Myrrh for Wound Healing
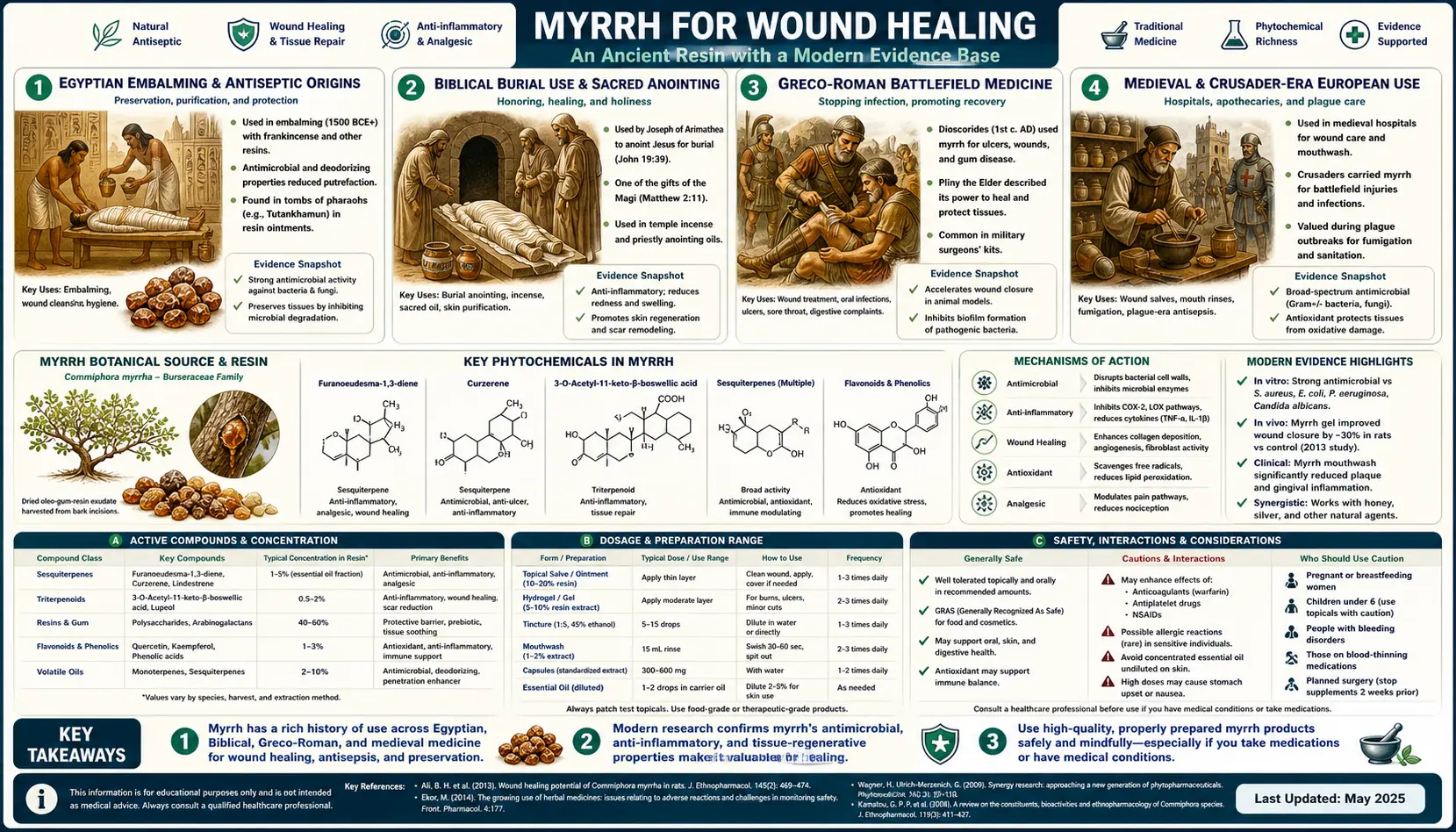
Wound treatment is the oldest documented use of myrrh and remains its single most cross-culturally consistent application. Egyptian embalmers were packing body cavities with myrrh resin to prevent putrefaction by 2700 BCE — not because they understood bacterial mechanisms, but because they observed empirically that myrrh-treated tissues resisted decomposition far longer than untreated remains. Roman legionary field surgeons carried myrrh in their medical kits for sword and arrow wounds. Greek physician Dioscorides described myrrh as "warming, drying, binding, and stopping the spread of gangrene." Crusaders brought renewed knowledge of myrrh's wound-treating value back to medieval Europe, where it became a staple of monastic infirmaries. Modern phytochemistry has decoded the mechanism: sesquiterpenes and commiphoric acids disrupt bacterial membranes (the antiseptic effect), resinous polymers cross-link surface proteins to seal weeping tissue (the astringent effect), and furanosesquiterpenes activate mu-opioid receptors to dampen wound pain. This page covers the historical record, the modern topical trials, the mechanism, and the dosing considerations for using myrrh on wounds today.
