Echinacea: History and Traditional Use
Echinacea — the purple coneflower — is one of the very few famous Western herbs that is genuinely native to North America, and almost everything the modern world knows about it traces back to the Indigenous peoples of the Great Plains, who used it as medicine long before Europeans arrived. Its written history is short by the standards of an Old World herb like mullein or garlic, but it is unusually well documented: a single ethnobotanist's 1919 field report, a German immigrant's patent tonic, and two famous Cincinnati pharmacists carried this prairie flower from the medicine bundles of the Plains nations into the American drugstore, across the Atlantic to Germany, and into the laboratory. This page tells that story plainly, marks tradition as tradition, and is honest about where the documentary record is thin.
Table of Contents
- A Native North American Plant and Its Name
- Medicine of the Plains Nations
- Gilmore and the Ethnobotanical Record
- H.C.F. Meyer and the Blood Purifier
- The Eclectic Physicians: Lloyd and King
- Decline in America, Rebirth in Germany
- Why Three Species, and Why It Matters
- From Tradition to Modern Research
- Research Papers and References
- Connections
- Featured Videos
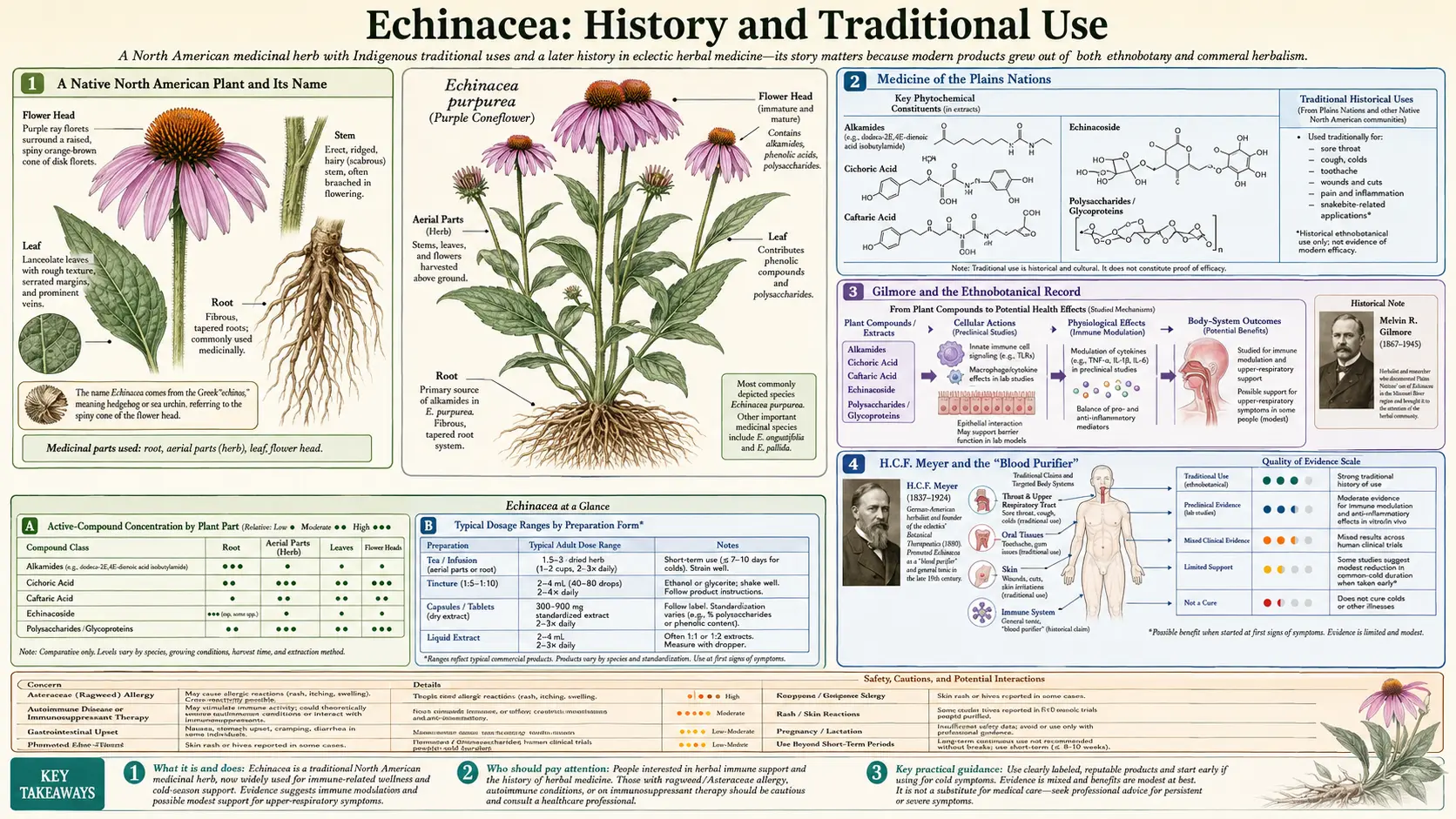
A Native North American Plant and Its Name
Unlike most of the herbs in the Western cabinet, Echinacea did not arrive in America from Europe or Asia — it has always grown here. The genus Echinacea belongs to the daisy family (Asteraceae) and comprises roughly ten species of coneflower, all of them native only to central and eastern North America, with the greatest diversity across the prairies and open woodlands of the United States. The three species that became medicines — Echinacea purpurea, Echinacea angustifolia, and Echinacea pallida — are plants of the Great Plains and the eastern grasslands, the country of the very nations who first used them.
The botanical name records a small piece of European scientific history. In 1753 Carl Linnaeus, the founder of modern biological naming, catalogued the purple coneflower in his Species Plantarum but placed it in the genus Rudbeckia, as Rudbeckia purpurea. In 1794 the German botanist Conrad Moench separated it into a new genus of its own, Echinacea, in his work Methodus Plantas Horti Botanici et Agri Marburgensis. The name is descriptive and rather charming: it comes from the Greek echinos, meaning hedgehog or sea-urchin, a nod to the stiff, spiny central cone of the seed-head that pricks the hand like a tiny hedgehog. These are named here as the historical naming events; the modern authority for the species is written Echinacea purpurea (L.) Moench, preserving both Linnaeus and Moench in the citation.
