Chia Seeds for Calcium and Bone
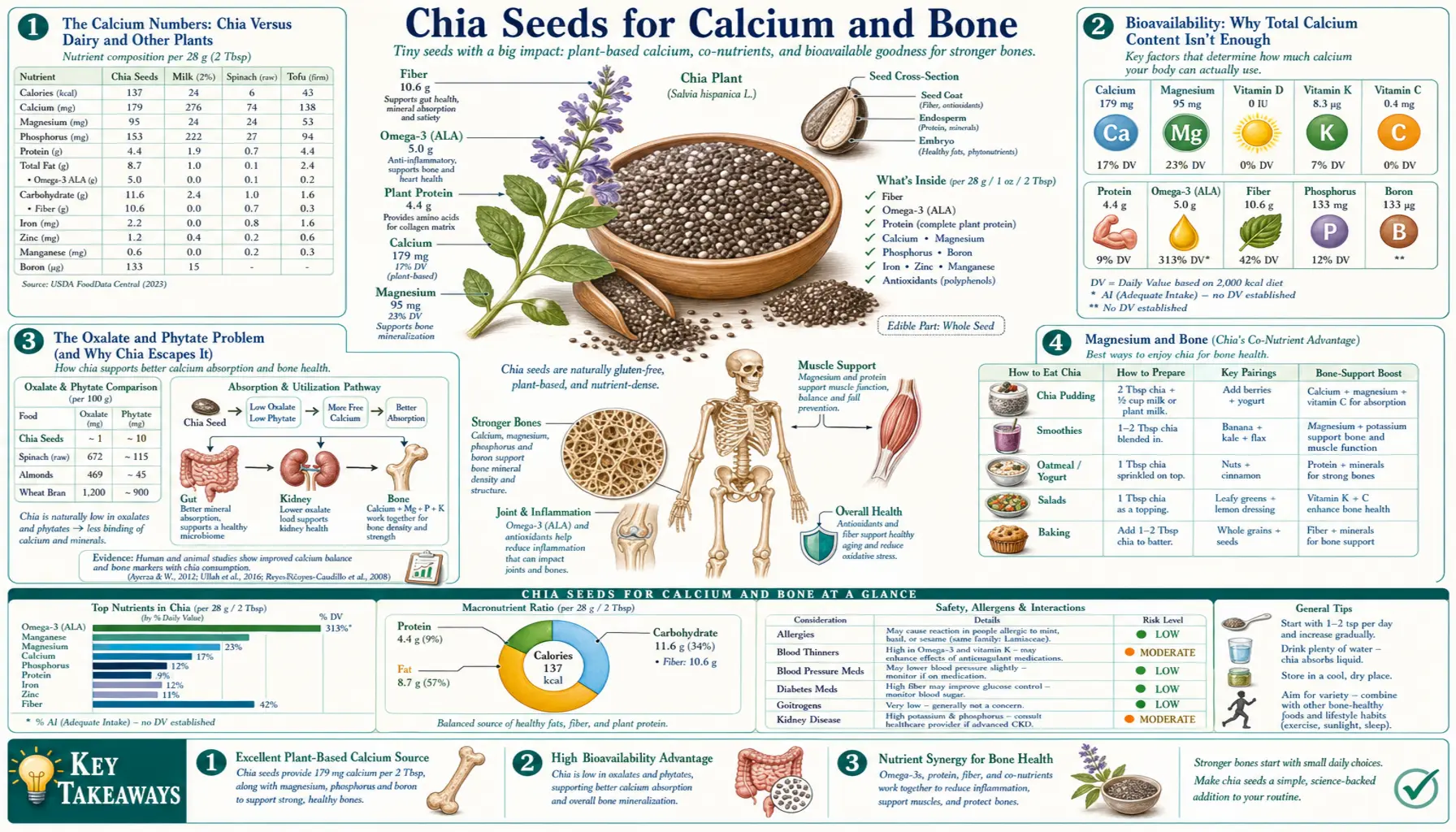
Chia seeds contain 631 mg of calcium per 100 g — substantially more than cow's milk (123 mg per 100 g) on a weight basis. A 28 g serving delivers 177 mg of calcium, roughly the same as 5 oz of milk or 1.5 oz of cheddar. More importantly, the calcium in chia is biologically available, in contrast to other high-calcium plant foods like spinach (where oxalate binding renders 95% of the calcium unabsorbable) or unfortified almonds (where phytate similarly impairs absorption). Chia is low in oxalate, modest in phytate, and rich in co-nutrients that support calcium utilization: magnesium (335 mg per 100 g), phosphorus (860 mg per 100 g), and trace boron. For patients pursuing a dairy-free diet for ethical, lactose-intolerance, allergy, or autoimmune reasons, chia is one of the most practical whole-food sources of bioavailable calcium. This page covers the bioavailability calculation in detail, the role of magnesium and boron in bone metabolism, the calcium-Vitamin-D-Vitamin-K2 triumvirate that determines whether dietary calcium actually deposits in bone, and the practical positioning of chia within a complete bone-health strategy.
