Aldosterone-Renin Ratio (ARR)
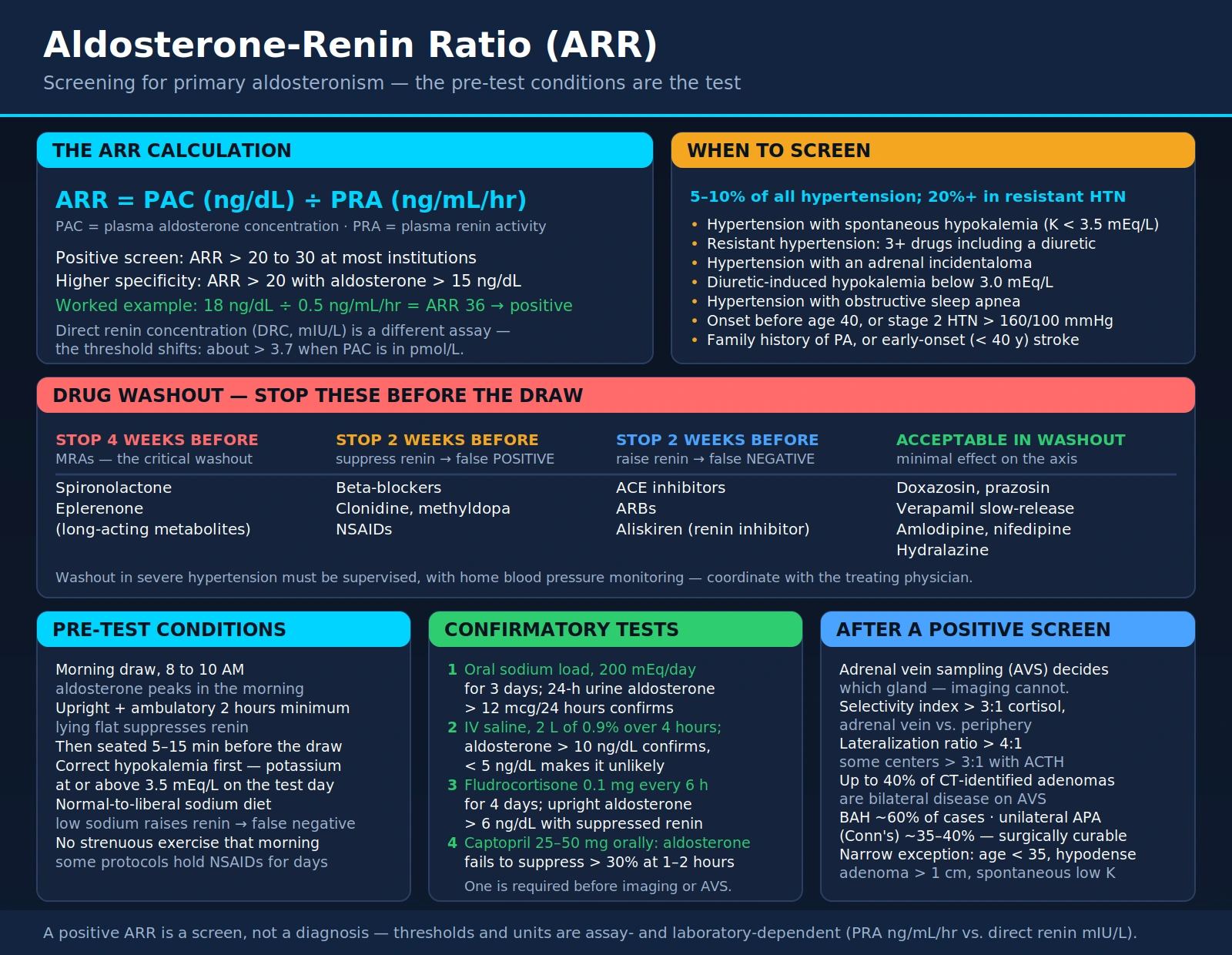
Table of Contents
- Primary Aldosteronism: The Hidden Cause of Hypertension
- The ARR Calculation
- Specimen Requirements — Timing and Position Matter
- Drug Interference: What to Stop and When
- Confirmatory Tests
- Adrenal Vein Sampling: Lateralization
- Treatment: Surgery vs. Medical Management
- When to Screen for Primary Aldosteronism
- Research Papers and References
- Connections
- Featured Videos
Primary Aldosteronism: The Hidden Cause of Hypertension
Primary aldosteronism is the most common cause of secondary hypertension, yet the vast majority of affected patients are never diagnosed. Research consistently shows it affects 5–10% of all hypertension patients — a staggering figure given that tens of millions of Americans carry a hypertension diagnosis. In resistant hypertension (blood pressure uncontrolled on three or more drugs), prevalence rises to 20% or higher.
