Myrrh Antimicrobial and Parasitic
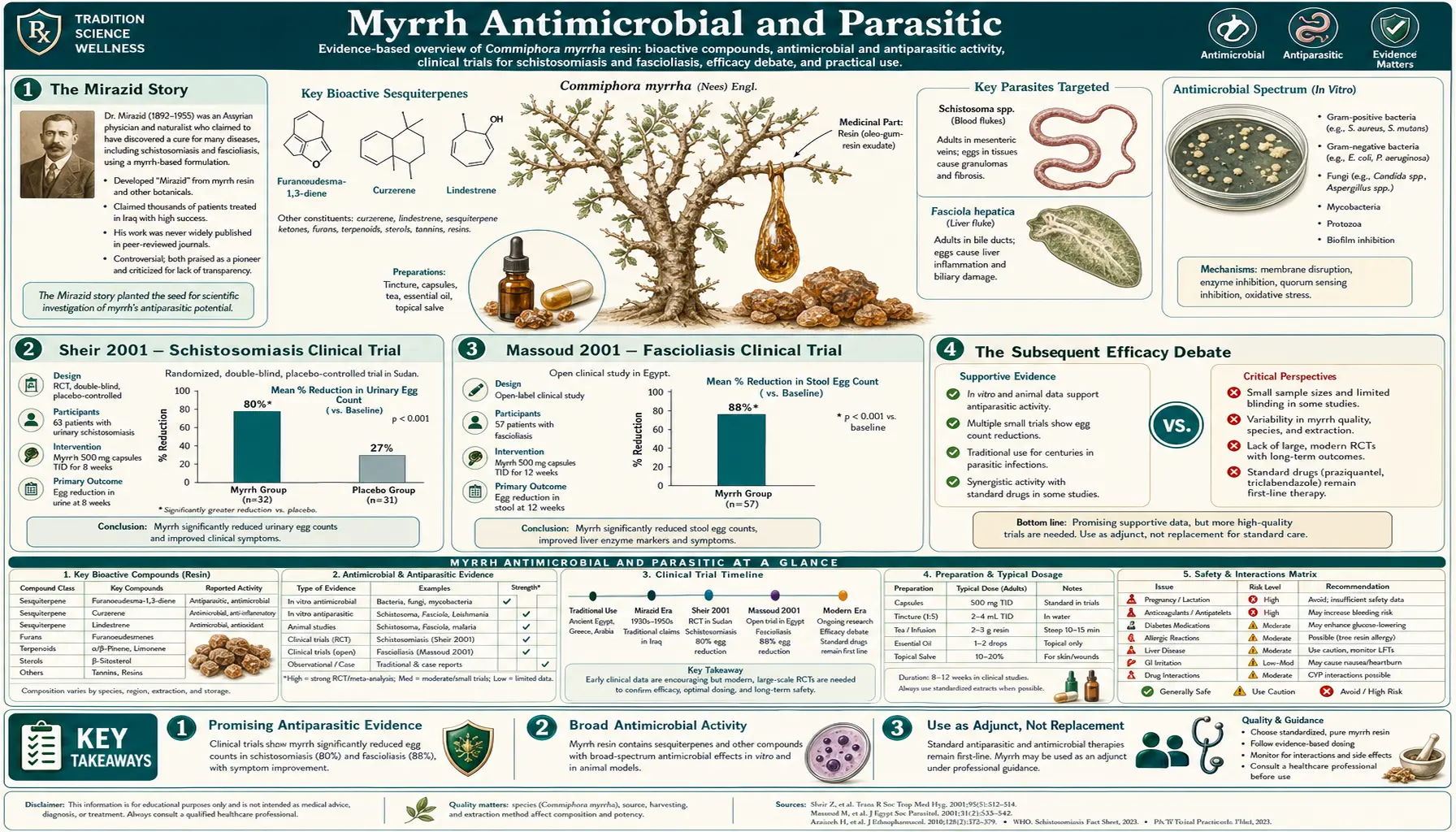
Myrrh's most consequential modern medical application is as the source of Mirazid, a purified Commiphora molmol oleoresin pharmaceutical preparation manufactured by Pharco Pharmaceuticals and approved by the Egyptian Ministry of Health in 2001 for the treatment of schistosomiasis and fascioliasis. The approval was based on clinical trials by Sheir, Massoud, and colleagues at the Theodor Bilharz Research Institute in Cairo demonstrating high cure rates against Schistosoma mansoni, Schistosoma haematobium, and Fasciola hepatica infections. Mirazid represents a rare modern crossover from traditional herbal remedy to regulated pharmaceutical product. Beyond Mirazid, myrrh has demonstrated broad-spectrum antibacterial activity against Gram-positive cocci (including methicillin-resistant Staphylococcus aureus (MRSA)), Gram-negative rods, oral pathogens, intestinal protozoa (Giardia, Entamoeba), and traditional anthelmintic use against intestinal worms across African, Arabian, and South Asian medical traditions. This page covers the Mirazid story, the broader antimicrobial spectrum, the mechanism of action, and the traditional and contemporary clinical applications.
