Bitter Melon — Benefits Deep Dive
Bitter melon (Momordica charantia, known as karela in Hindi and bitter gourd in English) is a tropical cucurbit vine whose intensely bitter unripe fruit has been the most extensively used plant remedy for diabetes across both the Indian Ayurvedic and Chinese herbal traditions for over a thousand years. Modern phytochemistry has identified at least three distinct hypoglycemic principles — the steroidal-saponin mixture charantin, the 17-amino-acid polypeptide-p (sometimes called “plant insulin” or p-insulin), and the glycoalkaloid vicine — that operate through complementary mechanisms more diverse than any single pharmaceutical drug. Cell-culture and animal data are unusually strong; human randomized controlled trial data are positive but modest in effect size, and importantly, head-to-head against pharmaceutical metformin bitter melon was the less effective agent (Fuangchan 2011). Four benefit pages below explore the conditions where bitter melon produces measurable clinical effect — fasting glucose and HbA1c reduction, the downstream microvascular and macrovascular complications of long-standing diabetes, weight loss and insulin resistance via AMPK-like activation, and the in vitro cucurbitacin cancer-cell research that justifies further study but does not justify treating bitter melon as a cancer therapy.
Deep-Dive Articles
Blood Sugar Regulation
The mechanistic and clinical case for bitter melon as a glycemic agent: charantin (steroidal-saponin mixture isolated by Lolitkar 1962, confirmed hypoglycemic by Welihinda 1986), polypeptide-p (17-amino-acid plant insulin-mimetic isolated by Khanna 1981), the comprehensive Krawinkel & Keding 2014 mechanistic review, and the Yin et al. 2015 systematic review and meta-analysis of randomized controlled trials showing fasting glucose and HbA1c reduction across multiple human trials.
Diabetes Complications
Insulin resistance trials, HbA1c response curves, the seminal head-to-head Fuangchan 2011 randomized trial against pharmaceutical metformin (bitter melon less effective than 1 g/day metformin but still glucose-lowering), Indian Charantia trials in newly diagnosed type 2 diabetes, downstream microvascular complications (retinopathy, neuropathy, nephropathy), and the practical role of bitter melon as an early-stage adjunct rather than a metformin replacement.
Weight Loss
The Yibchok-anun et al. 2006 study of insulin secretagogue activity, the Chaturvedi 2012 review of antidiabetic and weight-loss effects, traditional Chinese (kŭgua) and Indian (karela) uses for “excess heat” and metabolic stagnation, AMPK-like activation pathway (the same molecular target as exercise and metformin), reductions in visceral adipose tissue, and the appropriate magnitude expectation — bitter melon is a modest metabolic adjunct, not a stand-alone weight-loss intervention.
Cancer Cell Studies
The in vitro cucurbitacin and momordicin antiproliferative literature, traditional Chinese use of bitter melon for “tumors” and “swellings” in classical formularies, the MAP30 ribosome-inactivating protein research, and an honest framing of the evidence base — cell-culture and animal-model data are real but human clinical trials are limited to small phase-I and pilot studies. Bitter melon is NOT a cancer treatment. It may have value as part of an integrative supportive protocol under oncologist supervision; it cannot replace established cancer therapy.
