Copper Test (Serum Copper and Ceruloplasmin)
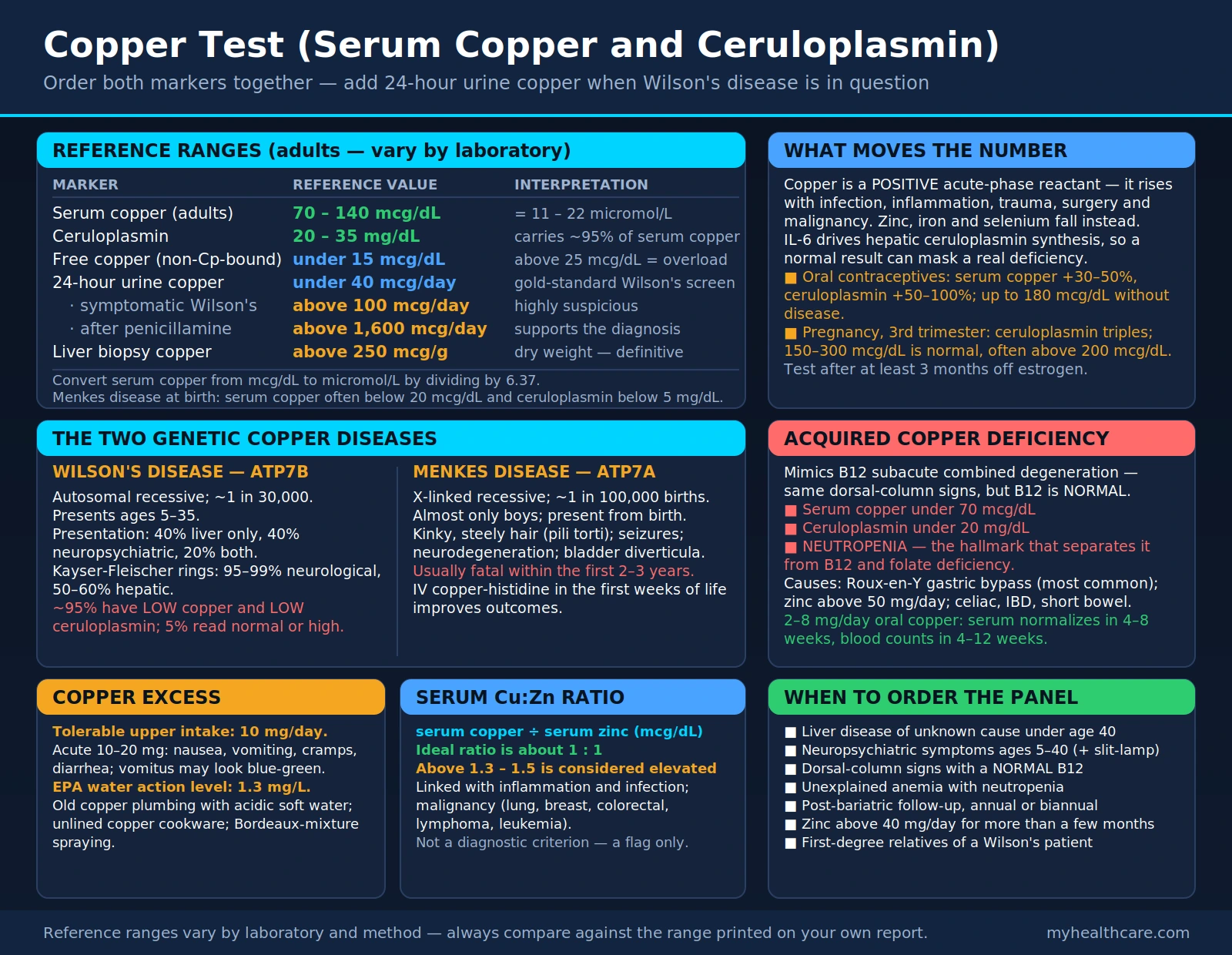
Table of Contents
- Why Test Serum Copper and Ceruloplasmin Together
- Reference Ranges
- Copper as a Positive Acute-Phase Reactant
- Wilson's Disease — ATP7B Mutation
- Menkes Disease — ATP7A Mutation
- Copper Deficiency: Myelopathy and Cytopenias
- Excess Copper: Sources and Toxicity
- Copper-Zinc Balance and Clinical Interpretation
- When to Order the Copper Panel
- Research Papers and References
- Connections
- Featured Videos
Why Test Serum Copper and Ceruloplasmin Together
Serum copper and ceruloplasmin are almost always ordered together, and for good reason: interpreting either result in isolation leads to mistakes. Ceruloplasmin is the main copper-transport protein in the blood, carrying approximately 95% of total serum copper. The remaining 5% circulates loosely bound to albumin or as free ionic copper.
