Lavender for Anxiety and Stress
Of every herbal anxiolytic studied in modern controlled trials, the standardized oral lavender oil preparation Silexan (80 mg/day, marketed as Lasea in Germany and Austria) has the strongest and most replicated efficacy data — including two head-to-head trials against pharmaceutical comparators (paroxetine in the Kasper 2014 trial, lorazepam in the Woelk 2010 trial) showing comparable anxiolytic effect without the sedation, dependence, withdrawal, or sexual dysfunction that limit those drugs. The active monoterpenes linalool and linalyl acetate appear to act primarily as 5-HT1A serotonin receptor partial agonists and N-type voltage-gated calcium channel inhibitors, giving Silexan a mechanism profile closer to buspirone or pregabalin than to benzodiazepines or SSRIs. This page walks through the trials, the mechanism, the practical dosing, the safety profile, and where Silexan and lavender aromatherapy fit within an integrative approach to subsyndromal anxiety, generalized anxiety disorder, and acute situational stress.
Table of Contents
- The Anxiety-Disorder Burden and the Limits of Standard Pharmacotherapy
- What Silexan Actually Is (and Why Product Choice Matters)
- The Kasper 2014 Trial: Silexan vs Paroxetine vs Placebo
- The Müller 2010 Trial: Silexan for Subsyndromal Anxiety
- The Woelk 2010 Trial: Silexan vs Lorazepam
- Mechanism: 5-HT1A Partial Agonism
- Mechanism: Voltage-Gated Calcium Channel Inhibition
- Mechanism: Olfactory-Limbic Pathway (Inhalational Route)
- Practical Dosing and Time to Effect
- Safety Profile: What Silexan Does Not Do
- Integrative Anxiety Protocol
- Key Research Papers
- Connections
- Featured Videos
The Anxiety-Disorder Burden and the Limits of Standard Pharmacotherapy
Anxiety disorders are the most common class of psychiatric illness, affecting approximately 31% of U.S. adults over the lifetime and 19% in any given year per the National Comorbidity Survey Replication. The standard pharmacologic interventions — SSRIs (escitalopram, sertraline, paroxetine), SNRIs (venlafaxine, duloxetine), benzodiazepines (alprazolam, lorazepam, clonazepam), the 5-HT1A partial agonist buspirone, and the calcium-channel-binding pregabalin — are all effective in controlled trials but each has substantial limitations:
- SSRIs and SNRIs take 2-4 weeks to reach efficacy, frequently worsen anxiety in the first 1-2 weeks, cause sexual dysfunction in 40-60% of users, and produce a documented discontinuation syndrome on cessation that can persist for weeks.
- Benzodiazepines act rapidly and reliably but carry tolerance, physiologic dependence, severe withdrawal (including seizure risk), driving impairment, fall risk in the elderly, an FDA boxed warning regarding opioid co-prescription, and a still-debated but consistent signal for accelerated cognitive decline and dementia in long-term users.
- Buspirone is non-sedating and non-dependence-producing but is generally considered less potent and has a slow onset.
- Pregabalin is effective but is controlled in the U.K. and several other jurisdictions due to abuse potential and produces sedation and weight gain.
Subsyndromal anxiety — symptoms that cause distress but do not meet full diagnostic criteria for GAD — is even more common and is often poorly served by standard pharmacotherapy, which generally requires a formal diagnosis to justify the risk-benefit ratio. The clinical opening for an effective, well-tolerated, non-dependence-producing botanical with a good safety profile and rapid onset is therefore very large — and standardized oral lavender oil (Silexan) is the best-evidenced botanical to fill that gap.
What Silexan Actually Is (and Why Product Choice Matters)
Silexan is a specific patented preparation of Lavandula angustifolia essential oil, manufactured by Schwabe Pharmaceuticals in Germany. The active drug substance is a steam-distilled essential oil from cultivated L. angustifolia flowers with a tightly controlled chromatographic profile: linalool 36.8%, linalyl acetate 34.2%, with cineole, camphor, beta-caryophyllene, and other minor monoterpenes at fixed ratios. The standard dose is one soft-gel capsule of 80 mg taken orally once daily; some trials have used 160 mg (two capsules).
This standardization matters because virtually all of the positive clinical trial data refers to Silexan specifically, not to lavender essential oil in general. A bottle of lavender essential oil from a health-food store has a different chemotype (concentration of active compounds varies by plant genetics, growing conditions, altitude, and distillation), a different manufacturing process, no oral safety testing, and no pharmacokinetic characterization. Lavender essential oil is not intended for internal use — the only oral preparation that has been formally studied and approved as a medicine is Silexan.