Table of Contents
- The Calcium Numbers: Chia Versus Dairy and Other Plants
- Bioavailability: Why Total Calcium Content Isn't Enough
- The Oxalate and Phytate Problem (and Why Chia Escapes It)
- Magnesium and Bone (Chia's Co-Nutrient Advantage)
- Boron, Manganese, and the Trace-Mineral Picture
- The Calcium-Vitamin-D-Vitamin-K2 Triumvirate
- Plant Protein and Bone (the Old "Acidic" Hypothesis Revisited)
- Calcium for Dairy-Free Diets (Vegan, Vegetarian, Lactose-Intolerant)
- Osteoporosis Prevention and Management
- Why Food-Source Calcium Beats Supplemental Calcium
- Practical Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Calcium Numbers: Chia Versus Dairy and Other Plants
Per 100 g of food (raw, edible portion):
- Chia seeds: 631 mg calcium
- Sesame seeds (with hulls): 975 mg calcium — but most of this is in the hull as calcium oxalate, largely unavailable
- Sesame seeds (hulled, tahini): 426 mg calcium — more bioavailable than hulled sesame
- Sardines (with bones): 382 mg calcium — highly bioavailable
- Tofu (calcium-set firm): 350 mg calcium — bioavailable, but depends on the coagulant used; calcium sulfate set tofu has more
- Almonds: 264 mg calcium — partially blocked by phytate
- Kale (cooked): 150 mg calcium — low oxalate, highly bioavailable (~50%)
- Bok choy (cooked): 105 mg calcium — low oxalate, highly bioavailable
- Cow's milk (2%): 122 mg calcium per 100 g — bioavailability ~32%
- Cheddar cheese: 721 mg calcium — but per typical serving (28 g) only ~200 mg
- Greek yogurt (plain): 110 mg calcium — bioavailability ~32%
- Spinach (cooked): 136 mg calcium — bioavailability only ~5% due to oxalate
The DRI (Dietary Reference Intake) for adult calcium is 1,000 mg/day (men and women 19-50), increasing to 1,200 mg/day for women over 50 and men over 70. Adolescents 9-18 need 1,300 mg/day. Per-serving math:
- 28 g chia = 177 mg calcium (~14-18% DRI)
- 8 oz milk = 290 mg calcium (~24-29% DRI)
- 6 oz Greek yogurt = 190 mg calcium
- 1 oz cheddar = 200 mg calcium
- 3.75 oz sardines = 350 mg calcium
- 1 cup cooked kale = 95 mg calcium
For a person consuming 1,000 mg/day calcium target, chia alone is not enough — even at a generous 56 g daily serving it provides 350 mg, or about 35% of target. The role of chia is therefore as a high-impact contributor within a varied calcium-source diet, not as a sole source. Most plant-based eaters benefit from combining chia with calcium-set tofu, leafy greens (kale, bok choy, collards), small bony fish if not strictly vegan, calcium-fortified plant milks, and modest amounts of almonds or sesame.