Table of Contents
- Egyptian Embalming and Antiseptic Origins
- Biblical Burial Use and Sacred Anointing
- Greco-Roman Battlefield Medicine
- Medieval and Crusader-Era European Use
- Modern Topical Wound Trials
- Sesquiterpene Membrane Disruption
- Astringent Protein Cross-Linking
- Mirazid — The Egyptian Pharmaceutical Crossover
- Practical Topical Application Today
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Egyptian Embalming and Antiseptic Origins
The earliest documented use of myrrh comes from Pharaonic Egypt, where the resin was central to the elaborate mummification process that aimed to preserve the body for an envisioned afterlife. Egyptian embalmers, working in temple workshops from roughly 2700 BCE through the Roman period, used myrrh as a primary preservative agent. After removing the brain and most of the abdominal organs, the embalmers packed the body cavity with a mixture that prominently featured myrrh resin alongside natron (a naturally occurring sodium salt mixture from desert lake beds), cinnamon, cassia, and other aromatic substances. The body was then wrapped in linen strips that had been impregnated with more myrrh and resinous oils.
The Egyptians did not understand bacteria, fungi, or putrefaction in modern biochemical terms. They worked from empirical observation of what preserved tissue and what did not. Myrrh-packed bodies resisted decomposition over thousands of years — modern radiocarbon-dated mummies from the New Kingdom (1550-1070 BCE) and earlier still show identifiable myrrh chemical signatures in their preserved tissues, detected through gas chromatography-mass spectrometry analysis of mummy fragments. The Ebers Papyrus, dated to approximately 1550 BCE and one of the oldest comprehensive medical texts in existence, lists myrrh in dozens of formulations for treating wounds, infections, skin diseases, and digestive complaints. Egyptian physicians prescribed myrrh-based preparations for cleaning infected wounds (the recipe in the Ebers Papyrus calls for ground myrrh mixed with honey applied to the wound), treating oral ulcers, and managing the discharging wounds of soldiers and laborers.
The mechanism the Egyptian embalmers were unwittingly exploiting is the same one modern phytochemistry identifies: the sesquiterpene and commiphoric acid fractions of myrrh resin are powerfully antimicrobial against the bacteria and fungi that drive putrefaction. Combined with the desiccating effect of natron (which essentially mummifies tissue by drawing out water through osmotic pressure), the antimicrobial properties of myrrh produced preservation that has survived three to four thousand years of subsequent burial.
Biblical Burial Use and Sacred Anointing
Myrrh occupies an exalted status in the Biblical record. It was one of the three gifts presented by the Magi to the infant Jesus in the Gospel of Matthew (along with gold and frankincense) — symbolically representing suffering, mortality, and the burial that the gift's recipient would eventually receive. It appears throughout the Old Testament: as a primary component of the holy anointing oil described in Exodus 30:23-25 (combined with cinnamon, calamus, cassia, and olive oil); referenced repeatedly in the Song of Solomon as a perfume of great value (Song of Solomon 1:13, 3:6, 4:6, 5:1, 5:5, 5:13); and recorded in the Book of Esther as the substance used in the six-month preparation period for women presented to King Xerxes (Esther 2:12).