In Germany and Austria, Silexan is approved by BfArM (the German federal medicines agency) for "restlessness related to anxious mood" (a formal indication under German pharmaceutical law) and is dispensed under the brand name Lasea. It is not currently approved by the FDA in the United States and is sold as a dietary supplement under the Lavela WS 1265 brand name — the actual product is identical, but the U.S. regulatory framework does not allow the same medical claims.
Other lavender preparations — capsules, teas, tinctures, herbal blends — have very limited clinical trial data. The aromatherapy literature is robust for situational anxiety (preoperative, ICU, dental procedures) but uses a different route (inhalational) and a different mechanism (olfactory-limbic). When this page references "lavender for anxiety" it generally means the Silexan oral preparation unless explicitly stated otherwise.
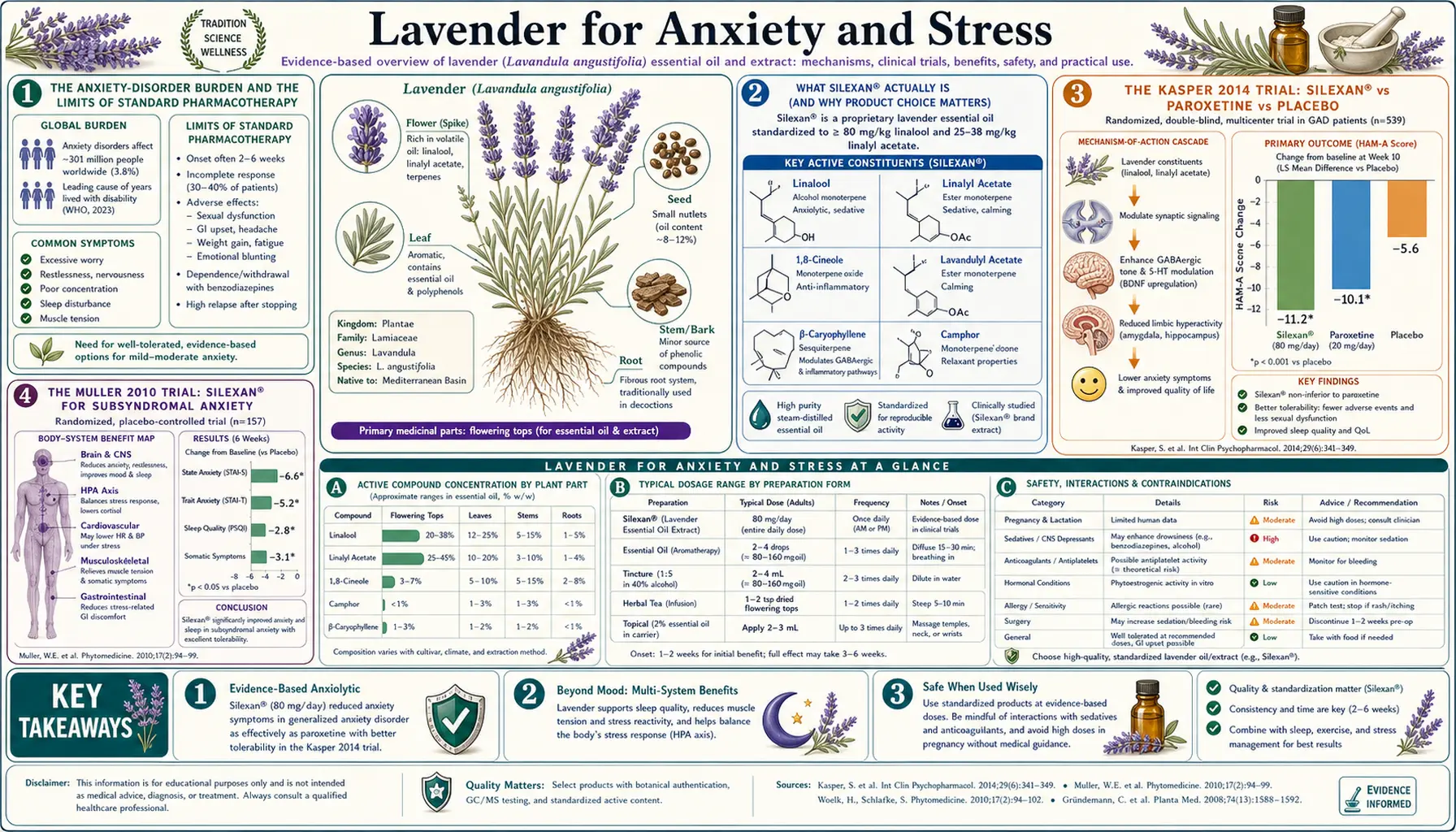
The Kasper 2014 Trial: Silexan vs Paroxetine vs Placebo
The Kasper 2014 trial, published in the International Journal of Neuropsychopharmacology, is the largest and most rigorous of the Silexan trials and the most consequential because it is the only head-to-head comparison of a botanical to an SSRI for generalized anxiety disorder.