When ceruloplasmin is low — as it is in Wilson's disease or severe malnutrition — most of the copper in the blood is that dangerous free fraction, not the safely bound form. A patient with Wilson's disease may show a low total serum copper precisely because they are making almost no ceruloplasmin, even though toxic copper is accumulating in their liver and brain. Conversely, in pregnancy or with oral contraceptive use, estrogen drives ceruloplasmin production sharply upward, pushing total serum copper above 200 mcg/dL in a completely healthy woman.
Together, the two tests allow you to calculate free (non-ceruloplasmin-bound) copper: multiply ceruloplasmin (mg/dL) by 3.15 to estimate the copper it carries (mcg/dL), then subtract from total serum copper. A free copper above 25 mcg/dL suggests Wilson's disease even when the total serum copper looks misleadingly low or normal.
Ordering only serum copper is a common and costly mistake. Clinicians who see a "normal" serum copper may falsely reassure a patient who actually has Wilson's disease, while those who see elevated copper may miss an entirely physiological estrogen effect. Always order both markers together.
Reference Ranges
Reference ranges vary slightly by laboratory and method, but the following values represent widely accepted adult norms:
- Serum copper (adults): 70–140 mcg/dL (11–22 micromol/L)
- Ceruloplasmin: 20–35 mg/dL
- Free (non-ceruloplasmin-bound) copper: normally <15 mcg/dL; values above 25 mcg/dL suggest copper overload
- Serum copper in pregnancy (third trimester): 150–300 mcg/dL is considered normal due to estrogen-driven ceruloplasmin surge
- Serum copper in women on oral contraceptives: up to 180 mcg/dL may be seen without disease
- 24-hour urine copper (gold standard for Wilson's disease screening): normal <40 mcg/day; symptomatic Wilson's >100 mcg/day; post-penicillamine challenge >1,600 mcg/day supports diagnosis
Children have naturally higher ceruloplasmin than adults, and neonates may have very low levels that normalize by 6 months of age. Menkes disease presents at birth with low serum copper and ceruloplasmin, often below 20 mcg/dL and below 5 mg/dL respectively.
Units differ between US labs (mcg/dL) and international labs (micromol/L). To convert serum copper from mcg/dL to micromol/L, divide by 6.37. Always check your lab's reference range on the report itself, as methods differ.
Copper as a Positive Acute-Phase Reactant
Unlike most minerals, copper behaves as a positive acute-phase reactant — meaning its serum level rises during infection, inflammation, trauma, surgery, and malignancy. This is the opposite of zinc, iron, and selenium, all of which fall during the acute-phase response as part of a protective nutritional immune strategy.
The mechanism is straightforward: interleukin-6 (IL-6) and other inflammatory cytokines stimulate hepatic synthesis of ceruloplasmin, which is itself an acute-phase protein. Because ceruloplasmin carries 95% of serum copper, total serum copper rises proportionally. Copper also functions as a cofactor for several immune enzymes, including copper-zinc superoxide dismutase and cytochrome c oxidase.
Clinical traps created by this effect:
- A patient with Wilson's disease who also has active liver inflammation may temporarily have normal or elevated serum copper and ceruloplasmin, masking the underlying deficiency. This is part of the "neurological Wilson's paradox" described below.
- A patient with true copper deficiency who has concurrent infection may show a falsely normal copper level, delaying diagnosis.
