Zinc Test (Serum Zinc)
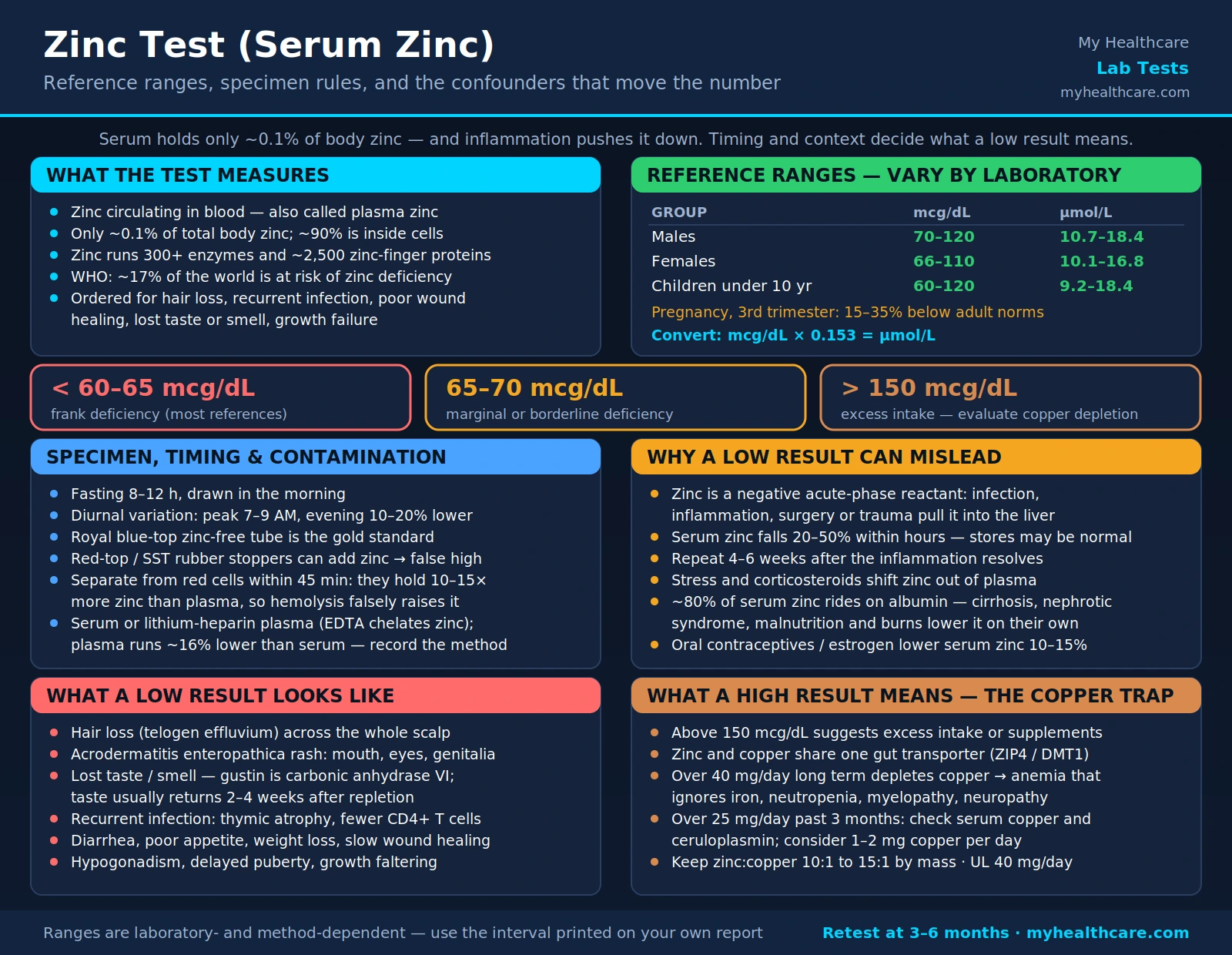
Table of Contents
- Why Test Serum Zinc
- Reference Ranges
- Specimen Requirements
- Limitations and Confounders
- Zinc as Enzymatic Cofactor
- Zinc in Immune Function and Wound Healing
- Taste and Smell (Ageusia and Anosmia)
- Signs of Deficiency
- Supplementation Guidelines
- Who Should Be Tested
- Research Papers and References
- Connections
- Featured Videos
Why Test Serum Zinc
Zinc is the second most abundant trace mineral in the human body after iron, participating in over 300 enzymatic reactions and playing an indispensable role in immune defense, cell division, protein synthesis, DNA replication, and wound repair. Despite its biological importance, zinc deficiency is surprisingly common worldwide — the World Health Organization estimates that approximately 17% of the global population is at risk, with higher rates in populations consuming predominantly plant-based diets or living in food-insecure environments.