The root problem is autonomous aldosterone production from one or both adrenal glands, operating independently of the normal renin-angiotensin system. Normally, aldosterone rises when renin signals that blood pressure or sodium is low. In primary aldosteronism, aldosterone is produced continuously regardless of what renin tells it to do — a regulatory circuit that has gone rogue.
Two main structural subtypes drive the condition:
- Bilateral adrenal hyperplasia (BAH): Both adrenal glands are overactive. Accounts for roughly 60% of cases. Managed medically rather than surgically.
- Unilateral aldosterone-producing adenoma (APA): A benign tumor in one adrenal gland, classically called Conn's syndrome. Accounts for roughly 35–40% of cases. Surgically curable.
The consequences extend far beyond blood pressure. Excess aldosterone causes hypokalemia (low potassium), hypomagnesemia (low magnesium), and direct cardiovascular damage. Studies show that patients with primary aldosteronism have significantly higher rates of atrial fibrillation, stroke, heart failure, and kidney damage than patients with essential hypertension at the same blood pressure level. Aldosterone itself appears to be directly toxic to the heart and blood vessels through pro-fibrotic and pro-inflammatory pathways — independent of its blood pressure effects entirely.
The aldosterone-renin ratio (ARR) is the first-line screening test that unmasks this diagnosis. A high aldosterone with a suppressed renin produces a markedly elevated ratio — the biochemical fingerprint of autonomous aldosterone secretion.
The ARR Calculation
The ARR is a simple division: plasma aldosterone concentration (PAC) divided by plasma renin activity (PRA). Understanding the units is critical, because laboratories are not all standardized.
The most common form uses:
- Aldosterone in ng/dL
- Plasma renin activity (PRA) in ng/mL/hr
- ARR = PAC (ng/dL) ÷ PRA (ng/mL/hr)
A threshold of >20 to 30 is considered a positive screening result at most institutions. Some labs apply a threshold of >20 with an absolute aldosterone >15 ng/dL for higher specificity.
An important distinction: Some modern laboratories report direct renin concentration (DRC) in mIU/L rather than plasma renin activity. These are different assays with different normal ranges. When DRC is used, the ARR threshold shifts considerably — typically a threshold of >3.7 when PAC is in pmol/L, or specific thresholds published by the ordering laboratory. Always confirm which renin assay is in use before interpreting the result.
Worked example using PRA:
- Aldosterone: 18 ng/dL
- Plasma renin activity: 0.5 ng/mL/hr
- ARR = 18 ÷ 0.5 = 36 → Positive screen (above the 20–30 threshold)
A positive ARR alone does not confirm primary aldosteronism — it is a screening result that triggers confirmatory testing. False positives occur, and many interfering factors (see drug interference section) can elevate the ratio artificially. The ARR is most informative when the absolute aldosterone level is also elevated, not just the ratio.
Specimen Requirements — Timing and Position Matter
The ARR is one of the most posture- and protocol-sensitive laboratory tests in clinical medicine. Getting the draw wrong can make a sick patient look normal, or make a normal patient look sick.
Timing
Blood should be drawn in the morning, ideally between 8 and 10 AM. Aldosterone follows a diurnal rhythm and is highest in the morning. Afternoon draws may yield lower aldosterone values and falsely reassuring ratios.
Posture and Ambulation
The patient must have been upright and ambulatory for at least 2 hours before the draw. Renin is positionally responsive — lying flat suppresses it, which would artificially elevate the ARR. After arriving at the lab, the patient should be seated for 5–15 minutes before venipuncture to allow a brief stabilization.