Bioavailability: Why Total Calcium Content Isn't Enough
Total dietary calcium and absorbed calcium are not the same. Calcium absorption from food depends on multiple factors:
- Solubility in the upper gut — calcium must be in ionized form (Ca²⁺) to be absorbed. Calcium bound tightly to oxalate or phytate forms insoluble complexes that pass through the gut without absorption.
- Vitamin D status — active 1,25-dihydroxyvitamin D upregulates the intestinal calcium transport machinery (TRPV6 calcium channel, calbindin-D9k, and PMCA1b pump). Vitamin-D-deficient individuals absorb 10-15% of dietary calcium; replete individuals absorb 30-40%.
- Acid environment in the stomach and proximal duodenum — gastric acid is required to dissociate calcium from food matrices. Elderly patients with achlorhydria, and patients on chronic proton-pump inhibitors, absorb calcium poorly.
- Co-ingested nutrients — certain amino acids (particularly lysine) enhance calcium absorption modestly. High dietary fat decreases absorption (calcium soaps form in the gut lumen). High dietary fiber has a small inhibitory effect on absorption fraction, although the much higher absolute calcium content of high-fiber foods often compensates.
- Sodium and protein intake — both increase urinary calcium loss; their net effect on calcium balance depends on whether dietary calcium intake is adequate to compensate.
The bioavailability percentages typically used in calcium-source comparison:
- Cow's milk: ~32%
- Cheese: ~32%
- Calcium-set tofu: ~31%
- Calcium-fortified soy milk or almond milk: ~30%
- Kale, bok choy, broccoli: ~50% (the highest of any food due to low oxalate)
- Chia seeds: estimated ~25-30% (similar to dairy, based on limited direct measurement studies)
- Calcium carbonate supplement (Tums, Caltrate): ~20% on an empty stomach, ~30% with meals
- Calcium citrate supplement: ~24% with or without meals
- Spinach: ~5% (oxalate blockade)
- Wheat bran: ~38% (despite the phytate, the high content compensates)
So a 28 g chia serving delivering 177 mg calcium at ~25-30% bioavailability yields ~45-53 mg absorbed calcium — comparable to the absorbed calcium from 4-5 oz of cow's milk. The actual numbers vary with the individual's Vitamin D status, gastric acidity, and overall diet composition.
The Oxalate and Phytate Problem (and Why Chia Escapes It)
Two anti-nutrients are responsible for most of the calcium-bioavailability problems in plant foods:
Oxalate (oxalic acid) binds to calcium in the gut to form calcium oxalate, an insoluble crystal that is excreted in feces. Spinach is the classic example: it contains 970 mg oxalate per 100 g (one of the highest concentrations in any food), which is enough to bind almost all of the spinach's own calcium plus calcium from other foods eaten in the same meal. Other high-oxalate foods include:
- Rhubarb: 860 mg/100 g
- Beet greens: 610 mg/100 g
- Swiss chard: 645 mg/100 g
- Almonds: 469 mg/100 g
- Cocoa powder: 623 mg/100 g
- Cashews: 262 mg/100 g
Chia seeds contain approximately 30-50 mg of oxalate per 100 g, an order of magnitude lower than spinach and low enough that it does not meaningfully impair calcium absorption from chia itself.
Phytate (phytic acid, inositol hexakisphosphate) is the storage form of phosphorus in seeds and grains. It binds divalent cations including calcium, iron, zinc, and magnesium, reducing their absorption. Phytate content of common foods:
- Wheat bran: 2,000-4,000 mg/100 g
- Sesame seeds: 1,400 mg/100 g
- Almonds: 1,300-3,200 mg/100 g
- Soybeans: 1,400 mg/100 g
- Brown rice: 700 mg/100 g
- Chia seeds: ~700-800 mg/100 g — moderate, lower than other seeds and nuts
Phytate's effect on calcium absorption is real but modest, particularly when the food also contains substantial calcium (as chia does). The phytate content of chia is similar to many staple plant foods and is not high enough to be problematic. Soaking, sprouting, or fermenting chia further reduces phytate, though for most users this is not necessary.