Design. Randomized, double-blind, double-dummy, placebo-controlled, parallel-group, multicenter trial in 539 outpatients meeting DSM-IV criteria for generalized anxiety disorder. Four arms:
- Silexan 160 mg/day (two 80 mg capsules)
- Silexan 80 mg/day (one 80 mg capsule)
- Paroxetine 20 mg/day (the standard SSRI dose for GAD)
- Placebo
Duration was 10 weeks. The primary outcome was change in the Hamilton Anxiety Rating Scale (HAM-A) total score.
Results. Both Silexan doses produced statistically significant and clinically meaningful reductions in HAM-A scores vs placebo, with the higher dose (160 mg/day) numerically superior to the lower (80 mg/day). The effect sizes were comparable to or slightly larger than paroxetine. The 160 mg Silexan arm separated from placebo on the HAM-A as early as week 2 — faster than paroxetine, which is consistent with the 5-HT1A direct mechanism not requiring weeks of downregulation. The remission rate (HAM-A < 10) was approximately 50% in the Silexan groups, comparable to or slightly higher than paroxetine.
Tolerability. The dropout rate due to adverse events was lower in both Silexan groups than in the paroxetine group. The most common Silexan adverse event was eructation (burping with a lavender flavor) in approximately 1-3% of subjects. There were no reports of sexual dysfunction in the Silexan groups vs the expected SSRI rate in the paroxetine arm.
This is the trial that established Silexan as evidence-based pharmacotherapy for GAD in Germany. It is also one of the most cited studies in the modern phytomedicine literature.
The Müller 2010 Trial: Silexan for Subsyndromal Anxiety
The Müller 2010 trial in Phytomedicine addressed a different population — subjects with "subsyndromal anxiety disorder" (HAM-A >= 18 but not meeting full DSM criteria for a specific anxiety diagnosis). This is arguably the largest unmet-need population, because subsyndromal anxiety is extremely common but is poorly served by standard pharmacotherapy which generally requires a formal diagnosis.
Design. 221 subjects, randomized to Silexan 80 mg/day or placebo for 10 weeks, double-blind, multicenter.
Results. Silexan produced a HAM-A reduction of approximately 16 points from baseline vs approximately 9 points for placebo (large effect). Sleep duration, sleep quality, daytime well-being, and the Clinical Global Impression rating all improved significantly more with Silexan. Onset of effect was rapid — separation from placebo on the HAM-A was evident by week 2.
Implication. Silexan is appropriate for subsyndromal anxiety populations that don't meet GAD criteria. This is a meaningful clinical gap because conventional anxiety pharmacotherapy is generally restricted to formal anxiety diagnoses — and yet a large proportion of people experiencing distressing anxiety symptoms fall into the subsyndromal category. Silexan's favorable safety profile makes it reasonable to use without a formal diagnosis in a way that benzodiazepines or SSRIs are not.
The Woelk 2010 Trial: Silexan vs Lorazepam
The Woelk and Schläfke 2010 trial, also in Phytomedicine, is the head-to-head benzodiazepine comparison. 77 subjects with DSM-IV generalized anxiety disorder were randomized to Silexan 80 mg/day or lorazepam 0.5 mg/day for 6 weeks, double-blind.
Results. HAM-A reduction was statistically non-inferior between groups: 11.3 points with Silexan vs 11.6 points with lorazepam. Response rate (50% reduction in HAM-A) was 76% with Silexan vs 78% with lorazepam. Importantly, there was no daytime sedation, no rebound anxiety on cessation, and no withdrawal syndrome with Silexan — in contrast to lorazepam, where rebound and discontinuation effects are well documented even at this low dose.