The serum zinc test (also called plasma zinc or blood zinc) measures the concentration of zinc circulating in the blood. It is the most widely available clinical tool for assessing zinc status, even though it represents only about 0.1% of total body zinc and can fail to detect early or marginal deficiency. Clinicians order the test when a patient presents with unexplained hair loss, recurrent infections, poor wound healing, diminished taste or smell, growth failure in children, or skin disorders consistent with zinc-responsive dermatoses.
Because zinc participates in so many physiological systems, its deficiency can masquerade as multiple seemingly unrelated problems. A serum zinc test is a low-cost first step that can redirect a diagnostic workup that might otherwise generate far more expensive investigations.
Reference Ranges
Reference ranges for serum zinc vary slightly by laboratory and measurement method, but the widely cited consensus values are:
- Males: 70–120 mcg/dL (10.7–18.4 μmol/L)
- Females: 66–110 mcg/dL (10.1–16.8 μmol/L)
- Children (under 10 years): 60–120 mcg/dL (9.2–18.4 μmol/L)
- Pregnant women (third trimester): Values typically fall 15–35% below non-pregnant adult norms; results must be interpreted with gestational age in mind.
Values below 60–65 mcg/dL are considered frank deficiency by most references. Values between 65–70 mcg/dL may represent marginal or borderline deficiency, particularly when combined with clinical symptoms. Values above 150 mcg/dL suggest excess intake or supplementation and may prompt evaluation for copper depletion.
Units vary between laboratories — some report in mcg/dL (micrograms per deciliter), others in μmol/L (micromoles per liter). To convert mcg/dL to μmol/L, multiply by 0.153. Always confirm the reference interval provided by the reporting laboratory, as instrument calibration and sample matrix (serum vs. plasma) affect absolute values.
Specimen Requirements
Proper specimen collection is critical for serum zinc accuracy, because zinc is ubiquitous in laboratory environments and even minor contamination elevates results.
Fasting morning draw: The test should be drawn after an 8–12 hour fast, ideally in the morning. Zinc concentrations exhibit a well-documented diurnal variation — levels are highest in the morning (roughly 7–9 AM) and decline throughout the day, with a nadir in the afternoon and evening that can be 10–20% lower than the morning peak. This circadian fluctuation is thought to reflect changes in albumin binding and redistribution to tissues following meals and physical activity. Drawing at a consistent morning time allows valid comparison between serial measurements.
Meal timing: Eating a zinc-containing meal shortly before the draw can transiently elevate serum zinc. Conversely, a high-carbohydrate meal may temporarily lower zinc by stimulating insulin-mediated uptake into cells. Standardized fasting eliminates both sources of variability.
Tube selection and handling: Zinc-free (royal blue-top) tubes are the gold standard for trace metal testing. Standard red-top and SST (gel-separator) tubes may contain zinc in the rubber stopper, introducing contamination. The sample must be processed promptly and separated from red blood cells within 45 minutes; erythrocytes contain 10–15 times more zinc than plasma, so hemolysis causes falsely elevated results.
Sample type — serum vs. plasma: Most laboratories accept either serum or lithium-heparin plasma for zinc measurement; EDTA plasma should be avoided because EDTA chelates zinc. Plasma zinc concentrations are approximately 16% lower than serum zinc drawn at the same time, so the collection method must be documented.
Limitations and Confounders
Serum zinc has several important limitations that clinicians and patients must understand before interpreting a result.
