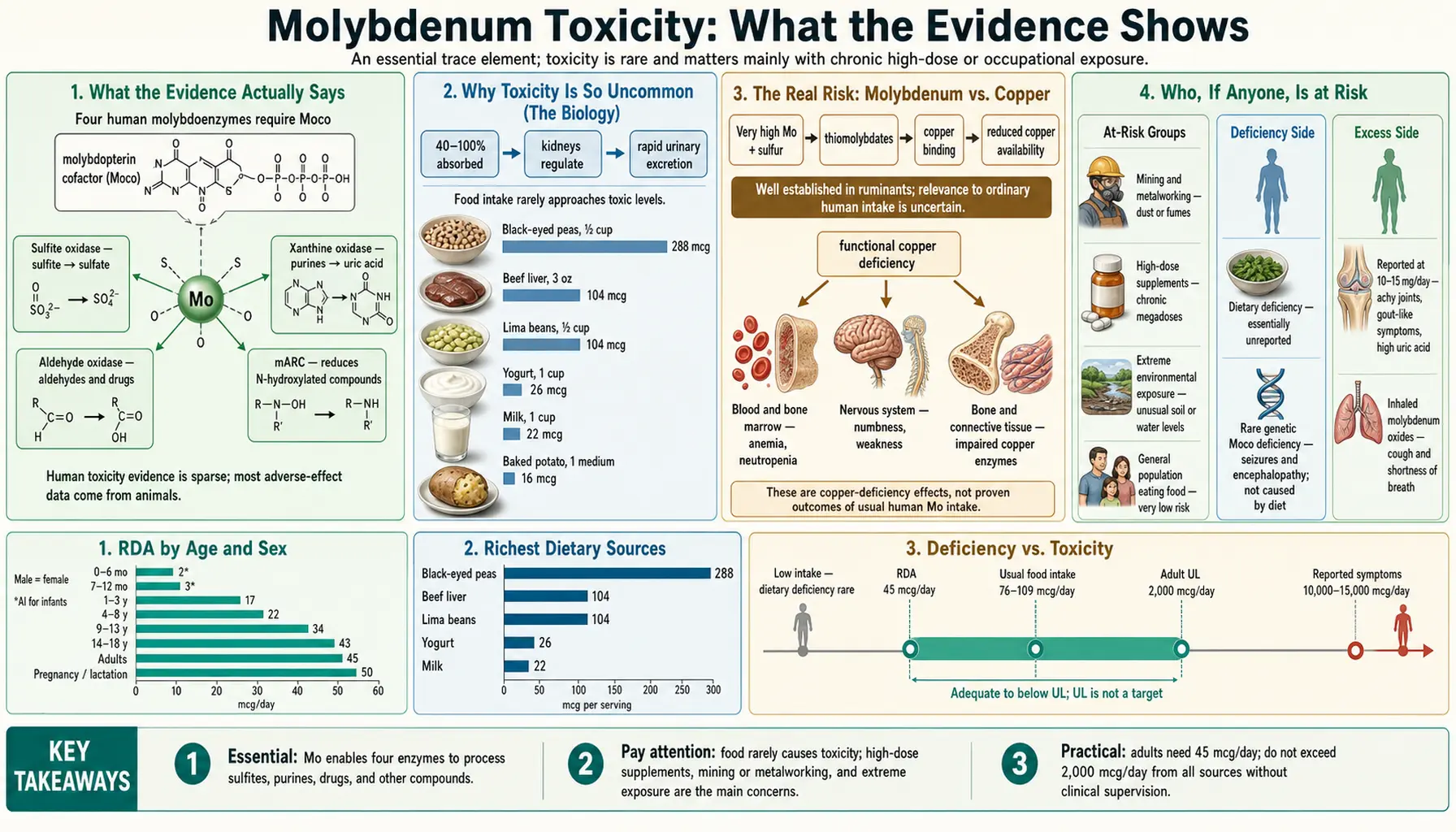
What the Evidence Actually Says
It is worth stating plainly, because health writing about trace minerals so often drifts toward alarm: there is no well-established human syndrome of molybdenum poisoning from food, and clinically meaningful molybdenum toxicity is uncommon even from supplements. Major reviews that have scoured the literature reach the same conclusion — the toxicity of molybdenum compounds in humans appears to be relatively low. When the European Food Safety Authority, the U.S. Institute of Medicine, and the Nordic Nutrition Recommendations each examined molybdenum, all three noted the same thing: the data on actual harm in people are thin, and the safety limits that exist lean heavily on animal experiments rather than human cases.