- Patients with active cancers (especially lung, breast, lymphoma, and leukemia) routinely show elevated serum copper and ceruloplasmin as a marker of systemic inflammation and tumor burden — not excess dietary copper.
Estrogen is the single most powerful driver of ceruloplasmin production. Combined oral contraceptive pills containing estrogen can raise serum copper by 30–50%, and ceruloplasmin by 50–100%. Pregnancy escalates this further: by the third trimester, ceruloplasmin triples compared to pre-pregnancy values, and total serum copper commonly exceeds 200 mcg/dL. This is physiological and does not require treatment. Testing for copper status in pregnant women or women on hormonal contraception requires awareness of this confound, and ideally deferred until off estrogen for at least 3 months.
Wilson's Disease — ATP7B Mutation
Wilson's disease is an autosomal recessive inherited disorder of copper metabolism caused by mutations in the ATP7B gene, which encodes a copper-transporting ATPase in liver cells. The protein's job is to export copper into bile for excretion. When ATP7B is defective, copper cannot leave the hepatocyte and accumulates first in the liver, then spills into the bloodstream and deposits in the brain (especially the basal ganglia), kidneys, and corneas.
Wilson's disease affects approximately 1 in 30,000 people worldwide, and it is one of the few genetic diseases that is both treatable and fatal if missed. It typically presents between ages 5 and 35, though late presentations into the 60s are reported. About 40% of patients present with liver disease alone, 40% with neuropsychiatric symptoms, and 20% with both.
Classic Signs
- Kayser-Fleischer rings: golden-brown rings at the outer rim of the cornea (limbus), visible only on slit-lamp exam by an ophthalmologist; present in 95–99% of neurological Wilson's but only 50–60% of hepatic presentations
- Basal ganglia copper deposition: causes dysarthria, dysphagia, tremor, dystonia, rigidity, and Parkinsonian features
- Neuropsychiatric symptoms: personality change, depression, psychosis, cognitive decline; often misdiagnosed as primary psychiatric illness for years
- Liver disease: ranges from asymptomatic transaminitis to cirrhosis; acute liver failure with Coombs-negative hemolytic anemia is a Wilson's emergency
- Fanconi syndrome: proximal renal tubular dysfunction causing aminoaciduria, phosphaturia, and renal tubular acidosis
The Wilson's Disease Diagnosis Trap
The most dangerous misconception in Wilson's disease testing is the belief that a low serum copper always means Wilson's. Approximately 95% of Wilson's patients have low serum copper and low ceruloplasmin, which is the expected pattern. But 5% of Wilson's patients — particularly those with neurological presentations — have normal or even elevated serum copper. This "neurological Wilson's paradox" occurs because:
- The liver releases copper in abnormal non-ceruloplasmin-bound form, which raises total serum copper but not ceruloplasmin-bound copper.
- Concurrent liver inflammation elevates ceruloplasmin as an acute-phase reactant, pushing serum copper into the normal range.
- Early-stage disease may not yet have depleted hepatic copper stores enough to reduce serum levels.
For this reason, the gold standard for Wilson's disease diagnosis is 24-hour urine copper, which reflects actual copper excretion independent of ceruloplasmin. A value above 100 mcg/day in a symptomatic patient is highly suspicious; above 1,600 mcg/day after a D-penicillamine challenge confirms the diagnosis. Liver biopsy showing hepatic copper above 250 mcg/g dry weight is definitive.
Diagnosis and Treatment
- Genetic testing for ATP7B mutations can confirm the diagnosis in ambiguous cases and is essential for family screening.
- D-penicillamine (copper chelator): first-line treatment for decades; removes copper via urinary excretion; requires pyridoxine supplementation; side effects include nephrotoxicity, bone marrow suppression, and worsening of neurological symptoms in up to 20% of patients at treatment initiation (a paradoxical neurological deterioration from mobilization of copper).
- Trientine (triethylenetetramine): alternative chelator with better neurological tolerability; now often preferred for neurological presentation.
- Zinc acetate or sulfate: blocks intestinal copper absorption by inducing metallothionein in enterocytes; used for maintenance therapy and in asymptomatic patients; safe in pregnancy.