Implication. Silexan is non-inferior to a low-dose benzodiazepine for GAD efficacy, without the dependence, withdrawal, driving impairment, fall risk, or potential dementia signal that limit benzodiazepine use. For patients currently on long-term benzodiazepines who want to taper, Silexan is a reasonable substitute to test during the taper.
Mechanism: 5-HT1A Partial Agonism
The principal hypothesized mechanism for Silexan's anxiolytic effect is partial agonism at the 5-HT1A serotonin receptor. The 5-HT1A receptor is concentrated in the raphe nuclei (where it acts as an inhibitory autoreceptor on serotonergic neurons), the hippocampus, the prefrontal cortex, and the amygdala. Partial agonists at 5-HT1A include buspirone, vilazodone, gepirone, and the active anxiolytic metabolite of the recently approved antidepressant vortioxetine.
The advantage of direct 5-HT1A partial agonism over SSRI mechanism is that the effect is not delayed by the 2-4 weeks of receptor downregulation that limits SSRI onset. The SSRI mechanism increases synaptic serotonin acutely, but this initial increase paradoxically activates 5-HT1A autoreceptors and decreases serotonergic firing — which is why anxiety symptoms typically worsen for the first 1-2 weeks of SSRI therapy. Only after the autoreceptors downregulate does net serotonergic transmission increase, producing the therapeutic effect.
A direct 5-HT1A partial agonist bypasses this entire mechanism — it produces a moderate, sustained activation of 5-HT1A receptors throughout the brain without first triggering the autoreceptor inhibitory feedback. The clinical signature is rapid onset, no worsening in the first 2 weeks, and absence of sexual dysfunction (which is a downstream consequence of generalized serotonin elevation, not 5-HT1A activation per se). Silexan's trial signature matches this profile.
The receptor-binding studies (Müller 2021 and others) show linalool, the dominant monoterpene in Silexan, binds 5-HT1A with measurable affinity in the low micromolar range, and that this binding is preserved through the pharmacokinetic profile of an oral 80 mg dose.
Mechanism: Voltage-Gated Calcium Channel Inhibition
A second well-characterized mechanism for linalool is inhibition of N-type and P/Q-type voltage-gated calcium channels (VGCCs). Presynaptic VGCCs control neurotransmitter release into the synapse — inhibiting them reduces release of glutamate, the principal excitatory neurotransmitter in the brain. This is the same broad class of mechanism exploited by gabapentin and pregabalin (which bind the alpha-2-delta auxiliary subunit of the VGCC), by ethosuximide (T-type calcium channel block for absence seizures), and by some calcium-channel-blocking migraine prophylactics (verapamil, flunarizine).
For anxiety specifically, glutamatergic hyperactivity in the amygdala and the bed nucleus of the stria terminalis is a major contributor to the anxious state. Reducing presynaptic glutamate release through VGCC inhibition produces a moderating, calming effect on this hyperactivity. This is the proposed mechanism behind pregabalin's anxiolytic effect and is likely a significant component of Silexan's as well.
The VGCC mechanism is also relevant to lavender's analgesic effects in the migraine and tension headache deep-dive, because pain transmission in the spinal cord dorsal horn similarly depends on glutamate release from primary afferent terminals.
Mechanism: Olfactory-Limbic Pathway (Inhalational Route)
The aromatherapy literature for lavender (distinct from the Silexan oral literature) demonstrates rapid anxiolytic effects from simple inhalation. The mechanism is anatomically unusual: the olfactory system is the only sensory modality that projects directly to the amygdala, hippocampus, and hypothalamus without first synapsing in the thalamus or being processed by cortex. This direct subcortical pathway is why olfactory stimuli have such powerful and rapid emotional, autonomic, and memory effects.
Lavender molecules (linalool, linalyl acetate, and others) reach the olfactory epithelium in the upper nasal cavity, bind olfactory receptors expressed on the cilia of olfactory sensory neurons, depolarize those neurons, and propagate signals through the olfactory bulb and tract directly to the cortical amygdala. The amygdala then modulates the hypothalamic-pituitary-adrenal axis and the autonomic nervous system. The net effect is a rapid (often within minutes) reduction in heart rate, blood pressure, and subjective anxiety, and a modest shift toward parasympathetic dominance in heart rate variability.