Zinc is a negative acute-phase reactant. During infection, inflammation, surgery, or trauma, the liver up-regulates production of metallothionein (a zinc-binding protein) and increases zinc uptake from the blood into hepatocytes as part of the acute-phase response. This redistribution can depress serum zinc by 20–50% within hours of the inflammatory stimulus — even when total body zinc stores are normal or high. A low serum zinc result obtained during or shortly after an acute illness should be repeated 4–6 weeks later once inflammation has resolved. Interpreting a depressed zinc level in an acutely ill patient as dietary deficiency is a common clinical error.
Stress and corticosteroids. Physiological stress (physical or psychological) elevates cortisol, which promotes zinc redistribution away from plasma. Pharmacological corticosteroids (prednisone, hydrocortisone) have a similar effect. Patients on chronic corticosteroid therapy may show borderline-low serum zinc that partly reflects drug effect rather than true deficiency.
Albumin dependency. Approximately 80% of serum zinc is loosely bound to albumin. In conditions that lower albumin — liver cirrhosis, nephrotic syndrome, protein-energy malnutrition, severe burns — serum zinc falls proportionally even when cellular zinc stores are adequate. A corrected zinc calculation (analogous to the corrected calcium formula) has been proposed but is not yet standardized.
Oral contraceptives and estrogen therapy consistently lower serum zinc by 10–15%, possibly by increasing albumin synthesis and altering hepatic zinc metabolism. Results in women taking these medications should be interpreted with that context.
Zinc does not reflect intracellular stores. Because 90% of body zinc resides inside cells (primarily muscle, bone, liver, and prostate), serum levels can remain within the reference range until deficiency is quite advanced. Functional markers such as erythrocyte zinc, platelet zinc, hair zinc, or the zinc taste test may detect marginal deficiency earlier, though none has displaced serum zinc as the primary clinical tool.
Zinc as Enzymatic Cofactor
Zinc is unique among trace minerals in the breadth of enzymatic reactions it supports — over 300 enzymes across all six major enzyme classes (oxidoreductases, transferases, hydrolases, lyases, isomerases, and ligases) require zinc as a structural or catalytic cofactor. This breadth explains why zinc deficiency produces such a diverse array of clinical manifestations.
Carbonic anhydrase — one of the fastest enzymes in the human body — catalyzes the interconversion of carbon dioxide and bicarbonate (CO₂ + H₂O ⇄ H₂CO₃¯ + H⁺), a reaction central to acid-base balance, gas exchange in red blood cells, and gastric acid secretion. All isoforms of carbonic anhydrase are zinc metalloenzymes.
Alkaline phosphatase (ALP) is a zinc and magnesium metalloenzyme. Zinc deficiency reliably lowers ALP activity, and a low ALP on a routine metabolic panel can serve as an indirect clue to zinc depletion — particularly relevant because ALP is routinely measured while serum zinc often is not.
Superoxide dismutase (Cu/Zn-SOD, or SOD1) is the primary cytoplasmic antioxidant enzyme, neutralizing the superoxide radical (O₂¯) generated by mitochondrial electron leakage and immune activation. Each SOD1 molecule contains one zinc atom (structural) and one copper atom (catalytic). Zinc deficiency therefore impairs both direct antioxidant activity and, indirectly, copper-dependent catalysis.
RNA and DNA polymerases contain zinc-finger domains — compact protein structures in which a zinc ion coordinates four cysteine or histidine residues to stabilize a loop that contacts nucleic acids. The human genome encodes approximately 2,500 zinc-finger proteins; they include transcription factors, DNA-repair enzymes, and chromosome-organizing proteins. This is why zinc deficiency preferentially affects rapidly dividing tissues (gut epithelium, immune cells, skin, hair follicles, gonads) — these cells need continuous transcription and replication.
Metallothionein is both a zinc-storage protein and a free-radical scavenger. It sequesters up to seven zinc atoms per molecule, releasing them in response to cellular zinc demand. During acute inflammation, cytokines (primarily IL-6) massively up-regulate hepatic metallothionein, pulling zinc out of the plasma — the mechanism behind the acute-phase reactant effect described above.
Zinc in Immune Function and Wound Healing
Zinc is essential for the development, maturation, and function of virtually every cell type in the immune system. Its absence creates a state of acquired immunodeficiency that particularly affects cell-mediated immunity.