That does not mean "anything goes." It means the honest summary has three parts, and it helps to hold all three at once:
- From a normal diet: effectively no risk. A typical diet supplies on the order of 75–250 micrograms (µg) of molybdenum a day. Healthy people excrete extra molybdenum so efficiently in urine that food-based intake has never been shown to cause harm. You cannot "overdose" on molybdenum by eating beans and oats.
- From extreme environmental or occupational exposure: a real but mostly mild signal. The single most-cited human example comes from a region of Armenia where the soil is unusually high in molybdenum and residents took in roughly 10–15 milligrams (mg) a day — dozens of times a normal intake. Those people reported achy, gout-like joints and had elevated blood uric acid. Workers with heavy industrial molybdenum exposure have reported similar joint complaints and raised uric acid, plus non-specific symptoms like fatigue and headache. These are genuine observations, but they describe discomfort and an altered lab value, not a dramatic poisoning.
- From high-dose supplements: rare, and the worst reports are debated. There is essentially one widely-quoted case report of a man who took a molybdenum supplement (a cumulative 13.5 mg over 18 days) and developed seizures and hallucinations. It is a real published case, but it is a single, atypical report at a dose below the official safety ceiling, and whether molybdenum truly caused the neurological damage remains uncertain and disputed. It is a cautionary footnote, not a typical outcome — and it is a reason not to megadose supplements, not a reason to fear the mineral.
So the candid verdict is: molybdenum is one of the safer trace minerals, the clearest documented human effect of excess is a gout-like uric-acid rise, and the most predictable downside of chronically high molybdenum is its effect on copper — which we cover in its own section below.
Why Toxicity Is So Uncommon (The Biology)
Why is a mineral that is biologically active — molybdenum sits at the heart of several enzymes — nonetheless so hard to overdo? The answer is mostly about plumbing. Think of your body's molybdenum like water in a sink with the tap and the drain both wide open: the more you pour in, the faster it runs out, so the level in the basin barely rises.
Carefully controlled balance studies make this concrete. When researchers fed healthy young men molybdenum across a wide range of intakes — from very low to about 1,500 µg a day — the men absorbed molybdenum efficiently (around 88–93%), but the amount and fraction they passed in urine rose right along with intake. In other words, the kidney acts as a fast, demand-driven release valve: when intake is low, the body holds on; when intake climbs, urinary losses climb to match, keeping blood levels in a tight band. This homeostatic release is the single biggest reason ordinary dietary molybdenum almost never accumulates to a harmful level.
A few related details round out the picture:
- More soluble forms are more bioavailable — and more able to cause trouble. Soluble molybdate (the form in food and most supplements) is well absorbed; poorly soluble industrial forms are not. This is why the rare problems cluster around either highly soluble dietary excess (the Armenian soil) or specific industrial compounds, not around, say, eating ordinary food.
- The enzymes it serves are not "overdriven" by extra molybdenum. Molybdenum works as part of a small helper molecule called the molybdenum cofactor, which a handful of enzymes use — most relevantly sulfite oxidase (which detoxifies sulfite, a topic covered on the Sulfite Metabolism page) and xanthine oxidase (which makes uric acid). Adding more molybdenum does not endlessly speed these enzymes up; the cofactor and enzyme amounts are themselves regulated. The one place extra activity shows up measurably is uric acid, via xanthine oxidase — which is exactly the gout-like effect seen in true overexposure.
- There is no useful "molybdenum status" test in routine medicine. Because the body holds molybdenum in such a narrow range and there is no sensitive everyday marker, doctors do not screen for molybdenum levels the way they do for iron or vitamin D. The practical consequence is reassuring: there is rarely anything to measure because there is rarely anything wrong.
Put simply, the same machinery that makes molybdenum deficiency almost unheard of in healthy people — tight regulation plus easy excretion — also makes toxicity hard to reach. The body treats molybdenum like a guest it neither hoards nor lets pile up.
The Real Risk: Molybdenum vs. Copper
If molybdenum has one genuinely important interaction worth understanding, this is it. High molybdenum can lower copper, an essential mineral in its own right, and this copper-lowering effect is the most predictable and best-understood consequence of molybdenum excess. It is so reliable, in fact, that medicine has turned it into a treatment.