In Jewish burial customs of the Second Temple period, myrrh was used to anoint the bodies of the dead, both for its aromatic value and for its preservative properties. The Gospel of John (John 19:39-40) records that Nicodemus brought approximately 75 pounds (Roman libra, equivalent to about 32 kg in modern units) of myrrh and aloes to prepare the body of Jesus for burial — a strikingly large quantity that reflects both the economic value placed on a proper burial and the practical preservation function the substance was intended to serve. This was wound and tissue preservation in the most literal sense: the substance applied to a body that had sustained crucifixion wounds, intended both to slow decomposition and to honor the deceased.
The continuity between the Egyptian, Jewish, and early Christian uses of myrrh reflects a single mechanism applied to a single set of biological problems: the preservation of human tissue from microbial degradation. The cultural framing differs — Egyptian magical preservation, Jewish purification ritual, Christian symbolism — but the underlying material practice is the same, exploiting myrrh's antimicrobial and astringent properties to retard tissue breakdown.
Greco-Roman Battlefield Medicine
Greek and Roman physicians made extensive use of myrrh as a wound medicine, and the Roman army made it a standard component of military field medicine. Hippocrates (c. 460-370 BCE) recommended myrrh for treating sores, fistulas, and infected wounds. Dioscorides, in his influential first-century text De Materia Medica, described myrrh in terms that translate roughly as: "warming, drying, binding, stopping the spread of gangrene, fastening loose teeth, drying running sores, and clearing wounds of putrefaction." Dioscorides specified preparations for both topical and internal use and noted the distinction between Arabian myrrh (preferred for medicinal use) and the inferior Indian product (sometimes substituted by unscrupulous merchants).
The Roman army carried myrrh in standard-issue field medical kits, alongside vinegar (for wound irrigation), honey (for dressing burns and sores), and various herbal preparations. Roman military surgeons applied ground myrrh resin directly to sword cuts, arrow wounds, and other combat injuries. The resin served multiple functions in this setting: as an astringent that helped control bleeding from cut tissues, as an antiseptic that prevented or controlled wound infection (a leading cause of death in Roman military operations), and as a pain-reducing agent through its mu-opioid receptor effects (though Roman physicians of course had no understanding of opioid pharmacology). Pliny the Elder documented myrrh's use in treating mouth ulcers, strengthening teeth, alleviating respiratory congestion, and dressing combat wounds. Galen, the most prominent physician of the Roman Empire and personal physician to several emperors, included myrrh in his polypharmacy preparations and prescribed it across the spectrum of infectious and inflammatory conditions.
The persistence of this Greco-Roman use through nearly a thousand years of European practice is one of the most striking examples of empirical observation surviving the cultural and political disruptions of the period. Even during the Roman Empire's decline, monasteries preserved the medical texts of Dioscorides and Galen, and myrrh remained a standard wound medicine in the European materia medica that emerged from the medieval medical schools at Salerno, Bologna, and Padua.
Medieval and Crusader-Era European Use
European medicine in the early medieval period largely lost direct trade access to the Horn of Africa myrrh supply chain and depended on limited imports through Byzantine and Arab intermediaries. The Crusades (1095-1291 CE) re-established direct European exposure to Eastern Mediterranean medical practice, including renewed knowledge of myrrh's wound-treating value and improved supply chains that brought larger quantities of resin back to European apothecaries. Crusader-era European wound salves frequently incorporated myrrh alongside other Arab-Mediterranean substances such as frankincense, mastic, and aloe.
The medieval Latin pharmacopoeia included multiple myrrh-based preparations: unguentum aegyptiacum (Egyptian ointment) for cleaning chronic ulcers and discharging wounds; tinctura myrrhae (myrrh tincture in alcohol) for topical antiseptic application; pulvis myrrhae (powdered myrrh) for direct application to fresh wounds; and various complex compound salves that combined myrrh with honey, beeswax, lard, and other ingredients. The monastic infirmaries that provided much of the available organized healthcare in medieval Europe maintained substantial stocks of myrrh and trained their lay-brother infirmarians in its preparation and use.
