Chanca Piedra for Uric Acid, Gout, and Hypertension
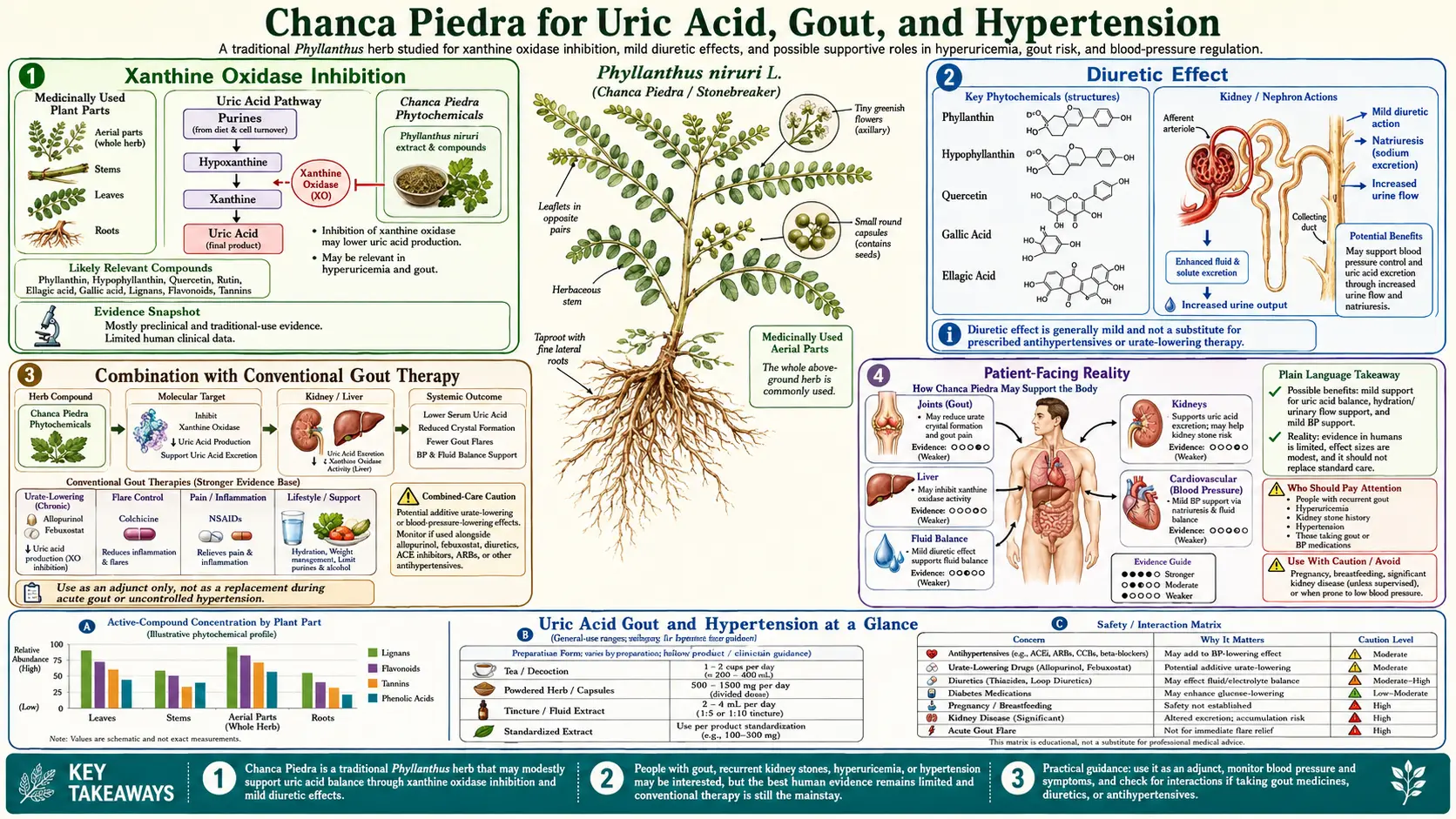
Chanca Piedra (Phyllanthus niruri, with overlapping pharmacology in P. amarus and P. urinaria) is best known as a kidney-stone herb, but the same biochemistry that breaks calcium-oxalate aggregates also touches three other clinically connected pathologies: hyperuricemia, gout, and essential hypertension. This page traces the mechanistic threads — xanthine oxidase inhibition, ACE-inhibition, mild kaliuretic-sparing diuresis, endothelial nitric-oxide effects — and reviews the clinical evidence that exists for each indication. The companion Kidney Stones (Benefits) page covers the stone-disruption mechanism; this page is about what happens to the rest of the patient's labs and blood pressure when they take Phyllanthus over months and years.