The net effect is that chia's calcium is roughly as bioavailable as that in dairy, and substantially more bioavailable than the calcium in spinach, almonds, or whole grains.
Magnesium and Bone (Chia's Co-Nutrient Advantage)
Magnesium is the calcium of the soft tissues and a critical co-factor in bone metabolism. Approximately 60% of total body magnesium is in bone, where it serves both structural and regulatory roles:
- Approximately one-third of bone magnesium is in the hydroxyapatite crystal lattice, where it substitutes for calcium and influences crystal size and morphology
- The remaining two-thirds is on the crystal surface, where it serves as an exchangeable reservoir for serum magnesium regulation
- Magnesium is required for parathyroid hormone secretion and target tissue response — severe hypomagnesemia causes functional hypoparathyroidism and hypocalcemia even with adequate dietary calcium
- Magnesium is required for the renal 1-alpha-hydroxylase that converts 25-hydroxyvitamin D to active 1,25-dihydroxyvitamin D
- Magnesium is required for the enzymes that convert dietary Vitamin D to its active form and Vitamin K to its active form in the carboxylation reactions
The clinical consequence of magnesium deficiency for bone is significant. Observational studies consistently show lower bone mineral density and higher fracture risk in individuals with low dietary magnesium intake. The Women's Health Initiative and other large cohorts have found 27-44% higher fracture risk in the lowest magnesium intake quintile compared to the highest.
Chia's 335 mg of magnesium per 100 g is one of the highest natural concentrations in any commonly consumed food. A 28 g serving provides 94 mg magnesium, or about 25% of the RDA (320 mg for adult women, 420 mg for adult men). Other top food sources:
- Pumpkin seeds: 535 mg/100 g
- Brazil nuts: 376 mg/100 g
- Chia seeds: 335 mg/100 g
- Almonds: 270 mg/100 g
- Cashews: 260 mg/100 g
- Dark chocolate (70%+ cocoa): 228 mg/100 g
- Black beans (cooked): 70 mg/100 g
- Spinach (cooked): 87 mg/100 g
Crucially, magnesium intake in the modern Western diet is consistently below the RDA. The NHANES survey data suggest 50-60% of US adults consume below the EAR (Estimated Average Requirement). Chia is therefore valuable not just for its calcium content but for its magnesium content — addressing the bone-health-relevant deficiency that is more common than calcium deficiency in developed-country diets.
For more on magnesium specifically, see our Magnesium page.
Boron, Manganese, and the Trace-Mineral Picture
Bone metabolism depends on more than calcium, magnesium, and Vitamin D. Several trace minerals play under-appreciated supporting roles:
Boron at intakes of 3 mg/day or more has been shown to reduce urinary calcium loss by approximately 44%, raise serum 17-beta-estradiol modestly (in both men and women), and improve mental alertness markers. The Nielsen 2008 review (Nutrition Reviews) summarized the evidence. Most US adults consume less than 1 mg/day of boron from food. Chia provides modest amounts (estimated 1-2 mg/100 g), making it a meaningful contributor to boron intake.
Manganese is a co-factor for the glycosyltransferase enzymes that synthesize the proteoglycans in cartilage and bone matrix. Deficient animals develop skeletal deformities. Most Western diets contain adequate manganese (1.8-2.3 mg/day for adults), but whole grains, nuts, and seeds (including chia at 2.7 mg/100 g) are major sources. Refined grain diets can produce subclinical manganese inadequacy.