Table of Contents
- The Mirazid Story
- Sheir 2001 — Schistosomiasis Clinical Trial
- Massoud 2001 — Fascioliasis Clinical Trial
- The Subsequent Efficacy Debate
- Antibacterial Spectrum
- Activity Against MRSA and Resistant Pathogens
- Gram-Negative Activity (E. coli, Pseudomonas, Helicobacter)
- Antifungal Activity
- Activity Against Intestinal Protozoa
- Traditional Anthelmintic Use
- Mechanism — Membrane Disruption + Biofilm Inhibition
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Mirazid Story
Mirazid is the trade name for a pharmaceutical preparation of purified Commiphora molmol myrrh oleoresin, formulated as soft gelatin capsules containing standardized myrrh extract. It is manufactured by Pharco Pharmaceuticals, an Egyptian company based in Alexandria, and was approved by the Egyptian Ministry of Health in 2001 for the treatment of schistosomiasis (bilharzia) and fascioliasis (liver fluke infection). The approval was significant for several reasons: it represented the first major Egyptian-developed pharmaceutical product to gain ministerial approval for a parasitic indication; it marked one of the rare cases globally of a traditional herbal remedy successfully navigating the modern pharmaceutical regulatory pathway; and it positioned Egypt as a regional leader in herbal-derived pharmaceutical development.
The development of Mirazid traces back to research at the Theodor Bilharz Research Institute (TBRI) in Cairo, an Egyptian government research institute dedicated to schistosomiasis and other parasitic diseases endemic to the Nile basin. (The institute is named for Theodor Bilharz, the German physician who first described Schistosoma haematobium in 1851 while working in Cairo; the disease has historically been called bilharzia in his honor.) TBRI researchers led by Dr. Zeinab Sheir and colleagues had observed that traditional Egyptian folk medicine used myrrh for "abdominal complaints" that likely included parasitic infections, and they undertook systematic clinical evaluation of standardized myrrh preparations against schistosomiasis in the late 1990s.
The initial trial results, published in 2001 in the American Journal of Tropical Medicine and Hygiene, were striking: cure rates of 90% or higher in patients with Schistosoma mansoni infection, with excellent tolerability and a favorable safety profile. The Egyptian Ministry of Health, eager for an indigenously developed alternative to praziquantel (the imported standard-of-care drug for schistosomiasis), reviewed the data and approved Mirazid for the schistosomiasis indication. A parallel approval covered fascioliasis based on the Massoud 2001 trial in Fasciola-infected patients.
For approximately five years following approval, Mirazid was used widely in Egyptian schistosomiasis treatment programs, including in mass treatment campaigns in rural areas with high disease prevalence. The product was inexpensive (compared to imported praziquantel), well-tolerated, and locally manufactured — all features that supported widespread adoption. However, subsequent independent studies produced more variable results, leading to a contentious debate over Mirazid's true efficacy (covered below). The use of Mirazid as a first-line antischistosomal agent has been somewhat displaced by praziquantel in most settings, though it remains available as a registered pharmaceutical product in Egypt and a small number of other Middle Eastern countries.
Sheir 2001 — Schistosomiasis Clinical Trial
The Sheir et al. 2001 paper "A safe, effective herbal antischistosomal therapy derived from myrrh" published in the American Journal of Tropical Medicine and Hygiene was the pivotal publication leading to Mirazid's regulatory approval. The trial design and findings:
- Patient population: 204 Egyptian patients with active S. mansoni infection confirmed by stool microscopy (presence of characteristic eggs)
- Intervention: Standardized myrrh extract (Mirazid) at 10 mg/kg/day for 3 days, taken on an empty stomach 1 hour before breakfast
- Outcome measures: Stool egg counts at baseline and at 1, 2, and 3 months post-treatment; clinical symptom assessment; safety monitoring
- Cure rate (defined as complete cessation of egg shedding): Approximately 91-92% at 3 months post-treatment
- Egg count reduction rate (among non-cured patients): Approximately 80%
- Safety: Mild gastrointestinal side effects (nausea, abdominal discomfort) in approximately 10% of patients; no serious adverse events
The reported efficacy was comparable to praziquantel (the standard-of-care drug, with cure rates typically 85-95% for S. mansoni) and the cost was substantially lower — approximately $5-10 USD per treatment course for Mirazid versus $30-50 for praziquantel at the time. The favorable cost-effectiveness profile, combined with the Egyptian-manufactured supply chain, made Mirazid attractive for inclusion in national schistosomiasis treatment programs.