Thymulin is a thymic hormone required for the differentiation and activation of T lymphocytes; it is a zinc-dependent nonapeptide that is biologically inactive without a bound zinc atom. Zinc deficiency causes thymic atrophy, reduced thymulin activity, and a selective decrease in CD4+ helper T cells — a pattern that clinically resembles mild HIV-induced immunosuppression in its susceptibility to opportunistic and recurrent infections.
Natural killer (NK) cell activity, neutrophil phagocytosis, and macrophage oxidative burst are all impaired in zinc-deficient individuals. This explains the well-established clinical observation that zinc-deficient children in low-income countries suffer dramatically higher rates of pneumonia, diarrheal disease, and malaria.
Zinc and wound healing proceed through several overlapping mechanisms: zinc stimulates fibroblast proliferation and collagen synthesis; it activates matrix metalloproteinases needed for tissue remodeling; it stabilizes cell membranes against oxidative damage; and it supports the proliferative phase of keratinocyte migration across the wound surface. Chronic non-healing wounds — particularly leg ulcers and pressure injuries — are a recognized manifestation of zinc deficiency, and supplementation accelerates healing in deficient patients, though it does not speed healing in zinc-replete individuals.
Zinc and the innate immune response to viruses: Intracellular zinc has direct antiviral properties. Zinc inhibits the RNA-dependent RNA polymerase of several respiratory viruses, slowing their replication within host cells. Zinc ionophores (compounds that carry zinc into cells) such as quercetin and epigallocatechin gallate (EGCG) have attracted research interest as adjuncts to zinc supplementation for respiratory infections.
Taste and Smell (Ageusia and Anosmia)
Zinc deficiency is one of the most common nutritional causes of impaired taste (ageusia or hypogeusia) and impaired smell (anosmia or hyposmia). The connection became widely recognized during the COVID-19 pandemic, when a substantial proportion of patients developed sudden, profound loss of taste and smell — prompting researchers to investigate whether subclinical zinc depletion might amplify SARS-CoV-2-related sensory loss.
Mechanism — gustin (carbonic anhydrase VI): Taste and smell function depend critically on a zinc metalloprotein called gustin, identified as carbonic anhydrase VI (CA-VI). Gustin is secreted by parotid salivary glands and supports the growth, maintenance, and renewal of taste bud cells. Zinc deficiency reduces gustin activity and impairs taste bud turnover; affected individuals report that foods taste bland, metallic, or uniformly sweet. Replenishing zinc typically restores taste within 2–4 weeks in deficiency-related cases.
Olfactory epithelium turnover: The olfactory epithelium, like the gut lining and skin, is a rapidly renewing tissue. Zinc deficiency slows the proliferation and differentiation of olfactory receptor neurons, leading to gradual attrition of smell function. Unlike viral anosmia (which can involve neuroepithelial destruction), zinc-deficiency anosmia tends to be gradual and is usually reversible.
COVID-19 connection: Several studies found that COVID-19 patients with anosmia had lower serum zinc levels on admission than those without olfactory symptoms, and that zinc supplementation shortened the duration of anosmia in some trials. The prevailing hypothesis is that SARS-CoV-2 infection triggers an acute-phase zinc redistribution (see Limitations section) that may deprive the already-inflamed olfactory neuroepithelium of the zinc it needs for repair and regeneration. Whether zinc supplementation provides measurable benefit in COVID-associated anosmia remains an active area of research.
Signs of Deficiency
Zinc deficiency manifests across multiple organ systems because of the mineral's role in so many enzymatic pathways. Clinical presentation ranges from subtle (marginal deficiency with non-specific fatigue and recurrent colds) to severe (profound immune failure and characteristic skin rash).
Skin and hair:
- Hair loss (telogen effluvium): Zinc is required for hair follicle cycling. Deficiency accelerates the transition from anagen (growth) to telogen (resting) phase, producing diffuse scalp hair thinning. The pattern differs from androgenetic alopecia in that it affects the entire scalp rather than crown or frontal regions, and it reverses with supplementation.