Phosphorus is the other major mineral component of bone (hydroxyapatite is calcium phosphate). Most modern diets contain abundant phosphorus, partly because of phosphate additives in processed foods. Phosphorus excess (relative to calcium) may actually worsen bone health by triggering parathyroid hormone elevation. Chia contains 860 mg phosphorus per 100 g, which sounds high but is balanced by the seed's substantial calcium content (the calcium:phosphorus ratio is approximately 0.7, which is acceptable; chronic ratios below 0.5 are concerning for bone). The phosphorus from chia is partially bound to phytate, which reduces its absorption to approximately 30-50%.
Zinc is required for osteoblast function and for the alkaline phosphatase enzyme involved in bone mineralization. Chia provides 4.6 mg/100 g (about 12% RDA per serving), a useful contribution but not a primary zinc source (oysters, beef, and pumpkin seeds are richer).
Silicon may influence bone formation; the data are less clear. Chia contains moderate amounts as part of its overall mineral profile.
The aggregate picture is that chia delivers a comprehensive package of bone-relevant minerals in a single food, complementing its calcium content rather than relying on calcium alone. This is the broader strategic value of food-source nutrition versus single-nutrient supplementation: bone is a tissue requiring a coordinated nutrient delivery, not a calcium-monosolution.
The Calcium-Vitamin-D-Vitamin-K2 Triumvirate
Calcium ingested with the diet faces a fork in the road: it can deposit in bone (where it is beneficial) or in soft tissue including arteries (where it is harmful). The directional decision is made by two Vitamins:
Vitamin D (cholecalciferol or D3, ideally) determines how much calcium is absorbed from the gut. With low Vitamin D status, calcium absorption is ~10-15% of intake; with adequate Vitamin D (serum 25-OH-D above 30 ng/mL), absorption rises to ~30-40%. Without adequate Vitamin D, even generous dietary calcium produces inadequate serum calcium, the body compensates by mobilizing calcium from bone via parathyroid hormone, and net bone mineral density falls despite adequate intake.
Vitamin K2 (menaquinone, particularly MK-4 and MK-7) activates two key calcium-handling proteins:
- Osteocalcin — produced by osteoblasts, requires Vitamin K-dependent carboxylation to bind calcium and incorporate it into bone matrix. Under-carboxylated osteocalcin (a marker of K2 deficiency) predicts higher fracture risk.
- Matrix Gla protein (MGP) — produced in vascular smooth muscle, requires Vitamin K-dependent carboxylation to bind calcium and prevent its deposition in arterial walls. Under-carboxylated MGP is a strong predictor of vascular calcification and coronary events.
Without adequate K2, calcium tends to deposit in soft tissue (arteries, kidneys) rather than bone. The Rotterdam Study showed that the highest tertile of dietary K2 intake was associated with 41% lower coronary heart disease and 36% lower all-cause mortality versus the lowest tertile.
This is why simply taking calcium supplements without attention to Vitamin D and K2 may not improve bone health and may increase cardiovascular risk — the Bolland 2010 meta-analysis raised concern about modest excess myocardial infarction risk from isolated calcium supplementation. The likely mechanism: in K2-deficient individuals, supplemental calcium deposits preferentially in arteries rather than bone.
Chia provides calcium and magnesium but is not a meaningful source of Vitamin D or Vitamin K2. The chia-based bone-health strategy therefore requires complementation with:
- Vitamin D3 from sunlight exposure, fatty fish, egg yolks, or supplementation (typical adult dose 2,000-4,000 IU/day, adjusted to serum 25-OH-D)
- Vitamin K2 from natto (the richest dietary source by far), aged cheeses, egg yolks, organ meats, or supplementation (typical dose 100-200 mcg/day MK-7)
The chia + D3 + K2 + leafy greens + adequate protein combination is the modern updating of the older calcium-and-Vitamin-D bone-health advice, and produces substantially better outcomes than calcium alone.
For more, see our Vitamin D3 page and Vitamin K2 page.