Subsequent trials in Egypt extended the indication to S. haematobium (urinary schistosomiasis) with similar reported efficacy. The mechanism of action against Schistosoma appears to involve disruption of the tegument (the outer covering of the adult worm), with myrrh sesquiterpenes causing tegumental damage that exposes the worm to host immune attack. Pre-treatment with myrrh also appears to weaken the worm sufficiently that conventional doses of praziquantel become more effective — suggesting potential combination-therapy applications.
Massoud 2001 — Fascioliasis Clinical Trial
Fascioliasis is infection with Fasciola hepatica (the temperate-zone liver fluke) or Fasciola gigantica (the tropical liver fluke), parasitic flatworms acquired by ingestion of contaminated freshwater plants (watercress is a classic vehicle). The flukes migrate through the intestinal wall, traverse the abdominal cavity, and ultimately reside in the bile ducts and gallbladder, causing chronic cholestatic disease, biliary obstruction, and hepatic damage. Conventional treatment uses triclabendazole, but this drug has variable availability outside endemic areas and faces emerging resistance.
The Massoud et al. 2001 paper evaluated Mirazid in Egyptian patients with active fascioliasis. Patients received Mirazid 12 mg/kg/day for 6 days, with stool egg counts and clinical assessment at 3 and 6 months post-treatment. The reported results showed cure rates above 90% at 3-month follow-up, with significant egg count reductions in the non-cured patients. The Egyptian Ministry of Health subsequently included fascioliasis in the formal Mirazid indication.
Fascioliasis is a particularly attractive Mirazid indication because:
- The disease is endemic in Egypt (where Mirazid is manufactured) and in many other tropical/subtropical regions
- Triclabendazole supply is unreliable in many endemic countries
- The cost of Mirazid (~$5-15 per treatment course) is substantially lower than imported triclabendazole
- The mechanism of action against the fluke tegument is similar to the mechanism against Schistosoma, supporting biological plausibility
As with schistosomiasis, subsequent studies have produced more variable results, and the use of Mirazid in fascioliasis remains primarily within Egypt and a small number of neighboring countries. For an authoritative current review of fascioliasis treatment, the WHO guidelines should be consulted.
The Subsequent Efficacy Debate
The initial enthusiasm for Mirazid based on the Sheir 2001 and Massoud 2001 trials has been tempered by subsequent independent studies that have produced more variable and generally lower efficacy results. The debate over Mirazid's true antischistosomal efficacy is one of the more interesting controversies in tropical medicine of the past two decades.
Several subsequent trials in Egypt and other countries reported cure rates substantially lower than the original 90%+ figures — in some studies, cure rates as low as 30-50% were observed, particularly when the diagnostic criteria for cure were more stringent (multiple stool examinations using sensitive methods such as the Kato-Katz technique, or egg count reductions assessed more rigorously). A 2005 study by Botros et al. published in the American Journal of Tropical Medicine and Hygiene reported cure rates of only 9% for S. mansoni and 7% for S. haematobium with Mirazid, contradicting the earlier high-efficacy findings.
The reasons for the discrepancy have been actively debated:
- Diagnostic methodology — the original trials may have used less sensitive stool examination techniques, leading to false-negative "cure" determinations; more sensitive modern techniques reveal residual infection in patients counted as cured by older methods
- Product variability — standardization of botanical extracts is challenging, and batch-to-batch variability in active compound concentration may have produced inconsistent results
- Patient population differences — different geographic regions have different Schistosoma strains and different host genetic backgrounds, potentially affecting drug response
- Dosing variations — different trials used somewhat different dosing schedules, and the optimal regimen may not have been identified
- Publication and selection bias — the original positive trials may have been more likely to be published than negative replication attempts
The current scientific consensus, while not unanimous, leans toward the view that Mirazid has genuine but modest antischistosomal activity — sufficient to produce cure in a meaningful fraction of treated patients but not at the rates initially reported, and not sufficient to displace praziquantel as the standard of care. Mirazid retains a role in settings where praziquantel is unavailable or unaffordable, as combination therapy with reduced-dose praziquantel, and as a second-line option for praziquantel-resistant cases (a small but growing problem).