- Liver transplantation: corrects the metabolic defect; indicated for acute liver failure or decompensated cirrhosis unresponsive to chelation.
Menkes Disease — ATP7A Mutation
Menkes disease (also called Menkes kinky hair syndrome or steely hair syndrome) is caused by mutations in the ATP7A gene, located on the X chromosome. It is therefore X-linked recessive, affecting almost exclusively boys, with an incidence of approximately 1 in 100,000 live births.
ATP7A performs the same copper-transport function as ATP7B but in the intestine and blood-brain barrier rather than the liver. When ATP7A is defective, copper accumulates in intestinal cells and cannot be exported into the circulation. The result is profound systemic copper deficiency despite copper being present in the diet — the body cannot absorb and distribute it properly.
Clinical Features
- Kinky, steely, or sparse hair (pili torti): the most recognizable sign; hair breaks easily and appears twisted under microscopy due to defective copper-dependent cross-linking enzymes
- Severe neurodegeneration: seizures, progressive loss of developmental milestones, profound intellectual disability; cerebellar and cerebral atrophy on MRI
- Connective tissue abnormalities: due to deficient lysyl oxidase (a copper enzyme essential for collagen and elastin cross-linking); bladder diverticula, vascular tortuosity, skeletal fractures, lax joints
- Hypothermia, hypotonia, feeding failure
- Low serum copper and ceruloplasmin: often below 20 mcg/dL and 5 mg/dL respectively from birth
Without treatment, Menkes disease is usually fatal within the first 2–3 years of life. Early diagnosis before the onset of neurological symptoms is critical. Newborn screening via plasma catecholamine ratios (specifically elevated dopamine relative to norepinephrine, reflecting impaired dopamine-beta-hydroxylase which requires copper) shows promise for earlier detection.
Treatment with intravenous copper-histidine, started in the first weeks of life before neurological symptoms begin, can partially restore copper delivery to the brain through an ATP7A-independent route and dramatically improves outcomes in patients with partially functional ATP7A mutations. In classical severe Menkes, even early treatment provides limited benefit. Genetic confirmation via ATP7A sequencing is essential for family counseling, including identification of female carriers who may show subtle hair or skin findings.
Copper Deficiency: Myelopathy and Cytopenias
Acquired copper deficiency in adults is far more common than most clinicians recognize, and it is frequently missed because providers rarely think to test for it. The classic presentation is a subacute combined degeneration of the spinal cord that mimics vitamin B12 deficiency almost exactly — the same dorsal column and corticospinal tract demyelination, the same gait ataxia and sensory loss, the same hyperreflexia progressing to weakness.
The key difference: B12 levels are normal. Many patients undergo extensive neurological workup, receive empirical B12 injections without response, and only have copper checked after months of decline. Once copper is replaced, neurological improvement occurs in most but recovery is incomplete if deficiency was prolonged.
Causes of Acquired Copper Deficiency
- Bariatric surgery (especially Roux-en-Y gastric bypass): the most common cause in developed countries; copper is primarily absorbed in the stomach and proximal duodenum, which are bypassed; serum copper should be checked annually post-bypass
- Excessive zinc supplementation: zinc induces intestinal metallothionein, which preferentially binds copper and prevents its absorption; this is why Wilson's disease is treated with zinc; doses of zinc above 50 mg/day chronically can cause copper deficiency; high-dose zinc lozenges (used for colds) and denture adhesive creams containing zinc (used in excess) have caused severe copper deficiency myelopathy
- Malabsorption syndromes: celiac disease, inflammatory bowel disease, short bowel syndrome, prolonged total parenteral nutrition without adequate copper supplementation
- Gastrectomy or gastric achlorhydria: reduced stomach acid impairs copper solubilization
Laboratory Findings
- Low serum copper (<70 mcg/dL)
- Low ceruloplasmin (<20 mg/dL)
- Anemia: typically normocytic or microcytic, resembling iron deficiency; may show vacuolated erythroid precursors on bone marrow biopsy
- Neutropenia: a hallmark finding that distinguishes copper deficiency from B12/folate deficiency; may predispose to infections
- Normal B12, folate, and iron studies
Treatment
Oral copper gluconate or copper sulfate at 2–8 mg/day for several months typically normalizes serum levels within 4–8 weeks. The hematological abnormalities (anemia and neutropenia) typically resolve within 4–12 weeks of repletion. Neurological recovery is slower and incomplete, making early diagnosis critical. If oral absorption is impaired (e.g., short bowel), intravenous copper chloride is available. Concurrent zinc supplementation should be stopped or reduced.