The transition from medieval to early modern medicine retained myrrh as a standard wound medicine. Paracelsus (1493-1541) included myrrh in his characteristic combination preparations. The London Pharmacopoeia of 1618 and the Edinburgh Pharmacopoeia of 1699 both listed myrrh tincture as an official preparation for wound and oral mucosal use. The British Pharmacopoeia maintained an official myrrh monograph through the nineteenth and into the twentieth century, and myrrh tincture remained a standard wound antiseptic in many European countries until it was largely displaced by synthetic antibiotic and antiseptic preparations after World War II.
Modern Topical Wound Trials
Modern clinical research on myrrh in wound healing is less voluminous than the historical record — the herb predates patentable pharmaceutical interest and lacks the regulatory pathway that would justify large industry-funded trials. However, the published research that does exist is generally supportive and consistent with the historical empirical use.
Haffor's 2010 study in the Journal of Immunotoxicology examined the effect of Commiphora molmol myrrh on leukocyte profiles during healing from gastric ulcer and skin injury in rats. The treated animals showed accelerated wound closure, increased fibroblast proliferation in the wound bed, and more rapid resolution of the inflammatory leukocyte infiltrate compared to untreated controls. The accelerated transition from inflammatory to proliferative phase of wound healing is precisely what is desired in chronic wound management, where prolonged inflammation often impedes closure.
Hydroalcoholic extract studies (Galehdari et al. and others) have evaluated topical myrrh preparations on experimentally induced wounds in rat and mouse models. The consistent findings: faster epithelialization (epidermal regrowth across the wound bed), increased collagen deposition (measured by hydroxyproline content of healed tissue), higher tensile strength of healed tissue (measured by tensiometric testing of excised wound strips), and lower rates of bacterial colonization in the early wound healing phase.
Burn wound studies have shown that topical myrrh-based ointments accelerate healing of partial-thickness burns in animal models and reduce the rate of secondary bacterial colonization. The mechanism appears to combine direct antibacterial action (reducing the pathogen load that would otherwise drive wound chronification), anti-inflammatory action (reducing the excessive inflammatory response that can impede burn healing), and direct stimulation of fibroblast proliferation and angiogenesis (the formation of new blood vessels in healing tissue, essential for adequate oxygen and nutrient delivery to regenerating skin).
Diabetic wound studies, while limited, have shown promising results with myrrh-containing topical preparations in animal models of diabetic ulceration. Diabetic wounds are particularly challenging because they combine impaired immune function, microvascular insufficiency, and prolonged inflammatory phase — the same combination that myrrh's mechanism of action addresses. Human clinical trials of myrrh for diabetic foot ulcers remain very limited, but the preclinical foundation supports further investigation. For more on diabetic complications including foot ulcers, see our Diabetes page.
Sesquiterpene Membrane Disruption
The antibacterial component of myrrh's wound-healing action is driven primarily by sesquiterpenes — volatile 15-carbon terpenoid molecules concentrated in the essential oil fraction of the resin. Myrrh essential oil typically constitutes 2-8% of the raw resin and contains over 200 identified compounds, with sesquiterpenes accounting for the dominant fraction. The principal antibacterial sesquiterpenes include curzerene (15-30% of myrrh oil), furanoeudesma-1,3-diene (5-20%), lindestrene (5-15%), beta-elemene, delta-elemene, beta-eudesmol, and alpha-copaene. The furanosesquiterpenes (furanodiene, furanodienone, isofuranogermacrene) are particularly distinctive because they are uncommon outside the Commiphora genus.
The mechanism of action is well-characterized. Sesquiterpenes are lipophilic small molecules that integrate into the phospholipid bilayer of bacterial cell membranes. Once embedded in the membrane, they disrupt the ordered arrangement of fatty acid chains, increasing membrane fluidity and permeability. This leads to uncontrolled leakage of intracellular contents, including potassium ions, ATP, nucleotides, and proteins. The resulting collapse of the transmembrane electrochemical gradient (proton motive force) halts ATP synthesis and active transport processes, leading to rapid cell death. Studies using electron microscopy have confirmed that myrrh-treated bacteria exhibit extensive membrane blebbing, pore formation, and eventual cell lysis.