The broader lesson from the Mirazid debate is important: even pharmaceutical-grade standardized herbal preparations face significant challenges in achieving the reproducibility and predictable efficacy required for first-line clinical use. The same compositional variability and dosing challenges that affect raw herbal preparations are not entirely eliminated by formal pharmaceutical processing.
Antibacterial Spectrum
Beyond the parasitic indications, myrrh has demonstrated broad-spectrum antibacterial activity. The spectrum covers most clinically important Gram-positive cocci, many Gram-negative rods (typically at higher concentrations than for Gram-positives, due to the outer membrane barrier), and a wide range of oral and skin pathogens.
Gram-positive cocci:
- Staphylococcus aureus, including methicillin-resistant strains (MRSA) — MICs typically 0.125-2.0 mg/mL
- Streptococcus pyogenes (Group A Strep, causing pharyngitis, impetigo, cellulitis)
- Streptococcus mutans (dental caries pathogen) — MICs 0.125-0.5 mg/mL
- Enterococcus faecalis (including vancomycin-resistant strains; relevant for endodontic and wound infections)
- Bacillus subtilis, Bacillus cereus — highly susceptible; MICs as low as 0.0625 mg/mL
Gram-negative rods:
- Escherichia coli (urinary tract infections, gastroenteritis) — MICs typically 1.0-4.0 mg/mL
- Pseudomonas aeruginosa (highly resistant Gram-negative; wound, respiratory, urinary infections in immunocompromised patients) — MICs 2.0-8.0 mg/mL; also notable for biofilm-disrupting activity
- Klebsiella pneumoniae (pneumonia, urinary tract infections, nosocomial infections)
- Salmonella typhimurium, Shigella dysenteriae (gastroenteritis, dysentery)
- Helicobacter pylori (gastric ulcer, gastric cancer association) — activity at clinically relevant concentrations
- Vibrio cholerae (cholera) — activity demonstrated in vitro
Oral and dental pathogens:
- Porphyromonas gingivalis (chronic adult periodontitis)
- Aggregatibacter actinomycetemcomitans (aggressive periodontitis)
- Fusobacterium nucleatum (periodontal disease bridging organism)
- Treponema denticola (periodontal "red complex" member)
- Streptococcus sanguinis, Streptococcus mitis (dental plaque early colonizers)
For more detail on oral pathogen activity, see the Oral Health page.
Activity Against MRSA and Resistant Pathogens
The activity of myrrh against multi-drug-resistant pathogens is one of its most clinically interesting properties. The major mechanisms of bacterial antibiotic resistance — beta-lactamase enzymes (inactivating beta-lactam antibiotics), efflux pumps (extruding antibiotics from the cell), target-site mutations (preventing antibiotic binding), and ribosomal protection proteins — do not generally provide protection against the membrane-disruption mechanism that drives myrrh's antibacterial action. As a result, antibiotic-resistant strains do not show meaningful cross-resistance to myrrh sesquiterpenes.
Documented activity against resistant pathogens includes:
- Methicillin-resistant Staphylococcus aureus (MRSA) — the most extensively studied resistant target. Multiple studies have shown that myrrh essential oil and resin extracts retain antibacterial activity against MRSA at concentrations similar to those effective against methicillin-susceptible S. aureus (MSSA). MICs of 0.25 mg/mL or lower have been reported. The clinical implication: topical myrrh preparations may be useful as an adjunct in management of MRSA skin and soft tissue infections, though formal clinical trials in this setting are limited.
- Vancomycin-resistant Enterococcus (VRE) — activity retained against VRE strains, important for the management of nosocomial infections in patients with vancomycin-resistant gut colonization.
- Extended-spectrum beta-lactamase (ESBL)-producing E. coli and Klebsiella — the ESBL enzymes hydrolyze cephalosporins and most penicillins, but do not affect myrrh sesquiterpenes. Myrrh retains activity against ESBL-producing strains.
- Multi-drug-resistant Pseudomonas aeruginosa — reduced but retained susceptibility; the additional biofilm-disrupting effect is particularly relevant against this organism.