Plant Protein and Bone (the Old "Acidic" Hypothesis Revisited)
For decades, the prevailing view was that high dietary protein, especially from animal sources, increased urinary calcium loss and accelerated bone loss. This was the basis for the "acid-ash" hypothesis: animal proteins are metabolized to sulfuric acid (from sulfur-containing amino acids cysteine and methionine), the body buffers the acid with bone mineral, and the resulting calcium is excreted in urine.
The hypothesis has not held up. Recent prospective cohort studies and randomized trials have shown:
- Higher protein intake (including animal protein) is associated with higher bone mineral density, not lower
- The increased urinary calcium is fully matched by increased intestinal calcium absorption (driven by protein-induced IGF-1 production)
- Inadequate protein intake is a much larger bone-health risk than excess protein, particularly in elderly populations
- Hip fracture rates are higher in low-protein populations and in elderly patients with low albumin
Chia delivers 16.5 g of complete protein per 100 g, or about 4.7 g per 28 g serving. This is a meaningful contribution to the modern RDA of 0.8 g/kg body weight (typically 50-70 g/day for adults), and a particularly important contribution for plant-based eaters who may struggle to reach adequate protein intake from grains, legumes, and vegetables alone.
The chia protein contains all nine essential amino acids, with lysine being the limiting amino acid (typical of seed proteins). For a complete amino acid profile, chia pairs well with legumes (lentils, beans, peas), which are lysine-rich but typically methionine-limited — the two protein sources are mutually complementary, as has been understood since the work of Lappe in the 1970s.
Calcium for Dairy-Free Diets (Vegan, Vegetarian, Lactose-Intolerant)
Roughly 65% of the global adult population is lactose intolerant to some degree, and an increasing fraction of the developed-world population avoids dairy for ethical (vegan), allergy (cow's milk protein allergy), autoimmune (some practitioners recommend dairy elimination for Hashimoto's thyroiditis, rheumatoid arthritis, MS), or aesthetic (skin concerns) reasons. For all of these populations, reaching the 1,000-1,200 mg daily calcium target without dairy requires deliberate planning.
A representative dairy-free calcium-adequate daily meal pattern:
- 1 cup calcium-fortified almond or soy milk in coffee or smoothie: 300 mg
- 2 tablespoons chia (28 g): 177 mg
- 2 cups cooked kale or bok choy: 180 mg
- 4 oz calcium-set firm tofu: 350 mg
- 1/4 cup sesame seeds or 2 tablespoons tahini: 280 mg
- Total: ~1,290 mg (above the higher 1,200 mg target)
Without dairy, calcium intake at this level requires conscious sourcing. The combination of chia, calcium-fortified plant milks, leafy greens, calcium-set tofu, and small bony fish (sardines, anchovies if not strictly vegan) reliably reaches target. Almond consumption helps but is not a primary calcium source — 1 oz almonds provides only 76 mg.
Calcium-fortified plant milks deserve specific mention. Most are fortified with calcium carbonate or tricalcium phosphate at approximately 30-45% of the daily value per 8 oz serving (300-450 mg). The fortified calcium is absorbed at roughly the same efficiency as the calcium in cow's milk (~30-32%). Critically, the calcium settles to the bottom of the container during storage — shake or stir the carton vigorously before pouring to avoid drinking calcium-poor milk from the top.
For more dairy-free calcium strategies, see our Calcium page.
Osteoporosis Prevention and Management
Osteoporosis is a disease of microarchitectural deterioration in bone tissue, leading to increased fragility and fracture risk. It affects an estimated 200 million women globally and 50 million men. Lifetime fracture risk in a 50-year-old woman exceeds 50% for at least one osteoporotic fracture (hip, vertebral, wrist). Hip fractures specifically carry approximately 20% one-year mortality and impose massive morbidity.