Excess Copper: Sources and Toxicity
Copper toxicity from dietary or environmental sources is less common than deficiency in most populations, but it does occur and can be serious. The liver is the primary organ affected by copper overload, because it is responsible for exporting excess copper into bile for elimination. When this capacity is overwhelmed, hepatocellular damage, cirrhosis, and eventually acute liver failure can follow.
Sources of Excess Copper Exposure
- Old copper plumbing: the most common environmental exposure; acidic water (low pH, soft water) leaches copper from pipes and solder joints; infants fed formula reconstituted with such water are particularly vulnerable; levels above 1.3 mg/L in drinking water are an EPA action level
- Copper cookware with acidic foods: unlined copper pots used for tomatoes, citrus, or vinegar-based dishes can dissolve significant copper into food; modern copper cookware is lined with tin or stainless steel specifically to prevent this
- Excessive copper supplementation: the tolerable upper intake level for copper is 10 mg/day for adults; supplements marketed for "immune support" or combined with zinc can exceed safe doses; acute ingestion above 10–20 mg causes nausea, vomiting, abdominal cramps, and diarrhea
- Occupational exposure: vineyard workers exposed to copper sulfate sprays (Bordeaux mixture); smelters and electroplating workers
- Indian childhood cirrhosis: a historically recognized condition in India associated with storage of milk in copper or brass vessels; largely eliminated with modern practices
Symptoms of Copper Toxicity
- Acute: nausea, vomiting (vomitus may appear blue-green), abdominal pain, diarrhea, metallic taste
- Subacute/chronic: hepatitis, jaundice, elevated liver enzymes (ALT, AST), right upper quadrant pain
- Severe: hemolytic anemia (copper directly damages red blood cell membranes), acute kidney injury, liver failure, encephalopathy
High-dose vitamin C (ascorbic acid) can reduce copper absorption from the gut by reducing cupric copper (Cu2+) to the less-well-absorbed cuprous form (Cu+) and competing for uptake pathways. This is one reason very high-dose vitamin C supplementation is occasionally used adjunctively in copper overload conditions, though it is not a substitute for chelation therapy.
Copper-Zinc Balance and Clinical Interpretation
Copper and zinc are metabolic antagonists that compete for absorption in the small intestine via shared metal transporters (especially DMT1 and metallothionein). The serum Cu:Zn ratio has attracted growing clinical and research interest as a marker of systemic inflammation, oxidative stress, and certain disease states.
The ideal Cu:Zn ratio is approximately 1:1. In practice, the ratio is calculated by dividing serum copper (mcg/dL) by serum zinc (mcg/dL). A ratio above 1.3–1.5 is generally considered elevated and has been associated with:
- Systemic inflammation and infection: because copper rises and zinc falls during the acute-phase response, the ratio amplifies the inflammatory signal
- Malignancy: elevated Cu:Zn ratios have been documented in lung cancer, breast cancer, colorectal cancer, lymphoma, and leukemia; the ratio tracks disease burden and falls with successful treatment in some studies
- Cardiovascular disease risk: some studies associate high Cu:Zn with oxidative stress and endothelial dysfunction
- Alzheimer's disease: dyshomeostasis of copper and zinc in the brain is an active area of research, with evidence of elevated brain copper and reduced brain zinc in affected tissue
A high Cu:Zn ratio is common in modern chronic illness for several reasons: diets high in processed foods are often low in zinc; widespread use of proton pump inhibitors impairs zinc absorption; zinc is depleted by chronic stress via the same cortisol pathway that mobilizes copper; and phytate-rich diets without adequate preparation (soaking, fermentation) reduce zinc bioavailability.