It is worth being clear at the outset about a fact that shapes the whole rest of this story: a plant native only to North America has no ancient Greek, Roman, medieval European, or classical Eastern medical record. There is no Dioscorides for Echinacea and no entry in the old Chinese or Ayurvedic materia medica, because the plant simply did not grow on those continents until gardeners and drug companies carried it there in the modern era. Everything genuinely old in Echinacea's human story is Native American.
Medicine of the Plains Nations
Echinacea was, by a wide margin, the most important medicinal plant of the Native peoples of the Great Plains, and a substantial ethnobotanical record documents its use across many nations. The species most often used was Echinacea angustifolia, the narrow-leaved coneflower of the dry prairie, whose root carries the characteristic tongue-tingling, saliva-provoking, slightly numbing taste that became the plant's signature. That tingling sensation — produced by the root's alkamides — was itself part of how the plant was understood and used, particularly for complaints of the mouth and throat.
The documented Indigenous uses cluster around infection, pain, and the mouth and throat. Tribes including the Lakota (Sioux), Cheyenne, Comanche, Pawnee, Kiowa, Omaha-Ponca, Dakota, and others are recorded as using Echinacea root for a remarkable range of ailments: chewed or held in the mouth for toothache and sore throat; applied as a poultice or wash to wounds, burns, insect bites, and the bites of venomous snakes; taken for coughs, colds, and other infections; and used as a general pain reliever. The Kiowa are documented using it for coughs and sore throats, the Cheyenne for sore mouth and throat, the Pawnee for headaches, and the Lakota among the nations who used it as a pain medication and a remedy for snakebite. The fresh root's numbing quality made it a natural choice for the pain of toothache and for the mouth.
Several nations also held the plant in ceremonial and protective regard, and it appears in connection with practices such as the handling of heat in certain rituals; readers should treat these as documented cultural practices belonging to those nations rather than as health recommendations. What stands out historically is the sheer breadth of use: independent Plains nations, working within their own distinct medical systems, converged on this single prairie root as a first-line remedy for infection and pain. That convergence is the foundation of Echinacea's entire later reputation.