An additional important finding is the synergy between myrrh and conventional antibiotics. Subinhibitory concentrations of myrrh essential oil significantly enhance the activity of gentamicin, ciprofloxacin, and tetracycline against resistant strains of S. aureus and E. coli. The mechanism: myrrh's membrane-disrupting activity increases bacterial membrane permeability, thereby enhancing intracellular accumulation of co-administered antibiotics. This makes myrrh potentially useful as an antibiotic adjuvant in management of resistant infections, restoring efficacy of drugs that bacteria have developed resistance to.
The clinical adoption of myrrh-antibiotic combinations remains limited — formal clinical trials of this combination approach are scarce — but the laboratory data are consistent and biologically plausible. For more on S. aureus infections including MRSA, see our Staphylococcus aureus page.
Gram-Negative Activity (E. coli, Pseudomonas, Helicobacter)
Gram-negative bacteria are generally less susceptible to myrrh than Gram-positive bacteria, due to the additional outer membrane barrier in Gram-negative organisms. The outer membrane contains lipopolysaccharide (LPS) and porin channels, and it presents a hydrophilic barrier that limits the entry of lipophilic sesquiterpenes. Nonetheless, myrrh retains clinically relevant activity against several important Gram-negative pathogens.
E. coli is susceptible at MICs typically 1.0-4.0 mg/mL, with particular efficacy against enterotoxigenic and enteropathogenic strains that cause diarrheal disease. Traditional use of myrrh for "intestinal complaints" likely included treatment of bacterial gastroenteritis, and the modern microbiological evidence supports this traditional indication.
Pseudomonas aeruginosa is one of the more challenging targets for any antimicrobial agent. Its intrinsic outer membrane permeability is low, it has multiple efflux pump systems, it forms tenacious biofilms (particularly in chronic wound infections, cystic fibrosis lung disease, and indwelling catheter infections), and it has substantial capacity to acquire additional resistance determinants. Myrrh shows moderate direct bactericidal activity against P. aeruginosa (MIC 2.0-8.0 mg/mL), but its anti-biofilm activity is particularly relevant. Studies have demonstrated that myrrh extracts can reduce P. aeruginosa biofilm biomass by 40-60% at sub-inhibitory concentrations, which is potentially more clinically important than the direct bactericidal effect for biofilm-associated infections.
Helicobacter pylori is the Gram-negative microaerophilic bacterium responsible for most cases of peptic ulcer disease and a recognized class I carcinogen for gastric cancer. Conventional treatment uses combination antibiotic therapy with proton pump inhibitor, but increasing antibiotic resistance has reduced eradication rates significantly. Myrrh extracts have demonstrated in vitro activity against H. pylori, and the additional gastroprotective effects of myrrh (stimulation of mucus secretion, mild inhibition of gastric acid production) may provide complementary benefits in H. pylori-related gastric disease. Clinical trials of myrrh as part of H. pylori treatment are limited but the mechanistic rationale supports further investigation.
Salmonella and Shigella species, causing bacterial gastroenteritis and dysentery, are susceptible to myrrh at clinically relevant concentrations. Traditional use of myrrh for "bloody flux" (the historical term for dysentery) is well-documented in Greco-Roman and medieval European medical texts.
Antifungal Activity
Myrrh demonstrates significant antifungal properties against multiple pathogenic fungi. The Mahboubi and Kashani 2016 study in Pharmaceutical Biology systematically evaluated the anti-dermatophyte activity of Commiphora molmol and reported significant inhibition of Trichophyton rubrum (the most common cause of athlete's foot and onychomycosis), Trichophyton mentagrophytes, Microsporum canis, and Epidermophyton floccosum.
Documented antifungal activity:
- Candida albicans — the most common cause of fungal infections in humans (oral thrush, vaginal candidiasis, diaper rash, invasive candidiasis in immunocompromised patients). Myrrh inhibits C. albicans at concentrations achievable in topical and mucosal applications. The activity extends to Candida glabrata and other non-albicans species.
- Aspergillus niger — environmental mold that can cause invasive aspergillosis in severely immunocompromised patients; susceptible to myrrh in vitro.
- Dermatophyte fungi — Trichophyton, Microsporum, and Epidermophyton species causing tinea (ringworm) infections of skin, hair, and nails. Topical myrrh preparations have demonstrated efficacy against these pathogens.
- Cryptococcus neoformans — encapsulated yeast causing meningitis in immunocompromised patients (particularly advanced HIV/AIDS). In vitro activity demonstrated; clinical translation limited.