Table of Contents
- Deep-Dive Articles
- Why Bitter Melon Produces Effects
- Key Research Papers
- External Authoritative Resources
- Cautions and Contraindications
- Connections
- Featured Videos
Why Bitter Melon Produces Effects
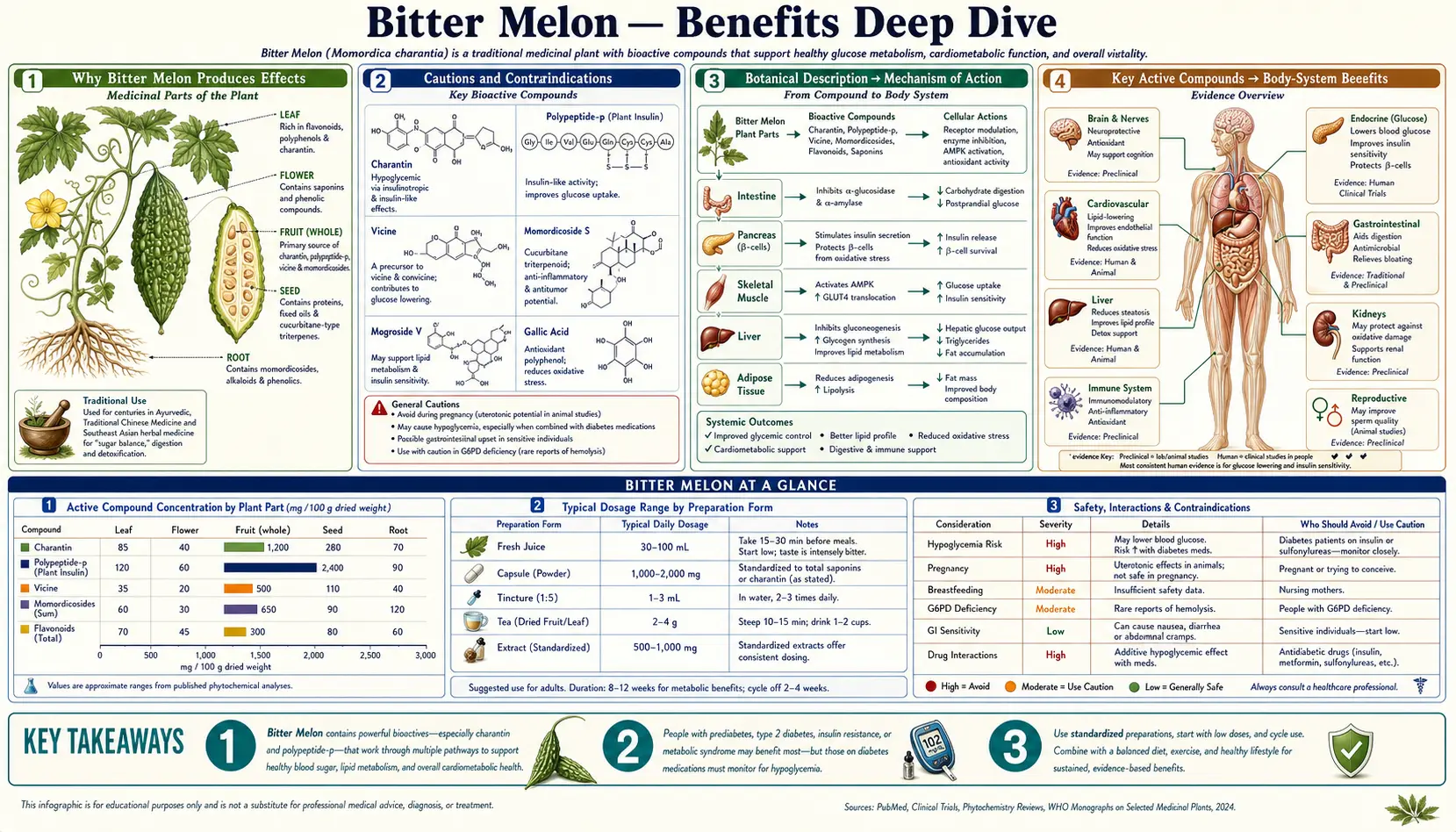
Most botanical hypoglycemic agents act through one or two mechanisms. Bitter melon is unusual because at least five distinct mechanisms have been documented in cell-culture and animal-model work, mediated by at least three structurally unrelated compound classes. This polypharmacy may explain why bitter melon's clinical effect is broader than the magnitude alone would suggest — it nibbles at multiple points along the glucose-handling and energy-metabolism pathways rather than slamming one receptor hard.
- Charantin (steroidal-saponin glucoside mixture) — first isolated by Lolitkar and Rao in 1962 as the principal hypoglycemic principle, charantin is a mixture of sitosteryl glucoside and stigmasteryl glucoside that increases peripheral glucose uptake in skeletal muscle and adipose tissue and improves hepatic glycogen storage. The Welihinda et al. 1986 work in Journal of Ethnopharmacology confirmed the dose-dependent fasting glucose reduction in human subjects with type 2 diabetes given a charantin-enriched extract.
- Polypeptide-p (plant insulin / p-insulin) — a 17-amino-acid peptide isolated from bitter melon fruit, seeds, and tissue by Khanna et al. in 1981. The molecule has measurable structural similarity to bovine insulin, binds insulin receptors with low affinity, and produces a hypoglycemic effect when administered subcutaneously to diabetic rabbits, dogs, and a small number of human subjects. Orally administered polypeptide-p is largely degraded by gastric protease, which limits clinical utility of the standardized whole-fruit preparation by oral route — but the compound's existence proves the “plant insulin” mechanism is real, not merely metaphor.
- AMPK-like activation — bitter melon constituents activate AMP-activated protein kinase (AMPK), the master cellular energy sensor that is also the molecular target of pharmaceutical metformin, of exercise, and of caloric restriction. AMPK activation increases skeletal-muscle GLUT4 translocation (insulin-independent glucose uptake), suppresses hepatic gluconeogenesis, and shifts cellular metabolism toward fatty-acid oxidation. This is the mechanism that links the glucose-lowering and weight-loss effects.
- Alpha-glucosidase and alpha-amylase inhibition — in vitro work has shown bitter melon extracts inhibit the intestinal disaccharidase enzymes that liberate glucose from dietary starch and sucrose, slowing post-prandial glucose absorption in the same general manner as the pharmaceutical acarbose. This contributes to the lower post-meal glucose spike documented in several clinical trials.
- Cucurbitacin and momordicin triterpenoid effects — the bitter triterpenoids responsible for the characteristic flavor have documented anti-inflammatory and antiproliferative activity in cell culture. These contribute to the cancer-cell research literature discussed in the corresponding deep-dive, and likely to the general “cooling” and anti-inflammatory effect described in both Ayurvedic and Traditional Chinese Medicine.