Gilmore and the Ethnobotanical Record
Much of what is reliably known about traditional Plains use of Echinacea was gathered and published by one careful observer: the ethnobotanist Melvin R. Gilmore, who recorded the plant lore of the nations of the Missouri River region in the early twentieth century. His landmark study, Uses of Plants by the Indians of the Missouri River Region, was issued in 1919 (in the Thirty-third Annual Report of the Bureau of American Ethnology) and grew out of fieldwork and a doctoral dissertation completed a few years earlier. Gilmore's report is the single most-cited primary source for Native American Echinacea use, and it is named here as that historical source.
Gilmore did not understate the plant's importance. In a sentence that has been quoted in nearly every history written since, he observed that "Echinacea seems to have been used as a remedy for more ailments than any other plant." That judgment — that of all the prairie medicines he catalogued, the coneflower was the most versatile and most relied-upon — is the closest thing Echinacea has to a founding statement, and it comes not from a folklore retelling but from a trained ethnographer recording living practice directly from the people who held it.
The archaeological record gives the tradition real depth in time. Roots identified as purple coneflower were recovered from a Pawnee earth-lodge village in Nebraska associated with around the year 1800, and were identified as Echinacea by Gilmore's era of ethnobotanical work. Reviews of the literature count on the order of nineteen different tribes with documented Echinacea use. The honest summary is this: Echinacea's deep history is Native American, it is genuinely old, and it is unusually well attested for a North American herb — thanks in large part to one diligent fieldworker.
H.C.F. Meyer and the Blood Purifier
Echinacea crossed from Indigenous medicine into the American commercial and professional world through an unlikely figure: H.C.F. Meyer, a German-born lay practitioner living in Nebraska in the second half of the nineteenth century, who is commonly said to have learned of the plant's uses from Native Americans of the region. In the 1870s and 1880s Meyer formulated a patent tonic built around Echinacea, which he marketed as Meyer's Blood Purifier and promoted, in the exuberant style of the era's patent medicines, for ailments ranging from rheumatism and neuralgia to the bite of the rattlesnake. Meyer was, by the standards of trained physicians of his day, very much an outsider — an enthusiastic promoter rather than a researcher — and the more extravagant snakebite-cure claims he attached to his tonic belong firmly to patent-medicine salesmanship rather than to verified fact.
Meyer's lasting contribution was not the tonic but the introduction. In 1887 he wrote to two of the most respected medical-botanical authorities in the United States — John Uri Lloyd, the eminent pharmacist of the Eclectic Medical Institute in Cincinnati, and John King, the physician who edited the great Eclectic reference work — pressing Echinacea on their attention and reportedly offering, with characteristic showmanship, to let himself be bitten by a rattlesnake to prove the remedy. Lloyd and King were initially skeptical of both the man and his claims. But they investigated the plant, and what began as a frontier curiosity promoted by a self-taught German immigrant became, within a couple of decades, one of the most widely prescribed botanical medicines in the country.
The Eclectic Physicians: Lloyd and King
The professionals who turned Echinacea into a mainstream American medicine were the Eclectic physicians — a nineteenth- and early-twentieth-century reform movement of doctors who built their practice around plant medicines and who treated North American native plants with particular seriousness. Through John King and especially John Uri Lloyd, Echinacea entered the Eclectic materia medica around 1887 and was written up in their professional literature, including the influential reference works that the Eclectics produced. These are named here as historical professional texts.
In Eclectic practice Echinacea was classed above all as an antiseptic and "blood-cleansing" remedy for sepsis and infection — what the period called a remedy for "bad blood" and conditions of "depraved" tissue. Eclectic physicians used it for boils, abscesses, carbuncles, infected and slow-healing wounds, snakebite and other venomous bites, diphtheria and other throat infections, typhoid and other fevers, and a long list of septic states — reaching for it precisely in the kinds of infectious emergencies that, in a world without antibiotics, doctors had few other tools to meet. John Uri Lloyd's pharmaceutical firm manufactured Echinacea preparations, and by the early twentieth century the herb had become one of the best-selling and most-prescribed botanicals among Eclectic and conventional physicians alike.