- Pityrosporum (Malassezia) species — lipophilic yeasts implicated in seborrheic dermatitis and pityriasis versicolor; some evidence of myrrh activity.
The mechanism of antifungal action parallels the antibacterial mechanism: lipophilic sesquiterpenes integrate into the fungal cell membrane and disrupt its integrity. Fungal membranes contain ergosterol rather than the cholesterol found in mammalian membranes, and the interaction of myrrh sesquiterpenes with ergosterol may provide some selectivity for fungal over mammalian membrane disruption. The antifungal activity is generally additive with conventional antifungal drugs (azoles, polyenes), suggesting potential combination therapy applications.
Practical antifungal applications of myrrh focus on topical use for superficial fungal infections: athlete's foot (tinea pedis), jock itch (tinea cruris), ringworm (tinea corporis), nail fungus (onychomycosis — though efficacy is limited by poor nail penetration), and Candida-related diaper rash or intertriginous infections. The typical preparation is myrrh essential oil diluted to 2-5% in carrier oil, applied to the affected area twice daily. For nail fungus specifically, a higher concentration (10% myrrh in jojoba oil) applied directly to the affected nail twice daily can produce gradual improvement, though complete cure of established onychomycosis typically requires prolonged treatment. For more on fungal infections, see our Fungal Infections page.
Activity Against Intestinal Protozoa
Beyond the helminth (worm) activity that underlies Mirazid's schistosomiasis and fascioliasis indications, myrrh has activity against several important intestinal protozoa:
- Giardia lamblia (giardiasis) — the most common cause of waterborne diarrheal illness in developed countries, causing chronic diarrhea, bloating, malabsorption, and weight loss. Myrrh extracts inhibit Giardia trophozoites in vitro, and traditional use of myrrh for chronic diarrheal illness in endemic areas likely covered giardiasis among other causes.
- Entamoeba histolytica (amoebiasis) — the cause of amoebic dysentery, with potential progression to invasive amoebic liver abscess. Myrrh shows activity against the trophozoite stage and may help reduce cyst shedding during chronic carriage.
- Cryptosporidium parvum — the cause of waterborne cryptosporidiosis, particularly problematic in immunocompromised patients (advanced HIV) and in childcare and water-supply outbreaks. Conventional treatment options for cryptosporidiosis are limited; myrrh's in vitro activity provides a potential adjunct.
- Trichomonas vaginalis — the cause of trichomoniasis, a sexually transmitted protozoal infection. Some evidence of myrrh activity in vitro.
- Leishmania species — the cause of leishmaniasis (cutaneous and visceral forms), endemic in many tropical and subtropical regions. Preliminary evidence of myrrh activity against the promastigote stage.
The antiprotozoal mechanism appears to involve disruption of the protozoal cell membrane through the same lipophilic-sesquiterpene mechanism that drives antibacterial activity, combined with interference with energy metabolism in the protozoal mitochondria-equivalent structures (kinetoplast in trypanosomatids, hydrogenosomes in Trichomonas).
Clinical applications of myrrh against intestinal protozoa remain primarily traditional and supportive rather than evidence-based first-line therapy. For confirmed giardiasis, amoebiasis, or cryptosporidiosis, conventional pharmaceutical therapy (metronidazole or tinidazole for giardiasis and amoebiasis; nitazoxanide for cryptosporidiosis) remains the standard of care. Myrrh may have a role as a supplementary agent or in resource-limited settings where conventional therapy is unavailable.
Traditional Anthelmintic Use
Beyond the well-documented schistosomiasis and fascioliasis indications that led to Mirazid's regulatory approval, traditional African and Arabian medicine has long used myrrh as a general anthelmintic for intestinal worm infestations. The traditional preparations and indications:
- Roundworms (Ascaris lumbricoides, soil-transmitted helminths) — the most common intestinal worm infection globally, affecting over 800 million people. Traditional Arabian preparations include myrrh resin dissolved in warm milk taken on an empty stomach in the morning, with a laxative follow-up several hours later. Conventional treatment uses albendazole or mebendazole, which are safer and more effective.
- Hookworm (Ancylostoma duodenale, Necator americanus) — soil-transmitted blood-feeding nematodes causing iron-deficiency anemia. Traditional myrrh use for "anemic weakness" overlapped with what would now be diagnosed as hookworm-associated anemia.
- Pinworm (Enterobius vermicularis) — the most common pediatric intestinal worm in developed countries, causing perianal itching especially at night. Traditional use of myrrh preparations is documented but conventional treatment (mebendazole, pyrantel) is more effective.