The bacterial spectrum is broad. Myrrh sesquiterpenes have demonstrated activity against Gram-positive cocci (Staphylococcus aureus, including methicillin-resistant strains (MRSA); Streptococcus pyogenes, the cause of skin infections including impetigo and cellulitis), Gram-negative rods (Escherichia coli, Pseudomonas aeruginosa — though at higher concentrations due to the outer membrane barrier), and oral pathogens. For wound treatment specifically, the relevance is the spectrum of common skin and wound pathogens that myrrh covers: S. aureus is the leading cause of skin and soft-tissue infections worldwide, S. pyogenes is the leading cause of cellulitis, and both are reliably inhibited by topical myrrh preparations at clinically achievable concentrations.
An important property is the resistance landscape: bacteria that have evolved resistance to conventional antibiotics generally do not show cross-resistance to myrrh sesquiterpenes. The mechanisms of antibiotic resistance — beta-lactamase enzymes, efflux pumps, target-site mutations, ribosomal protection proteins — do not protect against membrane disruption by lipophilic terpenoids. This makes myrrh and similar plant-derived antimicrobials potentially useful adjuncts in the management of multi-drug-resistant wound infections, though clinical translation has been limited.
Astringent Protein Cross-Linking
Beyond the antibacterial action, myrrh produces a distinct astringent effect on wound surfaces. Astringents are substances that contract and seal tissues by cross-linking surface proteins. The classic astringent mechanism is the binding of tannin-like polyphenolic molecules to proteins in mucosal or wound surfaces, creating a thin protein-tannin precipitate film that mechanically reduces oozing, contracts dilated capillary beds, and protects the underlying tissue from further injury.
Myrrh is not a true tannin-containing herb (its astringent action does not come from gallic-acid-based tannins like those in oak bark or witch hazel), but its resinous fraction contains compounds with analogous protein-binding capacity. The commiphoric acids and the resin polymers cross-link proteins on the wound surface and produce the characteristic astringent effect: a thin, slightly puckered film of dried resin and precipitated protein that mechanically seals the wound surface, reduces fluid weeping, and provides a barrier against further bacterial contamination.
The astringent effect is most clinically valuable in wounds that are oozing, weeping, or hemorrhaging from disrupted small blood vessels. Battlefield wounds, partial-thickness burns, abrasions, surgical wound dehiscence, and chronic ulcers with seropurulent discharge all benefit from astringent application. The mechanical reduction of fluid loss helps maintain wound bed moisture balance (too dry impedes healing, too wet promotes maceration), and the precipitated protein film provides some mechanical protection against secondary trauma during the early healing phase.
The astringent action also helps explain why myrrh was used historically as a hemostatic agent for minor bleeding wounds. The protein cross-linking effect contracts the cut ends of small blood vessels in the wound bed and reduces continuing oozing — an effect distinct from the platelet aggregation cascade and not dependent on intact coagulation. For minor superficial bleeding, topical myrrh powder or tincture can meaningfully reduce blood loss.
The combination of antibacterial action (sesquiterpenes) and astringent action (resinous polymers) in a single preparation is what makes myrrh distinctive among traditional wound medicines. Most herbs offer one or the other — either an antimicrobial volatile oil (tea tree, oregano, thyme) or an astringent tannin (oak bark, witch hazel, raspberry leaf). Myrrh combines both in approximately equal measure, which explains its persistent presence across nearly every traditional materia medica that had access to it.
Mirazid — The Egyptian Pharmaceutical Crossover
Mirazid is a pharmaceutical preparation of purified Commiphora molmol myrrh oleoresin manufactured by the Egyptian company Pharco Pharmaceuticals and approved by the Egyptian Ministry of Health in 2001 for the treatment of schistosomiasis and fascioliasis. While its primary indication is parasitic infection rather than wound healing (covered in detail on the Antimicrobial & Parasitic page), Mirazid is relevant here because it represents a rare modern example of a traditional herbal remedy successfully navigating the regulatory pathway to become an approved pharmaceutical product.