Potassium Correction
Hypokalemia must be corrected before testing. This is not optional. Low potassium independently suppresses aldosterone secretion, which can falsely normalize both the aldosterone level and the ARR — a false negative at exactly the moment you most want to screen (hypokalemia is itself a red flag for primary aldosteronism). Potassium should be at or above 3.5 mEq/L on the day of testing. Oral potassium supplementation in the days leading up to the draw is standard protocol.
Sodium Intake
Adequate sodium intake is required. A low-sodium diet stimulates renin release, raising PRA and thereby lowering the ARR — a potential false negative. Patients should be eating a normal-to-liberal sodium diet (not actively salt-restricting) in the days before the test. Conversely, extremely high sodium intake suppresses renin maximally; this is generally less problematic but should be noted.
Other Pre-Analytical Variables
Avoid strenuous exercise on the morning of the draw. Ensure the patient is not acutely ill. Some protocols request avoiding NSAIDs for several days prior, as they can modestly affect renin.
Drug Interference: What to Stop and When
Multiple common medications interfere with the ARR, and managing them is often the most logistically complicated aspect of the workup. Stopping antihypertensives in a patient with resistant hypertension requires careful planning and supervision. Always coordinate with the treating physician before adjusting medications.
Medications That Must Be Stopped (4 Weeks Before)
- Spironolactone and eplerenone: Mineralocorticoid receptor antagonists are the most important washout. They block aldosterone receptors, causing a compensatory rise in both aldosterone and renin that renders the ARR uninterpretable. Four-week washout is required because of their long-acting metabolites.
Medications That Should Be Stopped if Possible (2 Weeks Before)
- Beta-blockers: Suppress renin secretion, which falsely elevates the ARR and can cause false-positive results. A 2-week washout is recommended when clinically feasible. If the patient cannot safely stop beta-blockers, results must be interpreted with this bias in mind.
- Central alpha-2 agonists (clonidine, methyldopa): Suppress renin, similar to beta-blockers.
- NSAIDs: Suppress renin; may elevate ARR.
Medications That May Cause False Negatives (2 Weeks Before, if Possible)
- ACE inhibitors and ARBs: Block the conversion or action of angiotensin II, reducing aldosterone production and raising renin. They lower the ARR and can mask primary aldosteronism with a false-negative result.
- Direct renin inhibitors (aliskiren): Similar mechanism, stimulate renin, lower ARR.
Acceptable Alternatives During Washout Phase
- Alpha-1 blockers (doxazosin, prazosin): Minimal effect on the renin-aldosterone axis. Recommended as a bridge antihypertensive during washout.
- Non-dihydropyridine calcium channel blockers (verapamil): Acceptable; some guidelines specifically recommend verapamil slow-release as a washout-phase antihypertensive.
- Dihydropyridine calcium channel blockers (amlodipine, nifedipine): Have minimal interference and are generally acceptable for the screening phase, though some modestly elevate renin.
- Hydralazine: Acceptable during washout for blood pressure control.
The washout phase in a patient with severe hypertension should always occur under medical supervision with home blood pressure monitoring and a clear plan for escalation if blood pressure becomes dangerous.
Confirmatory Tests
A positive ARR is a screening result only — it raises suspicion but does not confirm the diagnosis. The Endocrine Society guidelines recognize four accepted confirmatory tests. At least one must be performed before proceeding to imaging or adrenal vein sampling.
1. Oral Sodium Loading Test
The patient consumes a high-sodium diet (200 mEq/day, roughly 4,600 mg sodium) for 3 days, then collects a 24-hour urine aldosterone on day 3. An aldosterone excretion of >12 mcg/24 hours confirms primary aldosteronism. Sodium loading suppresses the renin-angiotensin system in a normal person, which would also suppress aldosterone — the autonomous gland fails to suppress. Potassium supplementation is usually needed during this test due to the natriuresis-driven kaluresis.