- Tapeworm (Taenia species, Hymenolepis nana) — intestinal cestodes acquired from undercooked beef, pork, or fish, or by direct fecal-oral spread (H. nana). Traditional preparations of myrrh combined with pomegranate bark and other anthelmintic herbs have been used historically; conventional treatment uses praziquantel or niclosamide.
The traditional anthelmintic mechanism likely involves the same tegument-disrupting activity that gives myrrh activity against Schistosoma and Fasciola: the sesquiterpenes disrupt the syncytial outer covering of worms, exposing them to digestive enzymes and immune attack and impairing their ability to maintain physiological homeostasis. Modern clinical trials of myrrh against the soil-transmitted helminths are limited; conventional anthelmintic drugs (albendazole, mebendazole, praziquantel) are inexpensive, safe, and highly effective and have largely displaced traditional preparations in modern parasitology practice.
The relevance of traditional anthelmintic use today is primarily historical and as context for understanding the broader antimicrobial spectrum of myrrh. For active worm infestation, conventional anthelmintic drugs prescribed by a physician are the appropriate treatment. For more on intestinal parasites, see our Parasites page.
Mechanism — Membrane Disruption + Biofilm Inhibition
The unifying mechanism behind myrrh's broad-spectrum antimicrobial activity is membrane disruption by lipophilic sesquiterpenes, supplemented by anti-biofilm activity that is particularly clinically important in chronic infections.
Membrane disruption: The principal sesquiterpenes (curzerene, furanoeudesma-1,3-diene, lindestrene) and the commiphoric acids are lipophilic small molecules that integrate into the phospholipid bilayer of microbial cell membranes. Once embedded in the membrane, they disrupt the ordered arrangement of fatty acid chains, increasing membrane fluidity and permeability. This leads to uncontrolled leakage of intracellular contents (potassium ions, ATP, nucleotides, proteins) and collapse of the transmembrane proton motive force, halting ATP synthesis and active transport. Electron microscopy studies confirm extensive membrane blebbing, pore formation, and eventual cell lysis in susceptible microbes.
Biofilm inhibition: Biofilms are structured microbial communities enclosed in self-produced extracellular polymeric substance (EPS) matrices, responsible for up to 80% of chronic bacterial infections. Bacteria within biofilms are 100-1000 times more resistant to conventional antibiotics than planktonic counterparts. Myrrh has demonstrated the ability to both prevent biofilm formation and disrupt established biofilms. Sesquiterpenes penetrate the EPS matrix and destabilize its structural integrity; commiphoric acids inhibit quorum-sensing signals that bacteria use to coordinate biofilm formation. Sub-inhibitory concentrations of myrrh extract can reduce biofilm formation by 50-70% in susceptible species. This is particularly relevant for chronic wound infections, chronic sinusitis, dental plaque, chronic Pseudomonas infections in cystic fibrosis, and indwelling catheter biofilm infections.
Anti-adhesion: Many pathogens initiate infection through adhesion to host cells via surface adhesins, fimbriae, and pili. Myrrh interferes with bacterial adhesion through modification of adhesin gene expression and direct surface coating effects that block bacterial attachment. This anti-adhesion mechanism is particularly relevant for oral pathogens (interfering with dental plaque attachment) and uropathogens (interfering with E. coli attachment to bladder epithelium).
Oxidative damage: Certain myrrh compounds, particularly furanosesquiterpenes, generate reactive oxygen species within microbial cells, causing oxidative damage to DNA, proteins, and lipids. The oxidative stress overwhelms microbial antioxidant defense systems (superoxide dismutase, catalase), leading to irreversible cellular damage. Myrrh extracts have been shown to increase intracellular ROS levels 3-5 fold within the first hour of exposure in susceptible bacteria.
The combination of these mechanisms produces a multi-target antimicrobial effect that makes the development of bacterial resistance considerably more difficult than with single-target conventional antibiotics. This is one of myrrh's most attractive features as a potential antimicrobial adjunct in the era of escalating antibiotic resistance.
Cautions
- Pregnancy is an absolute contraindication. Myrrh's uterine-stimulant activity makes any significant exposure inadvisable during pregnancy. The Mirazid pharmaceutical preparation is specifically contraindicated in pregnancy in the Egyptian Ministry of Health labeling.