- Acrodermatitis enteropathica: The most dramatic manifestation of severe zinc deficiency, this condition produces a characteristic vesiculobullous and erythematous rash around the mouth, eyes, genitalia, and extremities — the body's highest-turnover skin sites. It occurs in its inherited form due to a mutation in the ZIP4 zinc transporter gene, and in its acquired form in patients on long-term total parenteral nutrition without adequate zinc supplementation, or in exclusively breastfed infants of mothers with low milk zinc.
- Paronychia and nail changes: White transverse bands (Beau's lines) across the nails and periungual inflammation are recognized features of zinc depletion.
Gastrointestinal:
- Diarrhea: Zinc is essential for intestinal epithelial integrity and brush-border enzyme activity. Deficiency causes villous atrophy and increased gut permeability, producing osmotic and secretory diarrhea. This creates a vicious cycle — diarrhea further depletes zinc through fecal losses, worsening the deficiency. Zinc supplementation in children with acute diarrhea shortens episode duration and reduces the risk of subsequent episodes, which is the basis for WHO and UNICEF recommendations for 10–14 days of zinc during pediatric diarrheal illness.
- Poor appetite and weight loss: Zinc-deficient individuals commonly lose their appetite, possibly through effects on leptin, ghrelin, and zinc's role in taste perception.
Reproductive and developmental:
- Hypogonadism: Zinc is required for testosterone synthesis and spermatogenesis. Male zinc deficiency produces low testosterone, reduced sperm count, and impaired sperm motility. The association between zinc and male fertility is well-established, and the testes and prostate gland have among the highest zinc concentrations of any tissue.
- Delayed puberty: Classic studies by Ananda Prasad in the 1960s in rural Egypt and Iran identified zinc deficiency as a cause of hypogonadal dwarfism — adolescent males with markedly delayed sexual development and short stature who responded dramatically to zinc supplementation. This discovery established zinc as an essential human nutrient.
- Growth retardation: Zinc deficiency is a significant contributor to childhood stunting globally. Zinc is necessary for growth hormone signaling and insulin-like growth factor 1 (IGF-1) production.
Neurological:
- Cognitive impairment: The hippocampus contains some of the highest brain zinc concentrations; mossy fiber synapses release zinc as a co-transmitter with glutamate. Zinc modulates NMDA receptor activity and is thought to play a role in learning and memory consolidation.
- Poor wound healing: Manifests as chronically non-healing skin ulcers, poor surgical healing, and increased infection risk post-operatively.
Supplementation Guidelines
When serum zinc confirms deficiency — or when clinical signs are strongly suggestive and a clinical trial is appropriate — zinc supplementation is straightforward and generally well-tolerated at therapeutic doses.
Typical therapeutic doses:
- Mild-to-moderate deficiency: 15–30 mg elemental zinc per day for 3–6 months, then retest.
- Severe deficiency or acrodermatitis enteropathica: 1–3 mg/kg/day elemental zinc under medical supervision.
- Maintenance / prevention: The Recommended Dietary Allowance (RDA) is 11 mg/day for adult males and 8 mg/day for adult females (12 mg/day during pregnancy, 13 mg/day during lactation).
- Tolerable Upper Intake Level (UL): 40 mg/day for adults from all sources combined.
Preferred forms: Not all zinc supplements are equally bioavailable.
- Zinc glycinate (zinc bound to the amino acid glycine): highly bioavailable, gentle on the stomach, typically 20–30% elemental zinc by weight.
- Zinc citrate: well-absorbed, less likely to cause nausea than zinc sulfate, approximately 31% elemental zinc.
- Zinc picolinate: often marketed as the most bioavailable form; evidence is mixed but generally favorable.
- Zinc sulfate: effective and inexpensive but frequently causes gastrointestinal upset (nausea, stomach cramping) when taken on an empty stomach; best taken with food.
- Zinc oxide: the least bioavailable form (~50–60% as bioavailable as zinc sulfate in some studies); commonly used in sunscreen and diaper rash creams but a poor choice for nutritional supplementation.