Prevention and management require a comprehensive nutrient-plus-mechanical-loading strategy:
- Adequate calcium intake (1,000-1,200 mg/day from food preferentially)
- Adequate Vitamin D status (serum 25-OH-D above 30 ng/mL, typically requiring 2,000-4,000 IU/day supplementation)
- Adequate Vitamin K2 (100-200 mcg/day MK-7, or dietary intake of natto, aged cheeses, egg yolks)
- Adequate magnesium (300-400 mg/day — chia is a leading source)
- Adequate protein (at least 1.0-1.2 g/kg body weight for older adults; particularly important post-menopause)
- Weight-bearing and resistance exercise (the mechanical-loading stimulus is non-negotiable; even maximal nutrient intake without mechanical loading does not build bone)
- Avoidance of bone-toxic factors (smoking, excess alcohol, glucocorticoid medications when possible)
- Treatment of relevant comorbidities (hyperparathyroidism, hyperthyroidism, malabsorption syndromes)
Within this framework, chia is a useful contributor of calcium, magnesium, protein, and ALA (the omega-3 anti-inflammatory effect may have additional benefit in osteoporosis). A daily 28 g serving fits cleanly into the overall plan and supports multiple components simultaneously.
For patients with established osteoporosis (T-score below -2.5), pharmacologic treatment (bisphosphonates, denosumab, anabolic agents like teriparatide or romosozumab) is the foundation of management. Diet, exercise, and Vitamin D/K2 are essential adjuncts but do not substitute for pharmacotherapy in established disease.
For more on osteoporosis specifically, see our Osteoporosis page.
Why Food-Source Calcium Beats Supplemental Calcium
The Bolland 2010 meta-analysis (BMJ) raised serious concern about supplemental calcium, finding approximately 30% higher risk of myocardial infarction in patients taking calcium supplements without concurrent Vitamin D. The Women's Health Initiative did not find similar harm with calcium plus Vitamin D, and the issue remains controversial. But several mechanisms support the concern:
- Supplemental calcium delivers a large bolus — a typical 600 mg calcium pill produces a brief but pronounced rise in serum calcium that does not occur with food-distributed calcium
- That brief bolus may favor soft-tissue calcification — if Vitamin K2 status is inadequate to direct calcium to bone, the excess transient serum calcium may deposit in arteries
- Food-source calcium is delivered more gradually over the course of digestion, producing more sustained but lower-magnitude serum calcium changes that are better integrated with bone metabolism
- Food calcium comes packaged with co-nutrients (magnesium, phosphorus, protein, K2 in some cases) that support its appropriate utilization
The clinical inference is that food-source calcium from chia, leafy greens, calcium-set tofu, dairy (if consumed), and small bony fish is preferable to supplemental calcium pills wherever achievable. Supplements remain useful in specific contexts: severe lactose intolerance combined with low plant-source calcium intake, post-gastric-bypass malabsorption, and confirmed osteoporosis where pharmacotherapy is being initiated. For most healthy adults, hitting the calcium target with whole foods is both more effective and safer.
Practical Protocol
Bone-health-focused chia protocol:
- Daily dose: 28-35 g chia (1-1.25 oz), delivering 177-220 mg calcium and 94-117 mg magnesium
- Combine with: Vitamin D3 2,000-4,000 IU/day, Vitamin K2 (MK-7) 100-200 mcg/day, leafy greens at most meals, calcium-set tofu or calcium-fortified plant milk if not dairy-eating
- Time of day: any; for those with low gastric acid, take chia with a meal containing some acidity (citrus, tomatoes, vinegar) to support calcium dissolution
- Pair with: weight-bearing and resistance exercise at least 3 times per week (the mechanical stimulus that converts dietary calcium into bone)
- Form: whole or ground chia work equivalently for calcium delivery
- Avoid: high-oxalate foods (spinach, rhubarb, large amounts of almonds or cocoa) eaten in the same meal as your calcium-rich foods, to avoid binding free calcium
Sample bone-health-optimized day:
- Breakfast: Chia pudding made with 3 tablespoons chia in 1 cup calcium-fortified almond milk, topped with berries and ground walnuts (Ca: ~600 mg)
- Lunch: Large kale-and-quinoa salad with 4 oz baked salmon, tahini dressing, lemon (Ca: ~400 mg)
- Dinner: Stir-fried bok choy and broccoli over 4 oz calcium-set tofu, brown rice (Ca: ~600 mg)
- Snack: 1 oz cheese OR 1/4 cup sesame seeds OR a small piece of natto (for K2)
- Total calcium: ~1,600 mg from food sources, well above the 1,200 mg target
- Magnesium total: ~600 mg, above RDA
Cautions
- Kidney stone history — for patients with calcium oxalate stones (the most common type), the medical guidance has shifted from low-calcium diets (which paradoxically increased stones by allowing more dietary oxalate to be absorbed) to adequate dietary calcium plus reduced oxalate. Chia is low in oxalate and high in calcium, making it actually favorable for calcium-oxalate stone prevention when consumed with meals.