- Diagnostic confirmation — for any suspected parasitic infection, formal diagnostic confirmation (stool examination, serology, imaging as appropriate) should precede treatment. Self-diagnosis and self-treatment of parasitic infections is generally unwise, and effective conventional antiparasitic drugs (praziquantel, triclabendazole, albendazole, metronidazole) are widely available and well-tolerated.
- Schistosomiasis-specific concerns — if Mirazid is used for schistosomiasis, follow-up stool examination at 3 and 6 months post-treatment is essential to confirm cure. Given the efficacy debate discussed above, treatment failures should prompt second-line therapy with praziquantel rather than repeated myrrh courses.
- Anticoagulant therapy — myrrh's platelet-inhibitory activity can potentiate warfarin, heparin, aspirin, clopidogrel, and direct oral anticoagulants. The clinically relevant exposure is most likely with internal use (capsules, tincture); topical antimicrobial application produces minimal systemic exposure.
- Drug interactions — myrrh may affect cytochrome P450 enzyme activity and interact with drugs metabolized through these pathways. Patients on prescription medications should consult a pharmacist about potential interactions before significant internal myrrh use.
- Hypoglycemia — myrrh's blood-glucose-lowering effect can potentiate diabetes medications. Diabetic patients using myrrh should monitor blood glucose closely.
- Contact dermatitis — allergic contact reactions to topical myrrh, particularly undiluted essential oil, are uncommon but documented. Patch test before extensive topical use.
- Children — safety data for internal myrrh use in young children are limited; pediatric use should be under medical supervision.
- Antibiotic stewardship — myrrh's broad-spectrum antimicrobial activity does not eliminate the need for appropriate antibiotic stewardship. Serious bacterial infections require conventional antibiotic therapy based on culture and susceptibility data, not herbal substitutes. Myrrh's role is adjunctive and complementary, not primary.
Key Research Papers
- Sheir Z et al. (2001). A safe, effective herbal antischistosomal therapy derived from myrrh. American Journal of Tropical Medicine and Hygiene 65(6):700-704. — PubMed
- Massoud A et al. (2001). Preliminary study of therapeutic efficacy of a new fasciolicidal drug derived from Commiphora molmol (myrrh). — PubMed
- Botros S et al. (2005). Efficacy of mirazid in comparison with praziquantel in Egyptian Schistosoma mansoni-infected schoolchildren and households. American Journal of Tropical Medicine and Hygiene. — PubMed
- Rahman MM et al. (2008). Antibacterial terpenes from the oleo-resin of Commiphora molmol. Phytotherapy Research. — PubMed
- Mahboubi M, Kashani LM (2016). The anti-dermatophyte activity of Commiphora molmol. Pharmaceutical Biology. — PubMed
- de Rapper S, Van Vuuren SF et al. (2012). Additive and synergistic antimicrobial effects of select frankincense and myrrh oils. Letters in Applied Microbiology. — PubMed
- Tonkal AM, Morsy TA (2008). An update review on Commiphora molmol and related species. Journal of the Egyptian Society of Parasitology. — PubMed
- Omer SA, Adam SE, Mohammed OB (2011). Antimicrobial activity of Commiphora myrrha against some bacteria and Candida albicans. Research in Veterinary Science. — PubMed
- Shen T et al. (2012). The genus Commiphora: a review of its traditional uses, phytochemistry and pharmacology. Journal of Ethnopharmacology. — PubMed
- Noumi E et al. (2011). Chemical composition, antioxidant and antifungal potential of Commiphora myrrha essential oil. Asian Pacific Journal of Tropical Medicine. — PubMed
- Hanus LO et al. (2005). Myrrh — commiphora chemistry. Biomedical Papers. — PubMed
- Nomicos EY (2007). Myrrh: medical marvel or myth of the Magi? Holistic Nursing Practice. — PubMed
PubMed Topic Searches
- PubMed: Mirazid schistosomiasis
- PubMed: Mirazid fascioliasis
- PubMed: Myrrh and MRSA
- PubMed: Biofilm inhibition
- PubMed: H. pylori activity
- PubMed: Traditional anthelmintic use
Connections
- Myrrh Overview
- Myrrh Benefits Hub
- Myrrh for Wound Healing
- Myrrh for Oral Health
- Myrrh Anti-Inflammatory
- Boswellia (Frankincense)
- Goldenseal
- Manuka Honey
- Tea Tree
- Neem
- Garlic
- Parasites
- Staphylococcus aureus (MRSA)
- Fungal Infections
- Schistosomiasis — the fluke infection Mirazid was approved to treat.
- All Herbs