Importantly, the Cu:Zn ratio is not an independent diagnostic criterion for any specific disease — it is a flag that warrants further investigation. Correcting it typically involves addressing the underlying cause (treating inflammation, stopping excess zinc or copper supplementation, repleting zinc if deficient) rather than arbitrarily supplementing zinc to bring the ratio down.
Morley Robbins and the Root Cause Protocol framework have emphasized the copper-iron-ceruloplasmin triad as central to chronic illness, arguing that most "copper toxicity" presentations are actually copper dysregulation due to low ceruloplasmin function and inadequate bioavailable copper. This perspective differs from the conventional toxicology view and is discussed further at Copper Iron Dysregulation and Hemoglobin and Ceruloplasmin Relationship.
When to Order the Copper Panel
The copper panel (serum copper + ceruloplasmin, usually with 24-hour urine copper when Wilson's disease is suspected) should be considered in the following clinical situations:
- Young patient with liver disease of unknown cause: Wilson's disease must be excluded in anyone under 40 with unexplained hepatitis, cirrhosis, or acute liver failure — it is one of the few reversible causes
- Neuropsychiatric symptoms in a patient aged 5–40: especially dysarthria, dystonia, tremor, psychiatric change, or cognitive decline without clear diagnosis; request slit-lamp exam for Kayser-Fleischer rings simultaneously
- Subacute combined degeneration with normal B12: any patient with dorsal column findings (gait ataxia, sensory loss) and normal B12 should have copper checked promptly
- Unexplained anemia with neutropenia: particularly post-bariatric surgery or with a history of excessive zinc supplementation
- Post-bariatric surgery follow-up: annual or biannual copper (along with zinc, iron, B12, folate, vitamin D) is standard of care
- Chronic high-dose zinc supplementation: any patient taking >40 mg/day of zinc for more than a few months
- Infant male with kinky hair, hypotonia, and developmental delay: Menkes disease requires urgent copper supplementation; confirm with plasma catecholamines and ATP7A sequencing
- Suspected copper toxicity: liver disease with known exposure to copper pipes, cookware, or excessive supplementation
- Evaluation of inflammatory state: as part of a broader micronutrient panel, the Cu:Zn ratio provides useful context alongside CRP and ferritin
- Family history of Wilson's disease: screen first-degree relatives with serum copper, ceruloplasmin, slit-lamp exam, and 24-hour urine copper
Because estrogen dramatically elevates copper and ceruloplasmin, results from women on oral contraceptives or hormone replacement therapy should be interpreted with caution. Ideally, testing is performed after at least 3 months off estrogen-containing medications. Pregnancy testing in the third trimester is unreliable for detecting either deficiency or Wilson's disease unless 24-hour urine copper and free copper calculations are used.
Research Papers and References
The following are curated PubMed literature searches for the key topics covered in this article. Each link opens a current search of the PubMed database.
- Wilson disease diagnosis — serum copper and ceruloplasmin interpretation (PubMed)
- Ceruloplasmin and copper serum clinical interpretation (PubMed)
- Menkes disease — ATP7A mutation and copper deficiency (PubMed)
- Copper deficiency myelopathy and spinal cord demyelination (PubMed)
- Copper-zinc ratio in inflammation and cancer (PubMed)
- Oral contraceptives, estrogen, copper and ceruloplasmin elevation (PubMed)
- Copper deficiency causing anemia and neutropenia (PubMed)
- Wilson disease neurological presentation and diagnosis (PubMed)
- Copper toxicity and liver disease from drinking water (PubMed)
- Ceruloplasmin as an acute phase reactant in inflammation (PubMed)
- Copper supplementation for deficiency treatment (PubMed)
- Gastric bypass and copper deficiency after bariatric surgery (PubMed)
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Copper (Mineral)
- Zinc (Mineral)
- Iron Panel Lab Test
- Zinc Test
- Liver Disease
- Hemoglobin and Ceruloplasmin Relationship
- Copper Iron Dysregulation (Morley Robbins)
- Anemia
- Wilson's Disease — the ATP7B copper-transport disorder this panel is most often ordered to rule in or out.