2. Intravenous Saline Infusion Test
Two liters of 0.9% normal saline infused over 4 hours in the morning in a recumbent or seated patient. A post-infusion aldosterone of >10 ng/dL confirms primary aldosteronism; <5 ng/dL makes it unlikely. The saline load expands plasma volume, suppressing renin and (in normal physiology) aldosterone. Autonomous aldosterone production fails to suppress. This test is contraindicated in patients with severe uncontrolled hypertension, heart failure, or significant arrhythmia.
3. Fludrocortisone Suppression Test (FST)
Considered by some experts to be the gold standard. The patient takes fludrocortisone 0.1 mg every 6 hours for 4 days along with sodium and potassium supplementation. An upright aldosterone >6 ng/dL at the end of the test, with a suppressed renin, confirms primary aldosteronism. Technically demanding and requires careful monitoring; hypokalemia is common and must be aggressively managed.
4. Captopril Challenge Test
The patient receives 25–50 mg oral captopril after being upright for 1–2 hours. In normal physiology, captopril (an ACE inhibitor) reduces angiotensin II and thereby suppresses aldosterone by at least 30%. In primary aldosteronism, aldosterone fails to suppress >30% from baseline at 1–2 hours post-dose. Easiest to perform; slightly lower sensitivity than saline infusion or oral loading.
Confirmatory tests are generally contraindicated in patients with severe uncontrolled hypertension (systolic >180 mmHg), severe uncorrected hypokalemia, or significant heart or kidney disease that would make volume loading dangerous.
Adrenal Vein Sampling: Lateralization
Once primary aldosteronism is biochemically confirmed, the critical next question is: which adrenal gland is responsible? The answer determines whether surgery is an option. Adrenal vein sampling (AVS) is the definitive test for lateralization.
The Procedure
AVS involves bilateral catheterization of the adrenal veins — a technically demanding procedure performed by experienced interventional radiologists — to measure aldosterone and cortisol concentrations simultaneously from the right adrenal vein, left adrenal vein, and a peripheral vein. ACTH stimulation (cosyntropin infusion) is typically used to maximize adrenal secretion and reduce procedural variability.
Interpreting the Results
Cortisol is measured alongside aldosterone to confirm successful catheterization of each vein (a selectivity index >3:1 cortisol in the adrenal vein vs. periphery is standard). The aldosterone-to-cortisol ratio is then compared between sides. A lateralization ratio >4:1 (some institutions use >3:1 with ACTH stimulation) from one side strongly suggests unilateral disease amenable to surgical cure via laparoscopic adrenalectomy.
Why CT and MRI Are Not Sufficient
This is one of the most important practical points in the entire primary aldosteronism workup: imaging alone cannot replace AVS. Up to 40% of CT-identified apparent adenomas turn out to be bilateral disease on AVS — and surgery on a patient with bilateral disease will fail to cure them. Conversely, bilateral adrenal hyperplasia can appear as a unilateral mass on CT. An incidentaloma on CT does not mean the incidentaloma is producing excess aldosterone. For any surgical candidate, AVS is mandatory before operating.
The exception is young patients (<35 years) with a clearly hypodense unilateral adenoma >1 cm on CT and spontaneous hypokalemia — in this narrow scenario, some guidelines accept proceeding to surgery without AVS due to the very high pretest probability of unilateral APA.
Treatment: Surgery vs. Medical Management
Unilateral Disease: Laparoscopic Adrenalectomy
For patients with a confirmed unilateral aldosterone-producing adenoma who are surgical candidates, laparoscopic adrenalectomy is the preferred treatment. Outcomes are excellent: 70–80% of patients achieve complete or substantial clinical cure — normal blood pressure off medications or on far fewer drugs. Biochemical cure (normalized aldosterone and renin) occurs in nearly 100% of properly selected patients.
Post-surgical hypoaldosteronism can transiently occur as the suppressed contralateral adrenal recovers — patients should be monitored for hyperkalemia in the weeks following surgery and may need brief fludrocortisone coverage.