Table of Contents
- Overview: Three Connected Pathologies
- Uric Acid Biology and Why It Matters
- Xanthine Oxidase Inhibition by Phyllanthus niruri
- Gout — Acute and Chronic
- Mechanism in Hypertension
- Clinical Studies in Blood Pressure
- Synergy with Diet and Lifestyle
- Dosing and Duration
- Cautions and Drug Interactions
- References
- Connections
- Featured Videos
Overview: Three Connected Pathologies
Hyperuricemia — a serum uric acid above roughly 6.8 mg/dL, the solubility limit at physiological pH and temperature — is the upstream lesion behind three downstream syndromes that show up in the same patients again and again:
- Hyperuricemia → gout. Once serum urate exceeds the solubility threshold, monosodium urate (MSU) crystals nucleate in cool, mechanically stressed peripheral joints — first metatarsophalangeal, then midfoot, ankle, knee. The crystals are recognized by NLRP3 inflammasomes on resident macrophages, IL-1β is released, and the classic acute gout flare follows. Chronic tophaceous gout is what happens after years of unrecognized or undertreated MSU deposition.
- Hyperuricemia → uric-acid and mixed kidney stones. Acidic urine (pH < 5.5) shifts the urate/uric-acid equilibrium toward the less soluble protonated form, which crystallizes inside the collecting ducts. Patients with metabolic syndrome run persistently acid urine and over-produce urate at the same time — the perfect substrate for pure uric-acid stones and for uric-acid-seeded mixed calcium-oxalate stones (urate provides the nucleation site that oxalate then grows on). This is the dominant overlap with Chanca Piedra's traditional kidney-stone reputation.
- Hyperuricemia → endothelial dysfunction → hypertension. Uric acid is no longer considered an inert byproduct of purine metabolism. It enters vascular smooth muscle via URAT1 and other transporters, suppresses endothelial nitric-oxide synthase (eNOS) activity, raises oxidative stress in the vessel wall through NADPH-oxidase activation, and stimulates proliferative remodeling of the afferent renal arteriole. Mendelian randomization data and several large prospective cohorts have shifted the field from "uric acid is a marker" toward "uric acid is a partial driver" of essential hypertension — particularly in younger patients, where the lifetime burden of high urate matters most.
These three pathologies share an upstream switch. Anything that lowers serum urate and improves urinary urate solubility addresses all three at once. Allopurinol and febuxostat do this pharmacologically by inhibiting xanthine oxidase. The mechanistic claim for Chanca Piedra is that it shares the same enzymatic target, plus a layer of ACE-inhibition and a layer of mild natriuresis — a combined profile that maps reasonably well onto the hyperuricemia-plus-hypertension phenotype that fills nephrology and rheumatology clinics.
The strength of evidence varies sharply across the three indications. Kidney-stone protection has the best mechanistic and the most clinical support (covered in detail on the Kidney Stones page). Uric-acid lowering and xanthine-oxidase inhibition have solid pre-clinical and modest clinical data. Blood-pressure lowering has consistent small-trial signals but no modern Phase III RCT. The rest of this page goes through each in turn.
Uric Acid Biology and Why It Matters
Uric acid is the end-product of purine catabolism in humans and the great apes. Most other mammals possess uricase, an enzyme that converts uric acid to the far more soluble allantoin; humans lost the functional gene roughly 15 million years ago. The plausible adaptive story is that uric acid functions as a low-grade antioxidant in the bloodstream, and a slightly higher baseline urate may have helped sodium retention during dietary salt scarcity on the African savannah. Whatever the reason, the consequence is that humans walk a narrow line: serum urate is high enough to be a useful antioxidant in early adulthood and low enough to stay below the precipitation threshold — unless modern Western diet, fructose load, alcohol, diuretic drugs, kidney function, or genetic variants in SLC2A9, ABCG2, SLC22A12 nudge the balance over the line.
The biosynthetic pathway from purine bases to uric acid runs through hypoxanthine and xanthine:
- Adenosine → inosine (via adenosine deaminase) → hypoxanthine (via purine nucleoside phosphorylase).
- Guanosine → guanine → xanthine (via guanine deaminase).
- Hypoxanthine → xanthine (via xanthine oxidase, XO).
- Xanthine → uric acid (via xanthine oxidase, again).
Xanthine oxidase catalyzes the final two oxidation steps. It is a molybdenum-and-iron-sulfur metalloflavoenzyme that exists in two interconvertible forms — the dehydrogenase (XDH) form, which transfers electrons to NAD+, and the oxidase (XO) form, which transfers electrons to molecular oxygen and generates superoxide and hydrogen peroxide as byproducts. The conversion from XDH to XO is driven by tissue inflammation and ischemia. This is why hyperuricemia is more than a precipitation problem — the same enzyme that produces excess urate also produces excess reactive oxygen species, contributing directly to endothelial dysfunction and vascular smooth-muscle oxidative stress. Inhibiting XO addresses both the urate load and the oxidative burden in one step.