The relevance to wound healing is twofold. First, the existence of Mirazid demonstrates that standardized, quality-controlled, pharmacologically active myrrh preparations are technically feasible — the obstacles to broader pharmaceutical development of myrrh-based wound products are commercial and regulatory rather than scientific. Second, the manufacturing process developed for Mirazid — controlled extraction of resin oleo-gum, defined sesquiterpene content, standardized dosing — provides a template for how myrrh-based topical wound preparations could be standardized for clinical use beyond the current craft-scale herbalist preparations.
The Egyptian regulatory acceptance of Mirazid was based on clinical trials demonstrating efficacy against Schistosoma mansoni, Schistosoma haematobium, and Fasciola hepatica infections, with cure rates initially reported at 90% or higher in the early 2000s clinical studies (Sheir et al. 2001, Massoud et al. 2001). Subsequent independent studies produced more variable results, and the use of Mirazid as a first-line antischistosomal agent has been somewhat displaced by praziquantel in most clinical settings. But the regulatory approval itself stands, and Mirazid remains available as a registered pharmaceutical product in Egypt and a small number of other Middle Eastern countries.
For wound healing applications, the closest analog to Mirazid is the European Medicines Agency monograph for Myrrhae tinctura (myrrh tincture), which provides a regulatory framework for myrrh tincture as an approved herbal medicinal product for topical use on minor oral and pharyngeal mucosal inflammations. The wound-healing indication has not been formalized through the EMA process, but the basic regulatory acceptance of myrrh as a topical therapeutic agent has been established.
Practical Topical Application Today
For practical contemporary use of myrrh on wounds, the available preparations and their applications are:
- Myrrh tincture (1:5 in 90% ethanol) — the most accessible and best-documented preparation. For minor wound antisepsis, dilute 2-4 mL of tincture in 100 mL of clean water and use as a wound wash. For chronic ulcers or weeping wounds, apply diluted tincture directly to the wound bed with a clean swab once or twice daily, then cover with a clean dressing. The alcohol carrier provides additional antiseptic action.
- Powdered myrrh resin — finely ground myrrh can be applied directly to fresh wounds as an antiseptic and hemostatic dust, particularly useful for minor abrasions, shallow lacerations, or oozing surgical site margins. The traditional Roman field application is essentially the same technique used today by herbalists.
- Myrrh essential oil (diluted) — the concentrated essential oil should never be applied undiluted to wound tissue (risk of irritation and contact dermatitis). For topical wound use, dilute to 2-5% in a carrier oil such as jojoba, coconut, or olive oil. The diluted oil is suitable for application around (rather than directly into) wound margins, or for treatment of mild skin inflammation adjacent to wounds.
- Myrrh-containing commercial wound products — several European wound salves and ointments contain myrrh extract as an active ingredient, often in combination with frankincense, propolis, or other antimicrobial herbs. These offer consistent dosing and predictable concentration compared to home preparations.
- Myrrh + honey poultice (traditional) — a traditional preparation that combines myrrh's antiseptic action with honey's antibacterial and hygroscopic (moisture-managing) effects. Mix powdered myrrh resin with raw honey to form a paste, apply to the wound, and cover with a clean dressing. The combination is particularly well-suited to chronic ulcers and minor burns. See our Manuka Honey page for more on honey wound treatment.
For any wound serious enough to require medical attention (deep lacerations, puncture wounds, animal bites, wounds with retained foreign material, large burns, wounds showing signs of significant infection such as expanding cellulitis or systemic illness), professional medical evaluation is essential. Myrrh is a useful adjunct for minor wound management but is not a substitute for surgical debridement, suture closure, or systemic antibiotic therapy when these are indicated. The traditional record establishes myrrh as a complement to surgical wound management, not a replacement for it.
Cautions and Contraindications
- Pregnancy is an absolute contraindication for internal use, and topical use should be limited. Myrrh is a documented uterine stimulant that can induce uterine contractions and has been historically used as an emmenagogue (agent to promote menstruation). Even topical application of significant amounts can produce systemic absorption sufficient to affect uterine activity. Pregnant women should avoid all internal myrrh use and limit topical use to very small areas if it is used at all.