The mechanism is a chemical handshake. In the gut and bloodstream — especially when sulfur is also abundant — molybdenum can combine with sulfur to form compounds called thiomolybdates. These latch tightly onto copper and bind it up into a complex the body cannot use or absorb. The clearest example of this was first noticed not in people but in grazing animals: cattle and sheep on pastures high in molybdenum (and sulfur) develop a copper-deficiency disease historically called "teart" or "peat scours." The molybdenum was effectively starving them of copper. (This is a real and important reason livestock nutrition watches the molybdenum-to-copper ratio closely; it is far less of an issue for humans eating a varied diet.)
Doctors then borrowed the trick. Tetrathiomolybdate — a molybdenum-sulfur compound — is used as a copper-lowering drug, most notably to treat Wilson's disease, a genetic disorder in which copper accumulates dangerously in the liver and brain. It is also being studied in other copper-driven conditions. This is a striking inversion of the usual "toxin" story: here, a controlled, deliberate dose of a molybdenum compound is the medicine, precisely because of its copper-binding power. It is a clean illustration that molybdenum's most reliable systemic effect is on copper, not on direct organ damage.
What does this mean for an ordinary person? Very little, in practice. Lowering copper to a harmful degree through diet is not something a varied eater needs to worry about. But it does carry a few sensible implications:
- Do not casually megadose molybdenum supplements — particularly alongside high-sulfur regimens — on the assumption it is harmless. Sustained high molybdenum can nudge copper down, and copper deficiency has its own real consequences (anemia, low white cells, and neurological problems). Modest supplement doses within recommended ranges are not the concern; large, prolonged, self-directed doses are.
- Context determines whether copper-lowering is good or bad. In Wilson's disease, lowering copper is the goal. In a healthy person, it is an unwanted side effect to avoid. The same property is therapeutic or undesirable depending entirely on the situation — another reason supplement decisions belong with a clinician who knows your case.
- The molybdenum–copper relationship is a two-way street. For the broader story of copper — what it does, and what happens when it is too high — see Copper and Copper Toxicity.
Who, If Anyone, Is at Risk
Because everyday molybdenum toxicity is so uncommon, it is more useful to name the narrow groups in whom excess could plausibly matter than to imply a broad public risk. If you are not in one of these categories — and most people are not — this is simply not your problem to manage.
- People in rare high-molybdenum environments. The classic example is a population living where the soil and locally-grown food carry extraordinarily high molybdenum, pushing intake into the 10–15 mg/day range. This is a geological accident, not a typical diet, and it is the strongest human evidence for the gout-like uric-acid effect.
- Workers with heavy occupational exposure. Mining, metalworking, and certain manufacturing processes can expose workers to molybdenum dusts or fumes. Reports from such settings describe raised uric acid, joint aches, and non-specific complaints (fatigue, headache, back pain). Workplace safety limits exist for exactly this reason, and respiratory exposure is handled through occupational-health controls rather than diet.
- People taking high-dose molybdenum supplements without medical guidance. Standard multivitamins and modest molybdenum supplements are not the issue; the concern is large, self-prescribed doses taken for long periods — sometimes marketed for "detox," "candida," or "sulfite sensitivity." The rare serious case report involved a supplement, and the more realistic risk from sustained high intake is the slow copper-lowering effect described above.
- People with reduced kidney function — a reasonable caution, not a documented epidemic. Because the kidney is the main exit route for molybdenum, it is biologically sensible that significantly impaired kidneys could clear it less well. Hard human evidence of molybdenum toxicity specifically from kidney disease is limited, but it is a logical reason for anyone with significant kidney impairment to be cautious with high-dose mineral supplements generally and to follow their clinician's advice. (See Kidney Function tests.)
- A separate, important clarification — molybdenum cofactor problems are genetic, not dietary. There is a rare, severe inherited disease called molybdenum cofactor deficiency, in which a baby cannot make the molybdenum-containing cofactor at all. This is a genetic disorder of too little functioning cofactor, not molybdenum toxicity, and it is not caused by anything in the diet. It is mentioned here only to prevent confusion: searching "molybdenum" and "brain damage" can surface this condition, which has nothing to do with eating or supplementing molybdenum.
The honest framing for everyone else is anticlimactic on purpose: if you eat a normal varied diet, are not occupationally exposed, and are not megadosing a supplement, molybdenum toxicity is not a realistic concern for you.