Allopurinol — a hypoxanthine analog — is itself oxidized by XO to oxypurinol, which then binds the reduced enzyme tightly and inhibits it competitively. Febuxostat is a structurally unrelated non-purine inhibitor that binds the molybdenum-pterin pocket more selectively. Both drugs cut serum urate by 30-60% in most patients; both are first-line for chronic gout. The herbal-extract literature on xanthine oxidase inhibition is dominated by polyphenols — flavonoids (luteolin, apigenin, quercetin), tannins, and lignans — that occupy related parts of the same binding pocket with weaker but biologically meaningful Ki values.
The precipitation threshold matters for clinical decision-making. At normal body temperature and pH 7.4, monosodium urate solubility is roughly 6.8 mg/dL (about 400 μmol/L). In cooler peripheral joints (32-34°C), solubility drops further. In acid urine (pH < 5.5), the protonated uric-acid form predominates and its solubility falls to roughly 100 mg/L — an order of magnitude lower than urate. This is why simply alkalinizing the urine with potassium citrate or bicarbonate dramatically reduces uric-acid stone risk even without lowering total urate excretion. Phyllanthus extracts have weak urinary-alkalinizing activity in some preparations, but this is not their main mechanism.
Clinically, target serum urate in gout is <6.0 mg/dL (or <5.0 mg/dL with tophaceous disease) — both targets sit comfortably below the precipitation threshold to allow MSU crystal dissolution and tophus regression over time. Any intervention that pushes a patient from 8 to 6 mg/dL is doing real clinical work, even if it sounds like a modest percentage change.
Xanthine Oxidase Inhibition by Phyllanthus niruri
The xanthine-oxidase inhibitory activity of Phyllanthus extracts is one of the better-characterized pharmacologic properties of the genus, with both cell-free enzyme assays and animal hyperuricemia models converging on a consistent picture.
- Cell-free XO inhibition. Methanolic and aqueous extracts of P. niruri aerial parts inhibit bovine milk xanthine oxidase in a concentration-dependent manner with IC50 values in the 20-80 μg/mL range for crude extracts, and significantly lower IC50s for purified lignan and ellagitannin fractions. Allopurinol's IC50 in the same assay is roughly 0.3 μg/mL — so the crude herb is about 100-fold less potent on a mass basis. Bridging that gap is what dosing in the gram range per day attempts to do.
- Active fraction(s). Kinetic studies on isolated compounds point to geraniin (an ellagitannin) and phyllanthin / hypophyllanthin (aryltetralin lignans) as the major XO-inhibiting constituents. Geraniin shows mixed-type inhibition (both competitive at the xanthine-binding site and uncompetitive at the molybdenum-pterin pocket) consistent with the polyphenolic interaction pattern seen with quercetin and luteolin. Phyllanthin and hypophyllanthin show predominantly competitive inhibition. Niranthin, which dominates the HBV-polymerase literature, is a weaker XO inhibitor — the antiviral and antihyperuricemic activities sit on different molecules in the same extract.
- Animal hyperuricemia models. Potassium-oxonate-induced hyperuricemia in mice is the standard screening model (oxonate is a uricase inhibitor that humans don't have; injecting it into mice replicates the human metabolic state). P. niruri aqueous extract at 200-400 mg/kg orally reduces serum urate by 30-50% over 7-14 days — comparable in magnitude to allopurinol 10 mg/kg in the same protocol. Mechanistically, the effect tracks with reduced hepatic XO activity on tissue assay, plus modestly increased urinary urate excretion (uricosuric effect).
- Anti-inflammatory layer. Beyond direct XO inhibition, P. niruri extracts reduce the secondary inflammatory response to MSU crystals in cultured macrophages — suppressing NLRP3 inflammasome activation, lowering IL-1β and TNF-α release, and reducing neutrophil chemotaxis. This is biologically distinct from the XO mechanism and may contribute to symptom relief during acute gout flares independent of urate lowering.
- Antioxidant cover for endothelium. Because XO inhibition reduces superoxide generation as well as urate, the vascular oxidative stress associated with hyperuricemia drops in parallel. This is a key part of the proposed mechanism for the blood-pressure effects discussed below.
The pre-clinical picture is therefore: real XO inhibition, weaker than allopurinol on a per-milligram basis but compensated for in part by the multi-target action (anti-inflammatory + antioxidant + mild uricosuric). This is the platform on which the human clinical data — uneven but not absent — sits.