This Eclectic chapter matters historically for two reasons. First, it carried the Native American infection-and-wound use almost intact into formal Western practice — the indications the Eclectics wrote down are recognizably the same ones the Plains nations had used. Second, it set the agenda for everything that followed: the antimicrobial, wound-healing, and immune-supporting roles the Eclectics emphasized are exactly the areas where modern laboratory and clinical research on Echinacea has since concentrated.
Decline in America, Rebirth in Germany
Echinacea's American heyday did not last. As the Eclectic medical schools faded in the early twentieth century and the rise of laboratory pharmacology, the sulfa drugs, and then the antibiotics of the 1940s gave physicians powerful new tools against infection, the old botanical remedies fell out of mainstream use. Echinacea, the former star of the Eclectic cabinet, slipped into obscurity in its own homeland and survived mainly in folk practice.
Its revival came from Europe, and it began with a documented botanical mix-up. In the 1930s the German physician and manufacturer Gerhard Madaus traveled to the United States to obtain seed of Echinacea angustifolia — the narrow-leaved prairie species that the Eclectics had favored — and brought seed home to Germany to cultivate. As later workers established, the seed he actually grew was largely the different species Echinacea purpurea. The error proved fortunate: E. purpurea grows far more readily in European gardens than E. angustifolia, and it became the basis of a commercial pressed-juice preparation marketed under the name Echinacin, promoted as an immune-supporting remedy. Largely because of that historical accident, E. purpurea — not the species the Plains nations chiefly used — became the most cultivated, most studied, and most widely sold Echinacea in the world.
Twentieth-century Europe, and Germany in particular, became the center of Echinacea cultivation, manufacture, and research, with commercial growing also taking hold elsewhere in Europe by mid-century. Much of the modern clinical-trial literature on Echinacea uses these European preparations. The plant that the United States had nearly forgotten came back to North American shelves in the late twentieth century as a popular European-style immune remedy, and today it is among the best-selling herbal supplements in the Western world.
Why Three Species, and Why It Matters
Part of what makes Echinacea's history confusing — and part of why its modern research record is so tangled — is that "Echinacea" has never meant a single plant. Three species entered the medicine cabinet by three different historical routes, and they are not interchangeable. Echinacea angustifolia is the narrow-leaved prairie species the Plains nations used most and the one the American Eclectics adopted; its root is the traditional part. Echinacea purpurea, the broad-leaved purple coneflower of the eastern grasslands and the easy garden plant, is the species the German tradition cultivated after Madaus's mix-up and the one most modern products and trials rely on; both its root and its aerial parts are used. Echinacea pallida, the pale purple coneflower, is a third root-medicine species especially prominent in European phytotherapy.
Because these three plants carry different proportions of active compounds — and because root and aerial parts differ, and alcohol tinctures, pressed juices, and dried preparations extract different things — historical and clinical reports that simply say "Echinacea" can be describing very different medicines. A great deal of the apparent inconsistency in the record dissolves once one asks which species, which part, and which preparation. That distinction is the single most useful thing to carry from the history into any practical decision, and it is taken up in detail in the companion Echinacea Benefits articles.
From Tradition to Modern Research
The striking feature of Echinacea's history is how directly the old uses point at the modern science. The Plains nations and the Eclectic physicians used Echinacea above all for infection, for wounds, and for the throat and mouth; modern phytochemistry has since identified the plant's major active classes — the lipophilic alkamides (responsible for the characteristic tongue-tingle), the caffeic-acid derivatives such as cichoric acid and the echinacosides, and the immune-active polysaccharides and glycoproteins — and has begun to supply mechanistic explanations for exactly those traditional uses. In a particularly neat example, laboratory work has shown that Echinacea's alkamides bind selectively to the body's cannabinoid CB2 receptors, which are concentrated on immune cells, offering a plausible molecular basis for the herb's long-claimed effects on immune function.