- Anticoagulant interactions — myrrh has documented platelet-inhibitory effects and can potentiate the action of warfarin, heparin, aspirin, clopidogrel, and direct oral anticoagulants. Patients on anticoagulant therapy should consult their physician before significant myrrh use, including extensive topical application to large wounds where systemic absorption is meaningful.
- Surgical procedures — for the same reason, myrrh should be discontinued at least two weeks before any scheduled surgical procedure to minimize the risk of excessive intraoperative or postoperative bleeding.
- Contact dermatitis — allergic contact reactions to topical myrrh have been documented, particularly with undiluted essential oil. A small patch test on the inner forearm before first use of a new preparation is prudent, especially for individuals with known sensitivity to other resinous plants (frankincense, mastic, or pine resin).
- Diabetes medication interactions — significant systemic exposure to myrrh can lower blood glucose and potentiate insulin and oral hypoglycemics. For most topical wound applications, the systemic exposure is minimal and this is not clinically relevant; for large-area topical use or any internal use, diabetic patients should monitor blood glucose more closely.
- Open puncture wounds — deep puncture wounds (particularly from contaminated objects like garden tools, animal bites, or human bite wounds) carry a significant risk of Clostridium tetani contamination and tetanus. Topical myrrh is not a substitute for tetanus prophylaxis — verify tetanus vaccination status and seek medical evaluation for any deep puncture wound.
- Children — internal use of myrrh in young children is generally not recommended due to limited safety data. Topical use in small amounts for minor wounds is generally considered safe but should be discussed with a pediatrician for any wound serious enough to require ongoing care.
Key Research Papers
- Haffor AS (2010). Effect of myrrh (Commiphora molmol) on leukocyte levels before and during healing from gastric ulcer or skin injury. Journal of Immunotoxicology. — PubMed
- Rahman MM et al. (2008). Antibacterial terpenes from the oleo-resin of Commiphora molmol. Phytotherapy Research. — PubMed
- Sheir Z et al. (2001). A safe, effective herbal antischistosomal therapy derived from myrrh. American Journal of Tropical Medicine and Hygiene. — PubMed
- Dolara P et al. (1996). Analgesic effects of myrrh. Nature. — PubMed
- Hanus LO et al. (2005). Myrrh — commiphora chemistry. Biomedical Papers. — PubMed
- Shen T et al. (2012). The genus Commiphora: a review of its traditional uses, phytochemistry and pharmacology. Journal of Ethnopharmacology. — PubMed
- Nomicos EY (2007). Myrrh: medical marvel or myth of the Magi? Holistic Nursing Practice. — PubMed
- Su S et al. (2011). Anti-inflammatory and analgesic activity of different extracts of Commiphora myrrha. Journal of Ethnopharmacology. — PubMed
- Massoud A et al. (2001). Preliminary study of the therapeutic efficacy of a new fasciolicidal drug derived from Commiphora molmol. — PubMed
- de Rapper S, Van Vuuren SF et al. (2012). The additive and synergistic antimicrobial effects of select frankincense and myrrh oils. Letters in Applied Microbiology. — PubMed
- Mahboubi M, Kashani LM (2016). The anti-dermatophyte activity of Commiphora molmol. Pharmaceutical Biology. — PubMed
- Tonkal AM, Morsy TA (2008). An update review on Commiphora molmol and related species. Journal of the Egyptian Society of Parasitology. — PubMed
PubMed Topic Searches
- PubMed: Myrrh wound healing
- PubMed: Burn / ulcer topical
- PubMed: Sesquiterpene mechanism
- PubMed: Mirazid pharmaceutical
- PubMed: Astringent hemostatic action
Connections
- Myrrh Overview
- Myrrh Benefits Hub
- Myrrh for Oral Health
- Myrrh Anti-Inflammatory
- Myrrh Antimicrobial & Parasitic
- Boswellia (Frankincense)
- Manuka Honey (Wound Honey)
- Goldenseal
- Tea Tree
- Neem
- Silver Nanoparticles
- Staphylococcus aureus (MRSA)
- Fungal Infections
- Diabetes (Diabetic Wounds)
- All Herbs