Bilateral Disease or Surgical Ineligibility: Mineralocorticoid Receptor Antagonists
Patients with bilateral adrenal hyperplasia, or those who decline or cannot tolerate surgery, are managed medically:
- Spironolactone: First-line mineralocorticoid receptor antagonist. Highly effective at controlling blood pressure and correcting hypokalemia. Doses typically 25–100 mg daily. Anti-androgenic side effects (gynecomastia, reduced libido in men, menstrual irregularity in women) limit tolerability in some patients.
- Eplerenone: More selective mineralocorticoid receptor antagonist with fewer anti-androgenic effects, making it preferred in men troubled by spironolactone side effects. Requires higher doses; slightly less potent per mg. Twice-daily dosing typically needed.
- Amiloride: A potassium-sparing diuretic that blocks the epithelial sodium channel downstream of aldosterone. An alternative when MRAs are not tolerated, though less studied in primary aldosteronism specifically.
Potassium and magnesium supplementation may be needed initially, though they are often no longer required once effective MRA therapy is established. Blood pressure is frequently fully controlled without additional antihypertensive agents once mineralocorticoid excess is blocked. Lifelong monitoring of blood pressure, potassium, kidney function, and aldosterone is required regardless of treatment modality.
When to Screen for Primary Aldosteronism
The major barrier to diagnosis is that most physicians do not screen for it. The Endocrine Society and other guideline bodies have progressively expanded their screening recommendations as evidence of the condition's prevalence has accumulated.
Established High-Priority Indications
- Hypertension with spontaneous hypokalemia (potassium <3.5 mEq/L without diuretic use) — the classic presentation; virtually all of these patients should be screened
- Resistant hypertension: Blood pressure uncontrolled on three or more optimally dosed antihypertensives including a diuretic
- Hypertension with an adrenal incidentaloma: Any incidentally discovered adrenal mass in a hypertensive patient should prompt ARR screening
- Diuretic-induced hypokalemia that is severe (<3.0 mEq/L) or disproportionate to the diuretic dose
- Hypertension with obstructive sleep apnea: High co-prevalence with primary aldosteronism
- Family history of primary aldosteronism, or a family history of early-onset (<40 years) stroke — consider familial hyperaldosteronism type I (glucocorticoid-remediable aldosteronism) or type II
Expanding Indications
- Hypertension onset before age 40: Young hypertension should always prompt a secondary cause workup
- Stage 2 or higher hypertension (>160/100 mmHg): Many current guidelines recommend ARR screening for all patients in this category regardless of other features, given the 5–10% background prevalence
- Any new hypertension diagnosis where cure is desired and surgical candidacy exists: Some endocrinologists advocate universal screening given the low cost and potential for surgical cure in a subset
The practical message for patients: if you have high blood pressure that is hard to control, if you have ever had a low potassium on a blood test, or if your doctor found something on your adrenal gland by accident on a CT scan — ask whether you have been screened for primary aldosteronism. The test is simple, the diagnosis is common, and in many cases the condition is completely curable.
Research Papers and References
The following are curated PubMed literature searches on the major clinical topics covered in this article. Each link opens the relevant search results at PubMed.
- Primary aldosteronism prevalence in hypertension — PubMed Search
- Aldosterone-renin ratio screening for primary hyperaldosteronism — PubMed Search
- Primary hyperaldosteronism diagnosis and clinical guidelines — PubMed Search
- Conn syndrome and aldosterone-producing adrenal adenoma — PubMed Search
- Adrenal vein sampling and lateralization in primary aldosteronism — PubMed Search
- Spironolactone treatment outcomes in primary aldosteronism — PubMed Search
- Fludrocortisone suppression test for primary aldosteronism confirmation — PubMed Search
- Intravenous saline infusion test for aldosterone suppression — PubMed Search
- Aldosterone and cardiovascular risk beyond blood pressure — PubMed Search
- Mineralocorticoid receptor antagonists in resistant hypertension — PubMed Search
- Adrenalectomy outcomes and cure rates in primary aldosteronism — PubMed Search
- Primary aldosteronism and hypokalemia — PubMed Search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Hypertension
- Potassium
- Sodium
- Magnesium
- Complete Blood Count (CBC)
- Iron Panel
- Endocrinology Diseases
- Heavy Metals Panel