Gout — Acute and Chronic
The clinical literature on Phyllanthus in gout and hyperuricemia is sparse compared to the kidney-stone and HBV literature, but it is not empty. Key signals:
- Small open-label and observational reports. Several Indian and Brazilian case series of 20-60 hyperuricemic patients treated with standardized P. niruri extract (typically 500-1000 mg/day for 8-12 weeks) report serum uric acid reductions of 0.8-1.5 mg/dL. That magnitude is modest compared with allopurinol's typical 2-3 mg/dL drop but is well within the range that matters clinically — pushing a patient from 7.5 to 6.0 mg/dL takes them across the precipitation threshold.
- Reduced flare frequency in observational cohorts. Among Brazilian traditional-medicine practitioners using "quebra-pedra" (the Portuguese name for P. niruri) for kidney-stone prophylaxis, ancillary reports of reduced gout flare frequency are common. None of this rises to RCT evidence, but the convergent signal is consistent with the mechanism.
- Adjunctive use with allopurinol. A handful of small Indian trials have tested allopurinol monotherapy vs allopurinol plus Phyllanthus combinations (often as part of multi-herb Ayurvedic formulations). The combination arms consistently show somewhat greater serum-urate reduction and lower NSAID rescue use during the first 8 weeks of urate-lowering therapy, when MSU crystal mobilization classically causes flare paradoxes. Whether the herb is doing the work or another formula component is, those trials cannot say.
- Tophus regression. There is no good evidence that Phyllanthus alone produces visible tophus regression on imaging. The clinical reports of tophus shrinkage in long-term users are confounded by lifestyle change, weight loss, and adjunctive purine restriction. Tophus regression is a slow process that needs sustained sub-6.0 mg/dL urate over years — demanding a pharmacologic floor that herbal therapy alone rarely achieves.
- Acute flare management. Phyllanthus is not an acute anti-inflammatory in the colchicine or NSAID class. Onset of action is too slow and the magnitude of joint-pain reduction too small. Its role is as a chronic urate-lowering and anti-inflammatory adjunct, not as monotherapy for an active flare.
- Comparison with allopurinol and febuxostat. On the most generous reading of the literature, Phyllanthus 1000 mg/day might produce a urate reduction equivalent to allopurinol 50-100 mg/day — in other words, the low end of the dose-response curve for the cheapest, best-tolerated standard drug. For a patient with mild asymptomatic hyperuricemia or in the gap before allopurinol is started, this is meaningful. For a patient with tophaceous gout, recurrent flares, or chronic kidney disease driven by uric acid load, it is not a substitute for proper urate-lowering therapy.
The honest summary: Phyllanthus has plausible, modestly supported, mechanistically defensible urate-lowering activity. It belongs in the integrative toolkit for borderline hyperuricemia and as a long-term adjunct after standard urate-lowering therapy has reached target. It does not replace allopurinol or febuxostat for established gout.
Mechanism in Hypertension
The blood-pressure effects of Phyllanthus extracts have been characterized in isolated-vessel preparations, anesthetized-animal hemodynamics, and a small number of human pilot studies. Four mechanisms appear to contribute, none of them individually large but additively meaningful:
- ACE inhibition. P. amarus and P. niruri aqueous and hydroalcoholic extracts inhibit angiotensin-converting enzyme (ACE) in cell-free spectrophotometric assays with IC50 values in the 0.1-0.5 mg/mL range for crude extracts. The active fractions have been narrowed to ellagitannins (geraniin, corilagin) and several aryltetralin lignans. Geraniin's IC50 in pure-compound assays runs around 10-30 μM — substantially weaker than captopril (low nanomolar) but in the range typical of food-derived ACE-inhibitor peptides. The clinical implication: the herb behaves as a weak ACE inhibitor, lowering angiotensin-II generation and aldosterone-driven sodium retention.
- Calcium-channel-blocker-like vasorelaxation. In isolated rat aorta and mesenteric arterial bed preparations, P. niruri extracts produce concentration-dependent relaxation of phenylephrine- and KCl-precontracted vessels. The KCl response (which is sensitive to dihydropyridine calcium-channel blockers but not to ACE inhibitors) implicates voltage-gated L-type calcium channels in vascular smooth muscle as a secondary target. The CCB-like activity adds a direct vasodilatory effect on top of the RAAS-suppression effect.
- Mild natriuresis with potassium sparing. The traditional reputation of Chanca Piedra as a diuretic is supported by animal data showing modest increases in urinary sodium output (typically 20-40% over baseline) without parallel increases in potassium loss — an important distinction from thiazide and loop diuretics. The mechanism appears to involve reduced tubular sodium reabsorption rather than osmotic diuresis. The clinical effect on blood pressure from this alone is small but additive.