Critical warning — copper depletion: Zinc and copper compete for absorption via the same intestinal transporter (ZIP4/DMT1). Long-term zinc supplementation at doses above 40 mg/day can deplete copper, causing a reversible anemia (microcytic or normocytic) that does not respond to iron, along with neutropenia and neurological symptoms (myelopathy, peripheral neuropathy). Anyone supplementing zinc at doses above 25 mg/day for more than 3 months should have serum copper and ceruloplasmin tested periodically and consider co-supplementing with 1–2 mg copper per day. The standard recommendation is a 10:1 to 15:1 zinc-to-copper ratio by mass for chronic supplementation.
Timing and interactions: Zinc absorption is inhibited by phytates (in whole grains and legumes), calcium supplements, iron supplements, and quinolone or tetracycline antibiotics. Take zinc supplements at least 2 hours apart from these substances. Taking zinc with a small amount of protein (rather than on an empty stomach or with a high-phytate meal) optimizes absorption.
Who Should Be Tested
Routine serum zinc screening is not recommended for the general population. Testing is most appropriate in individuals with a higher pre-test probability of deficiency or excess:
At risk for deficiency:
- Strict vegetarians and vegans (phytates reduce zinc bioavailability from plant sources by 15–35%)
- Patients with inflammatory bowel disease (Crohn's disease, ulcerative colitis), short bowel syndrome, or other malabsorptive conditions
- Patients on long-term total parenteral nutrition
- Alcoholics (alcohol increases urinary zinc excretion)
- Individuals with sickle cell disease (increased zinc losses through urinary excretion)
- Pregnant and breastfeeding women, particularly those with poor dietary zinc intake
- Exclusively breastfed infants beyond 6 months (breast milk zinc declines sharply after 6 months)
- Children with growth faltering or recurrent infections in low-income settings
- Patients with chronic kidney disease (increased urinary losses)
- Older adults with poor dietary intake or reduced stomach acid (achlorhydria impairs zinc absorption)
- Patients with unexplained hypogeusia, anosmia, or chronic non-healing wounds
- Post-bariatric surgery patients (gastric bypass significantly reduces zinc absorption)
At risk for excess or toxicity:
- Patients using high-dose zinc supplements (>40 mg/day) for extended periods
- Workers with occupational zinc exposure (welding, galvanizing, metal smelting)
- Patients with unexplained microcytic anemia or neutropenia unresponsive to iron treatment (possible zinc-induced copper deficiency)
After treatment or supplementation, follow-up serum zinc should be measured at 3–6 months to confirm response and avoid over-correction. In patients where serum zinc is expected to be confounded by inflammation, measuring erythrocyte zinc or serum alkaline phosphatase trend can provide supplementary evidence of true zinc status.
Research Papers and References
The following are curated PubMed literature searches for key topics covered on this page. Each link opens a live PubMed search for current evidence.
- Serum zinc deficiency diagnosis and clinical assessment — PubMed
- Serum zinc reference ranges in healthy adults — PubMed
- Zinc and immune function — T lymphocytes and thymulin — PubMed
- Zinc in wound healing — collagen and fibroblast proliferation — PubMed
- Zinc supplementation and copper depletion — PubMed
- Zinc deficiency and taste impairment — ageusia hypogeusia — PubMed
- Acrodermatitis enteropathica and zinc deficiency — PubMed
- Zinc as metalloenzyme and enzymatic cofactor — PubMed
- Serum zinc diurnal variation and circadian pattern — PubMed
- Zinc as negative acute-phase reactant in infection and inflammation — PubMed
- Zinc and anosmia in COVID-19 — olfactory loss — PubMed
- Zinc supplement forms and bioavailability — glycinate citrate oxide — PubMed
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Zinc (Mineral) — full nutrient profile, functions, and food sources
- Copper — competes with zinc for intestinal absorption; monitor during high-dose zinc supplementation
- Iron Panel — iron and zinc both rely on trace-metal transport mechanisms; concurrent deficiencies are common
- Complete Blood Count — anemia and neutropenia may signal zinc-induced copper depletion
- Immunology — zinc is foundational to T-cell, NK-cell, and innate immune function
- Vitamin A — zinc is required for retinol-binding protein synthesis and transport of vitamin A from the liver
- Dermatology — acrodermatitis enteropathica, eczema, and chronic wounds linked to zinc status
- Hair Loss — telogen effluvium associated with zinc deficiency; serum zinc is a first-line test in hair loss workup