- Hypercalcemia from medical conditions — patients with primary hyperparathyroidism, sarcoidosis, lymphoma, multiple myeloma, or other conditions producing hypercalcemia should not deliberately increase calcium intake without medical supervision.
- Lithium therapy — high-dose calcium can complicate lithium pharmacokinetics; coordinate with prescribing psychiatrist if increasing dietary calcium substantially.
- Quinolone and tetracycline antibiotics — calcium chelates these antibiotics in the gut, reducing absorption. Separate chia intake by at least 2 hours from these medications.
- Levothyroxine — calcium and other minerals impair levothyroxine absorption. Take levothyroxine on empty stomach 30-60 minutes before chia or any calcium-containing food.
- Iron supplements — calcium can reduce iron absorption when taken in the same meal. Separate by at least 2 hours if both are being supplemented.
Key Research Papers
- Capitani MI et al. (2012). Physicochemical and functional characterization of by-products from chia seeds. LWT - Food Science and Technology. — Search PubMed
- Heaney RP et al. (1988). Calcium absorbability from spinach. American Journal of Clinical Nutrition. — Search PubMed
- Weaver CM, Heaney RP (eds.) (2006). Calcium in Human Health. Humana Press. PubMed: Weaver/Heaney calcium
- Ross AC et al. (2011). The 2011 Dietary Reference Intakes for Calcium and Vitamin D from the IOM. JCEM. — PubMed (doi:10.1210/jc.2010-2704)
- Bolland MJ et al. (2010). Effect of calcium supplements on risk of myocardial infarction and cardiovascular events. BMJ. — PubMed (doi:10.1136/bmj.c3691)
- Rude RK et al. (2009). Skeletal and hormonal effects of magnesium deficiency. JACN. — PubMed (doi:10.1080/07315724.2009.10719764)
- Nielsen FH (2008). Is boron nutritionally relevant? Nutrition Reviews. — Search PubMed
- Geleijnse JM et al. (2004). Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study. Journal of Nutrition. — PubMed (doi:10.1093/jn/134.11.3100)
- Beulens JWJ et al. (2009). High dietary menaquinone intake is associated with reduced coronary calcification. Atherosclerosis. — Search PubMed
- Welch AA et al. (2007). Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries (EPIC). Eur J Clin Nutr. — Search PubMed
- Tang AL et al. (2010). Calcium absorption in Australian osteopenic post-menopausal women: an acute comparative study of fortified soymilk to cows' milk. APJCN. — Search PubMed
- Kulczynski B et al. (2019). The chemical composition and nutritional value of chia seeds. Nutrients. — Search PubMed
PubMed Topic Searches
- PubMed: Chia calcium bioavailability
- PubMed: Ca + D + K2 bone
- PubMed: Plant-based calcium bone density
- PubMed: Magnesium bone density fracture
- PubMed: Oxalate phytate calcium
Connections
- Chia Seeds Overview
- Chia Seeds Benefits Hub
- Chia for ALA Omega-3
- Chia for Blood Sugar
- Chia for Hydration and Endurance
- Calcium
- Magnesium
- Boron
- Vitamin D3
- Vitamin K2
- Osteoporosis
- Kale
- Sardines
- Yogurt
- All Food