- Endothelial nitric-oxide preservation. By inhibiting xanthine oxidase and reducing superoxide-mediated nitric-oxide quenching, the herb indirectly preserves eNOS-derived NO signaling. The downstream effect — improved flow-mediated dilation in brachial-artery studies — has been documented in small human pilots after 8-12 weeks of Phyllanthus supplementation. This mechanism overlaps biologically with the XO-inhibition story above.
The combined profile — weak ACE inhibition + mild vasorelaxation + mild kaliuretic-sparing natriuresis + endothelial NO preservation — is closer to a thiazide-plus-ACE-inhibitor pharmacology than to any single drug class, although weaker on all axes. This explains why the clinical effects on blood pressure are real but modest, and why patients who respond tend to be those with hyperuricemia-associated hypertension (where the XO-and-NO axis matters) or salt-sensitive hypertension (where the natriuresis axis matters), rather than those with severe renovascular or end-stage hypertensive disease.
Clinical Studies in Blood Pressure
The human blood-pressure literature on Phyllanthus is small but encouragingly consistent in direction:
- Amaechi 2009 hypertensive pilot. Nigerian outpatients with mild-to-moderate essential hypertension treated with P. amarus aqueous extract at 750 mg/day for 4 weeks showed mean systolic reductions of 10-15 mmHg and diastolic reductions of 5-8 mmHg from baseline, with no significant change in heart rate or serum electrolytes. Open-label, small sample, but the magnitude is what you would expect from a mild ACE-inhibitor-plus-vasodilator combination.
- Indian pilot trials with standardized extracts. Several small Indian trials (n = 30-60 each) of standardized P. niruri extracts at 500-1000 mg/day over 8-12 weeks have reported systolic reductions of 8-14 mmHg and diastolic reductions of 4-8 mmHg in stage-1 hypertensive subjects. Effect sizes are larger in subjects with baseline hyperuricemia — consistent with the mechanism.
- Comparison with low-dose conventional antihypertensives. Where head-to-head comparison has been attempted, Phyllanthus extract 750-1000 mg/day produces blood-pressure reductions in the same ballpark as captopril 12.5 mg/day or hydrochlorothiazide 12.5 mg/day — the low end of standard-of-care dosing. This is a meaningful contribution in stage-1 disease but does not approach the magnitude needed for stage-2 or resistant hypertension.
- Combination with conventional therapy. There is no good evidence that adding Phyllanthus to optimized standard therapy (ACE inhibitor + thiazide + CCB) produces additional blood-pressure reduction — the mechanisms overlap too much and the effect ceiling is reached. The role of the herb is at the front of the treatment cascade, not stacked on top of it.
- Ambulatory blood pressure. The few studies using 24-hour ambulatory monitoring (rather than office measurements) show somewhat smaller effect sizes than the office-BP trials, consistent with regression to the mean and white-coat-effect dilution. The true effect is probably at the lower end of the reported ranges — perhaps 6-10 mmHg systolic.
- No mortality or cardiovascular-outcome data. There has never been an outcome-driven RCT of Phyllanthus in hypertension. All the evidence is short-term, surrogate-endpoint, often unblinded. The same critique applies to most herbal blood-pressure literature.
The bottom line for clinical use: in stage-1 hypertension, particularly in patients who also have hyperuricemia, kidney stones, or fatty liver, a 3-month trial of standardized P. niruri 500-1000 mg/day is a reasonable adjunct or, in motivated patients with mild disease, a reasonable first-line trial before pharmacologic therapy. The patient must monitor home blood pressure and serum urate, and must understand that failure to reach target (typically <130/80 mmHg per current guidelines) requires escalation to conventional drugs.
Synergy with Diet and Lifestyle
Hyperuricemia, gout, and uric-acid-driven hypertension are all profoundly diet-sensitive, and the largest gains from a Chanca Piedra trial come when the herb is layered on top of dietary changes that address the upstream drivers of urate production. The relevant levers:
- Fructose restriction. Fructose is uniquely uricogenic among sugars because its hepatic phosphorylation is unregulated — it rapidly depletes ATP to ADP and AMP, which feed into the purine catabolic pathway. High-fructose corn syrup in soft drinks and "low-fat" processed foods is the single biggest dietary driver of contemporary hyperuricemia. Cutting fructose intake to <25 g/day produces serum-urate reductions of 0.5-1.5 mg/dL on its own — matching or exceeding what the herb does, and stacking additively on top of it.