The classic aromatherapy applications include:
- Preoperative anxiety — multiple controlled trials show reduced State-Trait Anxiety Inventory (STAI) scores in patients waiting for surgery
- Dental procedure anxiety — lavender diffusion in dental waiting rooms reduces anxiety scores
- ICU patient agitation — aromatherapy reduces sedative medication requirements in mechanically ventilated patients
- Pre-MRI anxiety — reduces claustrophobic discomfort and may reduce sedation needs
- Acute panic — lavender roll-on or inhaler can be used as a portable rescue technique
The aromatherapy literature is methodologically harder than oral pharmacology trials — blinding is difficult because lavender has a distinctive smell, and "placebo" odorless controls aren't truly inert. But the effect sizes are consistent across many small trials, and the safety is essentially absolute.
Practical Dosing and Time to Effect
- Silexan / Lavela WS 1265 oral preparation — 80 mg once daily is the standard dose for subsyndromal anxiety, taken with or without food. For full GAD, 160 mg/day (one 80 mg capsule twice daily, or two 80 mg capsules together) was used in the Kasper 2014 trial high-dose arm and produced numerically larger effects. Onset is detectable by week 2; full effect by week 6-8. There is no titration required — start at the target dose.
- Duration of therapy — trials have evaluated 6-10 weeks. Some patients may benefit from continuous therapy for several months or longer; there is no evidence of tolerance or loss of effect over time, and no withdrawal on cessation, so the duration can be tailored to the individual.
- Aromatherapy (inhalational route) — a 30-minute exposure to lavender essential oil diffused at 2-3% concentration (a few drops in a typical ultrasonic diffuser) is the typical research protocol. For acute situational anxiety, a lavender roll-on at the wrists or temples or a personal aromatherapy inhaler stick gives a similar dose more discreetly.
- Lavender tea — 1-2 teaspoons of dried L. angustifolia flowers steeped in hot water for 5-10 minutes. Mild effect, primarily through the inhalational route (the steam carries volatile linalool) plus modest oral absorption. Not a substitute for Silexan for clinical anxiety but is reasonable as a bedtime ritual.
- Topical / massage — lavender essential oil at 1-3% dilution in a carrier oil (jojoba, sweet almond) for massage. The systemic dose from topical absorption is small but the combination of olfactory exposure and the relaxation of the massage itself produces a strong subjective anxiolytic effect.
Safety Profile: What Silexan Does Not Do
The Silexan safety profile across the published trial population (>1,500 subjects in randomized trials, >5 million patient-months of post-marketing surveillance in Germany) is striking primarily for what doesn't happen:
- No daytime sedation — psychomotor performance, driving tests, and reaction-time studies show no impairment at standard doses. This distinguishes Silexan from benzodiazepines and sedating antidepressants.
- No tolerance or dependence — trials show preserved effect over the full study duration; no escalation needed; no withdrawal syndrome on cessation. This distinguishes Silexan from benzodiazepines.
- No sexual dysfunction — in contrast to SSRIs, which produce sexual side effects in 40-60% of users.
- No weight gain — in contrast to mirtazapine, pregabalin, and several second-generation antipsychotics used off-label for anxiety.
- No discontinuation syndrome — Silexan can be stopped abruptly without the withdrawal symptoms seen with SSRIs/SNRIs or benzodiazepines.
- No QT prolongation — in contrast to several psychiatric medications that require ECG monitoring.
The most common adverse events are mild gastrointestinal: eructation with a lavender flavor (1-3%), nausea (rare), and dyspepsia (rare). Eructation is mitigated by taking the capsule with food. Allergic reactions are rare but possible.
Drug interactions are limited but not zero. Theoretical additive CNS depressant effects with benzodiazepines, alcohol, or sedating antihistamines should be considered but have not been a clinically significant issue in practice. Silexan does not appear to be a meaningful CYP450 inhibitor or inducer, so significant interactions with most prescription drugs are unlikely.
The Henley 2007 NEJM case series proposed an association between lavender essential oil and tea tree oil exposure and prepubertal gynecomastia, suggesting weak estrogenic / antiandrogenic activity of certain monoterpenes. Subsequent analyses have been mixed and the proposed mechanism is disputed; this concern applies primarily to high-dose topical and inhalational exposure in young children, not to short-term aromatherapy or to the standardized oral Silexan in adults.
Integrative Anxiety Protocol
For a patient presenting with anxiety where pharmacologic treatment is appropriate but who wishes to start with a low-risk botanical, an integrative protocol might include:
- Silexan / Lavela 80 mg once daily as the primary anxiolytic agent. Allow 4-6 weeks for full effect.