The therapeutic complication is that the same plant that helpfully nibbles at five mechanisms also contains vicine, the glycoalkaloid found in seeds (and in fava beans, which is where the term “favism” comes from). Vicine is metabolized to a hydrogen-peroxide-generating quinone that destroys red blood cells in individuals with G6PD deficiency. G6PD deficiency is the most common human enzymopathy worldwide, affecting an estimated 400 million people, with highest prevalence in Mediterranean, African, Middle Eastern, and South/Southeast Asian populations — precisely the populations that have used bitter melon medicinally for centuries. Anyone of G6PD-deficient ancestry should be tested before regular bitter melon use, and seeds should be discarded before consumption.
A second hard contraindication is pregnancy — bitter melon has documented uterine-stimulating activity and has been used as an abortifacient in folk medicine across multiple cultures. The Charantia trials excluded pregnant women, and modern reviews uniformly list pregnancy as an absolute contraindication.
Key Research Papers
- Welihinda J, Karunanayake EH, Sheriff MH, Jayasinghe KS (1986). Effect of Momordica charantia on the glucose tolerance in maturity onset diabetes. Journal of Ethnopharmacology 17(3):277-282. — PubMed: Welihinda 1986 glucose tolerance
- Krawinkel MB, Keding GB (2006). Bitter gourd (Momordica charantia): a dietary approach to hyperglycemia. Nutrition Reviews 64(7 Pt 1):331-337. — PubMed: Krawinkel & Keding mechanistic review
- Yin RV, Lee NC, Hirpara H, Phung OJ (2014). The effect of bitter melon (Mormordica charantia) in patients with diabetes mellitus: a systematic review and meta-analysis. Nutrition & Diabetes 4(12):e145. — PubMed: Yin 2014/2015 meta-analysis
- Fuangchan A, Sonthisombat P, Seubnukarn T, Chanouan R, Chotchaisuwat P, Sirigulsatien V, Ingkaninan K, Plianbangchang P, Haines ST (2011). Hypoglycemic effect of bitter melon compared with metformin in newly diagnosed type 2 diabetes patients. Journal of Ethnopharmacology 134(2):422-428. — PubMed: Fuangchan 2011 vs metformin
- Khanna P, Jain SC, Panagariya A, Dixit VP (1981). Hypoglycemic activity of polypeptide-p from a plant source. Journal of Natural Products 44(6):648-655. — PubMed: Khanna 1981 polypeptide-p
PubMed Topic Searches
- PubMed: Momordica diabetes RCTs
- PubMed: Charantin chemistry
- PubMed: Polypeptide-p / plant insulin
- PubMed: Momordica AMPK pathway
- PubMed: Vicine and G6PD deficiency
- PubMed: MAP30 ribosome-inactivating protein
External Authoritative Resources
- NCCIH — Herbs at a Glance
- MedlinePlus — Bitter Melon
- Memorial Sloan Kettering — Bitter Melon (Integrative Medicine)
- PubMed — All research on Momordica charantia (~3,500+ papers)
- WHO — Traditional Medicine
Cautions and Contraindications
- G6PD deficiency (favism risk) — the seeds contain vicine, the same glycoalkaloid that causes the acute hemolytic crisis after fava bean ingestion in G6PD-deficient individuals. G6PD deficiency is the most common human enzymopathy worldwide (~400 million affected), with highest prevalence in Mediterranean, African, Middle Eastern, and South/Southeast Asian populations. Anyone of these ancestries should be tested for G6PD before regular bitter melon use, and seeds must be discarded before consumption. Symptoms of hemolytic crisis include sudden fatigue, dark or tea-colored urine, jaundice, and shortness of breath, typically beginning 24-48 hours after ingestion.
- Pregnancy (absolute contraindication) — bitter melon has documented uterine-stimulating activity and has been used as an abortifacient in folk medicine across multiple cultures. Pregnant women should avoid all forms (juice, extract, food, tea).
- Hypoglycemia risk in combination with diabetes medication — when combined with insulin, sulfonylureas, or metformin, bitter melon can produce additive hypoglycemia. Monitor blood glucose regularly and adjust medication dosing with the prescribing physician.
- Pediatric use — the bright red ripe fruit and seeds have caused vomiting, diarrhea, and hypoglycemic coma in infants and young children. Avoid in pediatric patients.
- Male fertility — some animal studies have suggested high-dose bitter melon may impair male fertility (reversible after discontinuation). Couples actively trying to conceive should avoid sustained high-dose supplementation.
- Not a replacement for established therapy — bitter melon is a modest metabolic adjunct, less potent than pharmaceutical metformin (Fuangchan 2011), and is NOT a cancer treatment despite encouraging in vitro data. Anyone with diabetes, cancer, or any other diagnosed condition should use bitter melon as an integrative add-on under medical supervision, not as a stand-alone replacement for evidence-based pharmaceutical therapy.
Connections
- Bitter Melon (Main Page)
- Bitter Melon for Blood Sugar
- Bitter Melon for Diabetes Complications
- Bitter Melon for Weight Loss
- Bitter Melon Cancer Cell Studies
- All Herbs
- Berberine
- Gymnema
- Cinnamon
- Fenugreek
- Diabetes
- Insulin Resistance
- HbA1c
- Fasting Insulin
- Blood Sugar
- Fasting