The Numbers: Intakes, Limits, and Context
It helps to anchor the discussion in actual figures, because the gap between a normal intake and a worrying one is enormous — and that gap is itself the reassurance.
- Typical dietary intake: roughly 75–250 µg/day in most Western diets, with legumes (beans, lentils, peas), whole grains, and nuts the leading sources. The adult Recommended Dietary Allowance is just 45 µg/day, so ordinary eaters comfortably meet their needs without trying.
- The Tolerable Upper Intake Level (UL): the U.S. Institute of Medicine set an adult UL of 2 mg/day (2,000 µg/day) — about 8 to 40 times a normal intake. Crucially, this limit was derived from reproductive and growth effects in laboratory animals, not from harm observed in people, and more recent work has not consistently reproduced those animal effects. The UL is therefore a deliberately cautious ceiling, not a cliff edge where harm begins.
- The Armenian high-exposure population: intake of about 10–15 mg/day — roughly 50 to 200 times normal — was associated with the gout-like, high-uric-acid picture. This is the kind of sustained, extreme exposure it takes to produce a clear human effect.
- Toxicological perspective: a thorough human-toxicity review proposed a tolerable daily intake on the order of 0.009 mg/kg/day (about 0.6–0.7 mg/day for a typical adult) as a conservative occupational/health benchmark — again, well above what food delivers.
The takeaway from the numbers is the same as the takeaway from the biology: there is a wide, comfortable buffer between what a person normally consumes and any level associated with even mild effects. The mineral has to be pushed to many multiples of a normal intake, and usually sustained, before anything measurable happens.
What to Do (Practical, Low-Key)
Because this is not a common clinical problem, the practical advice is appropriately understated. There is no special "low-molybdenum diet" for the general public, no routine test to chase, and no reason for a healthy person eating ordinary food to do anything at all. The few sensible steps are aimed at the small group for whom excess could matter:
- Skip the molybdenum megadose. A multivitamin's small amount of molybdenum is fine. Standalone high-dose molybdenum supplements — especially those sold for vague "detox," "candida die-off," or "sulfite sensitivity" purposes — offer no proven benefit for healthy people and are the main avoidable source of excess. If a product provides molybdenum in milligrams rather than micrograms, treat that as a flag to reconsider.
- Mind the copper picture if you supplement at the high end. If, for some specific reason, you take more molybdenum than a standard supplement provides, be aware of copper. Signs that copper has dropped too low include unexplained anemia, frequent infections (low white cells), or new neurological symptoms (numbness, unsteadiness). These warrant a doctor's evaluation, which can include checking copper. (See Copper.)
- Let food do the work. The healthiest way to get molybdenum is the way nearly everyone already does — through legumes, whole grains, and nuts, which deliver plenty without any risk of excess. There is no nutritional reason to supplement molybdenum for general health.
- If you have significant kidney disease, keep high-dose mineral supplements (molybdenum included) on your clinician's radar, simply because the body's main route for clearing molybdenum is the kidney.
- Occupational exposure is a workplace-safety matter, not a diet matter. If your job involves molybdenum dusts or fumes, the protections that matter are ventilation, respiratory protection, and monitoring under occupational-health rules — not changes to what you eat.
In short: for the overwhelming majority of people, the correct action is no action. The mineral is essential, easy to get, and hard to overdo.
When to Seek Care / Red Flags
Given how uncommon molybdenum toxicity is, the realistic reasons to seek medical advice are tied to specific symptoms or situations rather than to molybdenum as such. See a clinician if you notice any of the following, particularly if you have been taking high-dose molybdenum supplements or have heavy occupational exposure:
- Gout-like joint pain — new, achy, swollen, or painful joints, which in the context of very high molybdenum intake can reflect elevated uric acid. (Uric acid is easily checked with a blood test; for the condition itself see Gout.)
- Signs that copper may be low — unexplained fatigue and pallor (anemia), frequent or unusual infections, or new neurological symptoms such as numbness, tingling, or unsteadiness, especially if you take large molybdenum doses.
- Stopping a high-dose supplement is reasonable on its own — if you have been taking a milligram-level molybdenum supplement and feel unwell, discontinuing it and discussing it with your doctor is sensible; there is no benefit that justifies pushing through symptoms.