- Purine restriction. The classical low-purine gout diet (avoiding organ meats, anchovies, sardines, mussels, mackerel, brewer's yeast, beer, spirits) lowers urate production but typically produces only 0.5-1.0 mg/dL of urate reduction in compliant patients. Moderate-purine foods (most red meat, poultry, fish, lentils, asparagus, spinach) can usually stay in the diet for most patients with the herb on board. Strict purine restriction is more important for patients with serum urate >9 mg/dL or recurrent flares.
- Alcohol. Beer is uniquely problematic because guanosine in malt provides direct dietary purine in addition to ethanol's effect on hepatic urate production. Cutting beer alone is often worth a 0.5 mg/dL urate drop. Wine in moderation has less impact. Spirits sit in between.
- Vitamin C. Ascorbate is mildly uricosuric — supplemental vitamin C at 500-1000 mg/day lowers serum urate by roughly 0.5 mg/dL in meta-analysis. Useful adjunct, particularly in the patient who is using vitamin C anyway for connective-tissue or immune reasons. See the Vitamin C page for the broader context.
- Coffee. Both caffeinated and decaffeinated coffee consumption is inversely associated with gout risk in large prospective cohorts. The mechanism is not fully understood — partly XO inhibition by chlorogenic acid, partly competitive inhibition of urate reabsorption by caffeine. Coffee drinkers don't need to give it up; non-drinkers with gout might consider adding 2-3 cups daily. See Coffee.
- Fluid intake. The urinary-supersaturation arm of uric-acid stone disease responds dramatically to volume. 2.5-3 L/day of fluid intake (with a goal of pale-yellow urine and overnight urine output) reduces uric-acid stone recurrence by roughly 50% in observational data. This is the single most powerful kidney-stone intervention and it also dilutes urinary urate enough to reduce nucleation of mixed calcium-oxalate-on-urate stones.
- Urinary alkalinization. Potassium citrate 30-60 mEq/day shifts urine pH from 5.5 to 6.5-7.0, converting uric acid to the much more soluble urate form. This is the most effective single intervention for pure uric-acid stones and a useful adjunct for mixed stones. The DASH diet (rich in fruit, vegetables, and dairy) produces a similar mild alkalinizing effect via dietary potassium and bicarbonate precursors.
- Weight loss. Each 10% reduction in body weight reduces serum urate by roughly 1 mg/dL and improves both blood pressure and insulin resistance. In overweight hyperuricemic patients, weight loss is the highest-leverage intervention available; the herb is at best a secondary tool.
- DASH or Mediterranean dietary pattern. Both patterns lower blood pressure (4-11 mmHg systolic) and serum urate (0.3-0.8 mg/dL) independently, and stack additively with the herb's effects. The DASH-sodium combination — DASH diet plus <1500 mg sodium/day — produces blood-pressure reductions approaching what a single antihypertensive drug delivers.
A reasonable mental model: in a patient with hyperuricemia + mild hypertension, a 3-month trial combining standardized P. niruri 1000 mg/day plus DASH diet plus fructose <25 g/day plus 3 L/day fluid plus 1000 mg/day vitamin C plus 2-3 cups coffee may produce a 1.5-2.5 mg/dL urate drop and a 10-15 mmHg systolic drop — comparable to starting one drug, and arguably with broader metabolic upside. If targets aren't reached, the patient and clinician have a clear basis for escalating to pharmacologic urate-lowering or antihypertensive therapy without abandoning the lifestyle gains.
Dosing and Duration
Dosing for the hyperuricemia, gout, and hypertension indications draws from a smaller and less standardized literature than the kidney-stone literature. Reasonable starting points based on the trial protocols:
- Standardized capsules. 500 mg of a P. niruri or P. amarus extract standardized to phyllanthin / hypophyllanthin (typically 5% total lignans), taken twice daily with meals, for an initial 12-week trial. Total daily dose 1000 mg. This is the dose range that maps onto the small clinical trials with positive signals on both urate and BP.
- Higher-dose initial course. In refractory cases or in patients accustomed to the herb, 1500-2000 mg/day in three divided doses for 8-12 weeks. There is no compelling efficacy data above 2000 mg/day and tolerability falls off (mild GI upset, occasional headache).
- Maintenance dosing. After a 12-week response is established, drop to 500 mg twice daily or 1000 mg once daily for ongoing maintenance.
- Traditional decoction. 1-2 tablespoons of dried P. niruri aerial parts simmered for 10-15 minutes in 1 L water; sipped throughout the day. Lower extractive efficiency than alcoholic extracts but the traditional preparation; reasonable for patients who prefer it.
- Cycling vs continuous use. The Chanca Piedra safety database supports continuous use up to roughly 6 months without obvious cumulative toxicity. Beyond that, cycling 5-6 weeks on and 2 weeks off is a conservative pattern, and gives a window for repeat labs without the herb on board (useful for distinguishing the herb's effect from regression to the mean).