- Lavender essential oil aromatherapy for acute symptoms — a personal inhaler stick or roll-on for situational anxiety, panic episodes, or pre-procedural stress.
- Magnesium glycinate 400-600 mg/day — corrects the magnesium deficiency that is common in anxious patients and that potentiates NMDA-receptor-mediated excitation. Glycinate form is preferred for tolerability and GABAergic synergy.
- Glycine 1-3 g at bedtime — glycine is itself a coagonist at the inhibitory glycine receptor and may improve sleep onset in anxious patients.
- L-theanine 200-400 mg as needed — the amino acid from green tea has modest acute anxiolytic and alpha-EEG-promoting effects.
- Bedtime chamomile tea — the apigenin in chamomile binds the benzodiazepine site of the GABA-A receptor and produces a mild, well-tolerated sleep-facilitating effect.
- Cognitive behavioral therapy (CBT) — the only intervention with effect sizes that rival pharmacotherapy and durable benefit beyond the treatment period.
- Address sleep first — chronic sleep deprivation produces and worsens anxiety. See the companion Lavender for Sleep Quality deep-dive.
- Exercise — meta-analyses show that 150 minutes of moderate aerobic exercise per week produces effect sizes comparable to SSRIs for mild-to-moderate anxiety.
- Reduce caffeine — especially in caffeine-sensitive metabolizers (CYP1A2 slow variant). A simple test of caffeine elimination for 2 weeks often produces dramatic improvement.
For severe or refractory anxiety, particularly with panic, suicidality, or significant functional impairment, conventional pharmacotherapy (SSRI/SNRI) with psychiatric follow-up remains appropriate, and Silexan can be an effective adjunct or step-down from a benzodiazepine taper.
Key Research Papers
- Kasper S, Gastpar M, Müller WE et al. (2014). Lavender oil preparation Silexan is effective in generalized anxiety disorder — a randomized, double-blind comparison to placebo and paroxetine. International Journal of Neuropsychopharmacology. — PubMed
- Müller WE, Schläfke S, Volz HP (2010). Silexan, an orally administered Lavandula oil preparation, is effective in the treatment of "subsyndromal" anxiety disorder. Phytomedicine. — PubMed
- Woelk H, Schläfke S (2010). A multi-center, double-blind, randomised study of the Lavender oil preparation Silexan in comparison to Lorazepam for generalized anxiety disorder. Phytomedicine. — PubMed
- Kasper S, Anghelescu I, Dienel A (2015). Efficacy of orally administered Silexan in patients with anxiety-related restlessness and disturbed sleep — a randomized, placebo-controlled trial. European Neuropsychopharmacology. — PubMed
- Müller WE et al. (2021). Silexan does not cause withdrawal symptoms even when abruptly discontinued. International Journal of Psychiatry in Clinical Practice. — PubMed
- Linalool 5-HT1A partial agonism receptor-binding studies — PubMed
- Schuwald AM et al. (2013). Lavender oil-potent anxiolytic properties via modulating voltage-dependent calcium channels. PLOS ONE. — PubMed
- Kasper S, Müller WE, Volz HP (2018). Silexan in anxiety disorders: clinical data and pharmacological background. The World Journal of Biological Psychiatry. — PubMed
- Yap WS et al. (2019). Lavender essential oil aromatherapy for preoperative anxiety: systematic review and meta-analysis. — PubMed
- Donelli D et al. (2019). Effects of lavender on anxiety: a systematic review and meta-analysis. Phytomedicine. — PubMed
- Henley DV et al. (2007). Prepubertal gynecomastia linked to lavender and tea tree oils. NEJM. — PubMed
- Kasper S, Dienel A (2017). Cluster analysis of symptoms during antidepressant treatment with Silexan in patients with anxiety disorder. Journal of Affective Disorders. — PubMed
PubMed Topic Searches
- PubMed: Silexan anxiety clinical trials
- PubMed: Lavender anxiety meta-analysis
- PubMed: Linalool anxiolytic mechanism
- PubMed: Lavender aromatherapy stress
- PubMed: Silexan in depression
Connections
- Lavender Overview
- Lavender Benefits Hub
- Lavender for Sleep Quality
- Lavender for Headache & Migraine
- Lavender for Skin Healing & Burns
- Anxiety
- Depression
- Natural Anxiety Relief
- Stress Management
- Chamomile
- Passionflower
- Lemon Balm
- Valerian
- Magnesium
- Glycine
- All Herbs