- Any severe neurological symptom — seizures, confusion, or hallucinations — is an emergency regardless of cause. Such symptoms have many serious explanations and warrant urgent care on their own merits; molybdenum would be, at most, one rare item on a long list a doctor would consider.
The reassuring counterpoint deserves repeating: feeling fine on a normal diet is exactly what you should expect, because dietary molybdenum does not accumulate to harmful levels in healthy people. There is no symptom you need to watch for in ordinary life.
Related Topics
Molybdenum's story is best understood alongside the minerals and functions it touches. A few closely related pages add useful context:
- Molybdenum (overview) — what the mineral is, what it does, food sources, and why deficiency is essentially unheard of in healthy people.
- Copper and Copper Toxicity — the other half of the molybdenum–copper relationship; molybdenum's most reliable systemic effect is on copper.
- Sulfite Metabolism — how molybdenum's sulfite oxidase enzyme detoxifies sulfite, and why "sulfite sensitivity" is often misattributed to molybdenum status.
- Molybdenum and Uric Acid — the xanthine oxidase link that explains the one clear human effect of true molybdenum excess.
- Sulfites — the dietary additive at the center of many molybdenum supplement claims.
Key Research Papers
- Vyskočil A, Viau C (1999). Assessment of molybdenum toxicity in humans. Journal of Applied Toxicology;19(3):185-192. — DOI: 10.1002/(SICI)1099-1263(199905/06)19:3<185::AID-JAT555>3.0.CO;2-Z
- Turnlund JR, Keyes WR, Peiffer GL, Chiang G (1995). Molybdenum absorption, excretion, and retention studied with stable isotopes in young men at five intakes of dietary molybdenum. The American Journal of Clinical Nutrition;62(4):790-796. — DOI: 10.1093/ajcn/62.4.790
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA) (2013). Scientific Opinion on Dietary Reference Values for molybdenum. EFSA Journal;11(8):3333. — DOI: 10.2903/j.efsa.2013.3333
- Bjørklund G, Hilt B, Dadar M, et al. (2023). Molybdenum — a scoping review for Nordic Nutrition Recommendations 2023. Food & Nutrition Research;67:10326. — DOI: 10.29219/fnr.v67.10326
- Maiti BK, Mukherjee N (2024). Molybdenum-Copper Antagonism in Metalloenzymes and Anti-Copper Therapy. ChemBioChem;25(6):e202300679. — DOI: 10.1002/cbic.202300679
- Brewer GJ, Dick RD, Johnson V, et al. (1994). Treatment of Wilson's Disease With Ammonium Tetrathiomolybdate: I. Initial Therapy in 17 Neurologically Affected Patients. Archives of Neurology;51(6):545-554. — DOI: 10.1001/archneur.1994.00540180023009
- Schwarz G (2016). Molybdenum cofactor and human disease. Current Opinion in Chemical Biology;31:179-187. — DOI: 10.1016/j.cbpa.2016.03.016
- Schwarz G, Mendel RR, Ribbe MW (2009). Molybdenum cofactors, enzymes and pathways. Nature;460(7257):839-847. — DOI: 10.1038/nature08302
- Momčilović B (1999). A case report of acute human molybdenum toxicity from a dietary molybdenum supplement — a new member of the "Lucor metallicum" family. Arhiv za Higijenu Rada i Toksikologiju (Archives of Industrial Hygiene and Toxicology);50(3):289-297. — PubMed
- Koval'skiy GA, Yarovaya GA, Shmavonyan DM (1961). Changes in purine metabolism in man and animals under conditions of molybdenum biogeochemical provinces (Armenian endemic gout). Zhurnal Obshchei Biologii. — PubMed
PubMed Topic Searches
- PubMed — Molybdenum toxicity in humans
- PubMed — Molybdenum–copper antagonism and tetrathiomolybdate
- PubMed — Molybdenum, uric acid, and xanthine oxidase
- PubMed — Molybdenum dietary reference and upper intake level
- PubMed — Molybdenum absorption, excretion, and homeostasis
Connections
- Molybdenum Overview
- Molybdenum Deficiency Hub
- Molybdenum Benefits Hub
- Molybdenum and Sulfite Metabolism
- Molybdenum and Uric Acid
- Copper
- Copper Toxicity
- Gout
- Liver Disease (Wilson's Disease)
- Sulfites
- Uric Acid Test
- Kidney Function Tests
- Comprehensive Metabolic Panel
- Sulfur