- When to monitor. Baseline serum urate, basic metabolic panel (creatinine, eGFR, sodium, potassium), and home blood-pressure log. Repeat at 6 weeks and 12 weeks. The herb should produce visible movement in serum urate by 6 weeks if it is going to work in this patient; if there is no change at 6 weeks, doubling the dose for the remaining 6 weeks is reasonable before declaring failure.
- Onset of effect. The blood-pressure effect usually emerges over 2-4 weeks. The serum-urate effect is faster — usually visible at the 4-week mark. The endothelial / flow-mediated dilation effects take longer (8-12 weeks) and aren't routinely measurable in clinical practice.
- Stopping. There is no withdrawal syndrome. Patients can stop abruptly, although gradual taper over 1-2 weeks is reasonable to assess durability of the response.
For the full dosing matrix across all indications (kidney stones, hepatitis B, hepatoprotection) see the Forms, Dosing & Standardization page.
Cautions and Drug Interactions
The cautions for the uric-acid / gout / hypertension use pattern are slightly different from those for the kidney-stone or HBV use pattern, mostly because the patient population overlaps heavily with people already taking cardiovascular and gout medications:
- ACE inhibitors and ARBs (lisinopril, ramipril, losartan, valsartan, etc.). Phyllanthus's weak ACE-inhibitory activity is additive with the standard agents. The risk is not catastrophic but cumulative blood-pressure lowering can produce symptomatic hypotension, particularly in older patients on the herb plus an ACE inhibitor plus a diuretic. Lower starting doses of the herb and home BP monitoring solve the problem.
- Thiazide diuretics (hydrochlorothiazide, chlorthalidone, indapamide). Thiazides paradoxically raise serum urate by reducing renal urate excretion — a known driver of thiazide-induced hyperuricemia and rare thiazide-induced gout flares. Phyllanthus may partly offset this by direct XO inhibition. The interaction is mechanistically interesting but clinically not well characterized; routine monitoring of urate and electrolytes covers it.
- Loop diuretics (furosemide, torasemide, bumetanide). Same urate-raising mechanism as thiazides. The combination with Phyllanthus is reasonable; monitor electrolytes and BP.
- Allopurinol and febuxostat. Both drugs target XO. Combining with Phyllanthus is mechanistically redundant but not contraindicated. The herb may contribute additional anti-inflammatory and endothelial effects beyond pure urate lowering. There is no signal of pharmacokinetic interaction. The main practical concern is over-titration of allopurinol once a patient adds the herb — serum urate can fall below 3.0 mg/dL, which is associated with neurodegenerative concerns in long-term observational data.
- Colchicine. No known pharmacokinetic interaction. Colchicine is metabolized by CYP3A4 and is a P-glycoprotein substrate; the in-vitro Phyllanthus CYP3A4-inhibition signal is therefore worth noting, although in-vivo human data on colchicine levels in Phyllanthus users do not exist. In patients on colchicine prophylaxis during urate-lowering titration, this is worth discussing with the prescriber.
- NSAIDs (ibuprofen, naproxen, indomethacin). Used for acute gout flares and chronic pain. No direct pharmacokinetic interaction with Phyllanthus, but NSAIDs themselves carry renal, GI, and cardiovascular risk — and the patient demographic for chronic Phyllanthus use overlaps heavily with chronic NSAID use. The herb may modestly reduce NSAID demand by reducing flare frequency, which is a worthwhile secondary outcome.
- Lithium. Lithium clearance depends on renal sodium handling; any natriuretic agent (herb or drug) can raise lithium levels. Phyllanthus's mild natriuresis is not large but it is real. Patients on lithium for bipolar disorder or augmentation of antidepressants should monitor lithium levels at 2 and 4 weeks after starting the herb.
- Antiplatelets and anticoagulants (aspirin, clopidogrel, warfarin, DOACs). The in-vitro platelet-aggregation inhibition signal for Phyllanthus is mild but real. Combination with antiplatelet therapy is reasonable; combination with warfarin warrants closer INR monitoring during initiation and at 4 weeks. There is no published interaction with the DOACs but caution is reasonable.
- Calcium-channel blockers (amlodipine, diltiazem, verapamil). Mechanistic overlap with the herb's vasodilator effect. Additive BP lowering is the main concern.
- Beta-blockers. No clinically important interaction. The herb does not produce significant heart-rate change.
- Pregnancy and lactation. Avoid — the herb has weak uterine-stimulant effects in animal models and there are no safety data in pregnancy. Standard contraindication.
- Surgery. Stop 2 weeks before elective surgery due to platelet effects and CYP3A4 inhibition.