It is important to be honest about what this does and does not mean, because real people read pages like this one to decide whether to take an herb. The traditional and Eclectic enthusiasm for Echinacea as a near-cure-all for infection runs well ahead of what modern controlled trials can confirm; the best current evidence, summarized in a major systematic review, finds at most a small and inconsistent benefit for preventing or shortening the common cold, with results that depend heavily on which preparation is tested. Echinacea is best understood today as a generally well-tolerated supportive remedy with a fascinating, genuinely Indigenous-American pedigree — not as a substitute for medical care for a serious infection. Anyone with a high fever, a wound that is spreading or not healing, a venomous bite, or an illness that is getting worse rather than better needs a clinician, not a coneflower.
That caution aside, the thread that runs from a Lakota medicine bundle, through Gilmore's 1919 field notes and the pages of the Eclectic dispensatories, through a German manufacturer's lucky seed mix-up, and into a modern receptor-binding assay is unusually unbroken and unusually well documented. Tradition raised the questions; research is now testing the answers. The detailed compounds, mechanisms, and clinical evidence are taken up in the Immune Modulation, Cold and Flu Prevention, Antimicrobial and Wound Healing, and Safety and Autoimmune Cautions articles.
Research Papers and References
The list below combines key peer-reviewed reviews and primary studies relevant to Echinacea's history, chemistry, and evidence base with curated PubMed topic-search links into the ethnobotanical and clinical literature. Historical primary sources — Linnaeus's Species Plantarum (1753), Moench's Methodus Plantas (1794), Melvin Gilmore's Uses of Plants by the Indians of the Missouri River Region (1919), and the Eclectic dispensatories of John King and John Uri Lloyd — are named in the article as historical sources rather than as modern citations. Author names, titles, and journals are given as plain text; only stable DOI/PMID links are hyperlinked, and each opens in a new tab.
- Burlou-Nagy C, Bănică F, Jurca T, Vicaș LG, Marian E, Muresan ME, Bácskay I, Kiss R, Fehér P, Pallag A. Echinacea purpurea (L.) Moench: Biological and Pharmacological Properties. A Review. Plants (Basel). 2022;11(9):1244. — doi:10.3390/plants11091244 Search PubMed
- Karsch-Völk M, Barrett B, Kiefer D, Bauer R, Ardjomand-Woelkart K, Linde K. Echinacea for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2014;(2):CD000530. — doi:10.1002/14651858.CD000530.pub3 Search PubMed
- Raduner S, Majewska A, Chen JZ, Xie XQ, Hamon J, Faller B, Altmann KH, Gertsch J. Alkylamides from Echinacea are a new class of cannabinomimetics: cannabinoid type 2 receptor-dependent and -independent immunomodulatory effects. Journal of Biological Chemistry. 2006;281(20):14192-14206. — doi:10.1074/jbc.M601074200 · PMID 16547349
- Woelkart K, Xu W, Pei Y, Makriyannis A, Picone RP, Bauer R. The endocannabinoid system as a target for alkamides from Echinacea angustifolia roots. Planta Medica. 2005;71(8):701-705. — doi:10.1055/s-2005-871290 · PMID 16142631
- Ahmadi F. Phytochemistry, Mechanisms, and Preclinical Studies of Echinacea Extracts in Modulating Immune Responses to Bacterial and Viral Infections: A Comprehensive Review. Antibiotics (Basel). 2024;13(10):947. — doi:10.3390/antibiotics13100947 · PMID 39452214
- Hobbs C. Echinacea: A Literature Review — Botany, History, Chemistry, Pharmacology, Toxicology, and Clinical Uses. HerbalGram (American Botanical Council). 1994;30:33-47. (Historical review; named as a source.)
- Echinacea ethnobotany and Native American traditional use PubMed: Echinacea Native American ethnobotany
- Echinacea alkamides, immune modulation, and the cannabinoid CB2 receptor PubMed: Echinacea alkamides CB2 immunomodulation
External Authoritative Resources
Connections
- All Herbs
- Echinacea Hub
- Echinacea Benefits Deep Dive
- Goldenseal
- Elderberry
- Astragalus
- Andrographis
- Garlic