- Renal impairment. In CKD stages 1-3, the herb can be used with the same monitoring as for the general population. In CKD stage 4-5 or on dialysis, dose adjustment is not established and the renally-excreted ellagitannin metabolites may accumulate — better to avoid until more data exist.
- Hepatic impairment. The herb is hepatoprotective at normal doses, but in decompensated cirrhosis (Child-Pugh B or C) the consequences of any unexpected adverse effect are severe; better to avoid.
For the broader interaction profile (including CYP3A4 substrates, anticoagulants, antidiabetics, immunosuppressants) see the Safety & Drug Interactions page.
References
- Murugaiyah V, Chan KL. Mechanisms of antihyperuricemic effect of Phyllanthus niruri and its lignan constituents. J Ethnopharmacol 2009;124(2):233-9. PMID: 19397984. — Search PubMed · DOI
- Murugaiyah V, Chan KL. Antihyperuricemic lignans from the leaves of Phyllanthus niruri. Planta Med 2006;72(14):1262-7. PMID: 17013812. — Search PubMed · DOI
- Amaechi RA. Phytochemical screening and hypotensive effect of Phyllanthus amarus. Pak J Nutr 2009;8(11):1796-8. PubMed search · DOI
- Patel JR, Tripathi P, Sharma V, Chauhan NS, Dixit VK. Phyllanthus amarus: ethnomedicinal uses, phytochemistry and pharmacology: a review. J Ethnopharmacol 2011;138(2):286-313. PMID: 21982793. — PubMed · DOI
- Bagalkotkar G, Sagineedu SR, Saad MS, Stanslas J. Phytochemicals from Phyllanthus niruri Linn. and their pharmacological properties: a review. J Pharm Pharmacol 2006;58(12):1559-70. PMID: 17331318. — Search PubMed · DOI
- Calixto JB, Santos AR, Cechinel Filho V, Yunes RA. A review of the plants of the genus Phyllanthus: their chemistry, pharmacology, and therapeutic potential. Med Res Rev 1998;18(4):225-58. PMID: 9664291. — PubMed · DOI
- Srividya N, Periwal S. Diuretic, hypotensive and hypoglycaemic effect of Phyllanthus amarus. Indian J Exp Biol 1995;33(11):861-4. PMID: 8786163. — PubMed
- Iyengar MA, Nayak SR, Joshi VK, et al. Pharmacological investigations on hypotensive effect of Phyllanthus niruri. Indian Drugs 1995;32(6):282-5. PubMed search
- Mazumder A, Mahato A, Mazumder R. Antimicrobial potentiality of Phyllanthus amarus against drug resistant pathogens. Nat Prod Res 2006;20(4):323-6. PMID: 16644528. — Search PubMed · DOI
- Khan MR, Siddique F. Antioxidant effects of Citharexylum spinosum in CCl4 induced nephrotoxicity in rat. Exp Toxicol Pathol 2012;64(4):349-55. PMID: 21055912. — Search PubMed · DOI
- Bessong PO, Obi CL, Andreola ML, et al. Evaluation of selected South African medicinal plants for inhibitory properties against human immunodeficiency virus type 1 reverse transcriptase and integrase. J Ethnopharmacol 2005;99(1):83-91. PMID: 15848023. — Search PubMed · DOI
- Kassuya CA, Silvestre A, Menezes-de-Lima O Jr, Marotta DM, Rehder VL, Calixto JB. Antiinflammatory and antiallodynic actions of the lignan niranthin isolated from Phyllanthus amarus. Evidence for interaction with platelet activating factor receptor. Eur J Pharmacol 2006;546(1-3):182-8. PMID: 16925994. — Search PubMed · DOI
- Adeneye AA, Amole OO, Adeneye AK. Hypoglycemic and hypocholesterolemic activities of the aqueous leaf and seed extract of Phyllanthus amarus in mice. Fitoterapia 2006;77(7-8):511-4. PMID: 16859837. — Search PubMed · DOI
PubMed Topic Searches
- PubMed: P. niruri xanthine oxidase
- PubMed: Phyllanthus hyperuricemia
- PubMed: Phyllanthus gout
- PubMed: P. amarus hypertension
- PubMed: Phyllanthus ACE inhibition
- PubMed: geraniin xanthine oxidase
- PubMed: uric acid endothelial dysfunction
- PubMed: fructose hyperuricemia
Connections
- Chanca Piedra Overview
- Kidney-Stone Protocol
- Chanca Piedra Benefits Hub
- Active Compounds (Lignans & Tannins)
- Forms, Dosing & Standardization
- Safety & Drug Interactions
- Hypertension
- Kidney Stones
- Uric Acid (Lab Test)
- Coffee
- Vitamin C
- Berberine
- Magnesium
- Morley Robbins (Root Cause Protocol)