Lupus: History and Discovery
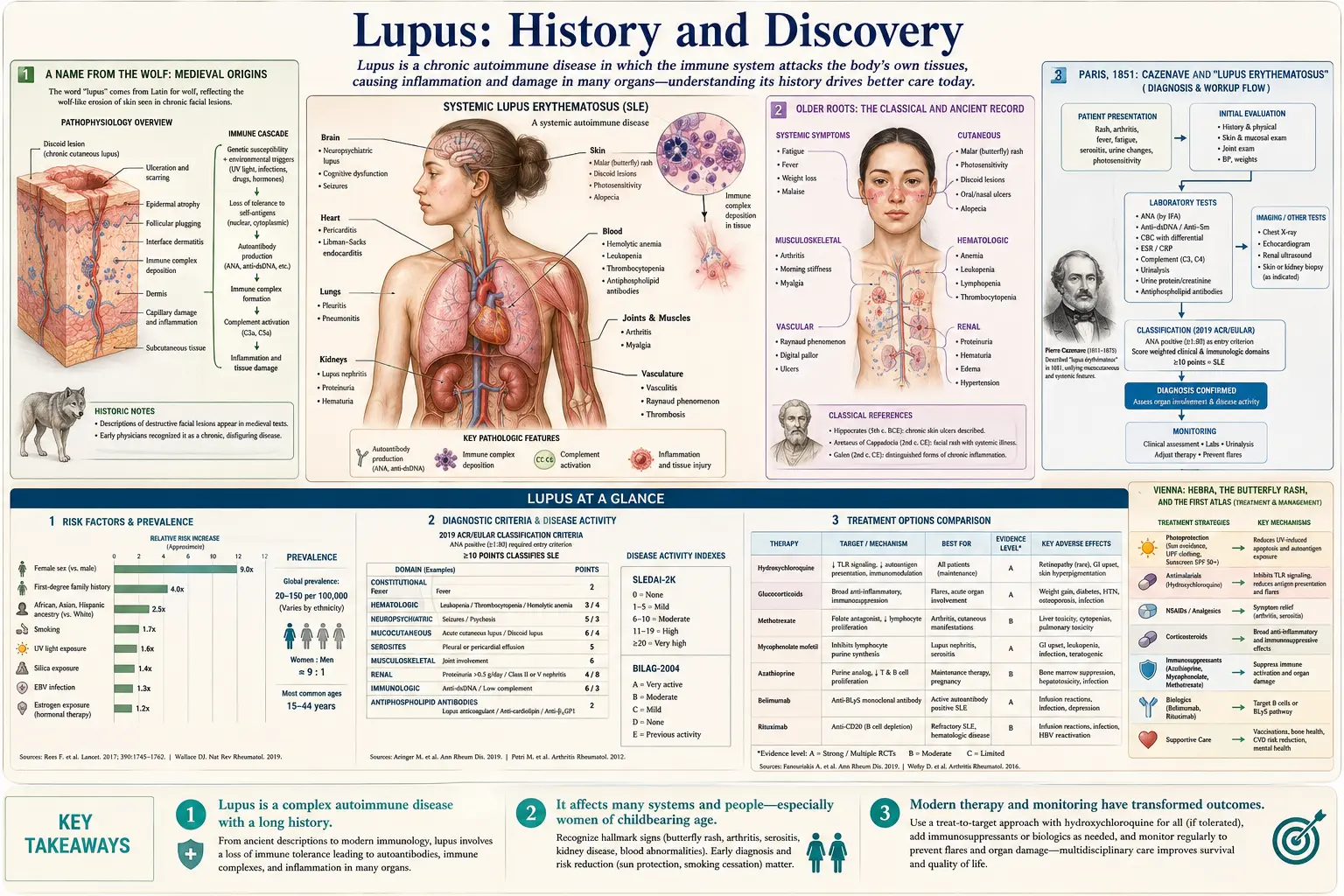
The story of lupus is a story of a name that traveled, slowly, from a description of a wound to a description of a disease of the whole body. The Latin word lupus means “wolf,” and in the Middle Ages physicians used it for destructive, eroding sores of the face — lesions that, in the imagination of the time, looked as if a wolf had bitten the skin. For roughly seven centuries that word meant only a skin problem. It took the work of nineteenth-century dermatologists in Paris and Vienna, the clinical eye of William Osler in Baltimore, and finally a single discovery at the Mayo Clinic in 1948 — the “LE cell” — to reveal that lupus is not a disease of the skin that sometimes harms the body, but an autoimmune disease of the body that often shows on the skin. This page traces that journey, naming who described what, and when, and taking care to distinguish a name from a first description from the discovery of a cause or a marker.
Table of Contents
- A Name from the Wolf: Medieval Origins
- Older Roots: The Classical and Ancient Record
- Paris, 1851: Cazenave and “Lupus Erythematosus”
- Vienna: Hebra, the Butterfly Rash, and the First Atlas
- Kaposi, 1872: Lupus as a Systemic Disease
- William Osler and the Visceral Manifestations
- The LE Cell, 1948: The Immunological Era Begins
- From the LE Cell to ANA and Anti-DNA Antibodies
- A Note on the History of Treatment
- Research Papers and References
- Connections
- Featured Videos
A Name from the Wolf: Medieval Origins
The name we still use comes from a vivid, frightening image. Lupus is simply the Latin for wolf, and medieval physicians applied it to ulcerating, destructive sores on the face — lesions that ate away at the skin and were popularly likened either to the bite of a wolf or, in another reading, to the dark mask of fur around a wolf’s muzzle. The attribution most often cited is to Rogerius (Roger Frugardi of Salerno and his school), a surgical writer usually dated to the late twelfth and thirteenth centuries, who is credited with using lupus for these eroding facial lesions. It is important to be precise here: this is a naming, not a discovery of the disease. In the medieval and early-modern period, “lupus” was a loose, descriptive label for any gnawing, ulcerating skin condition — it could include what we would now call cutaneous tuberculosis (lupus vulgaris), skin cancers, and other destructive sores, not only the disease we mean today.
This matters because it explains a persistent source of confusion in old texts. When a writer before the nineteenth century says “lupus,” we usually cannot be sure which modern disease is meant. The word marked an appearance — a wolf-bitten face — rather than an identified illness with a known cause. The disease that modern medicine calls lupus erythematosus had to be carved out of this older, broader category by careful clinical observers, and that work did not really begin until physicians started to classify skin diseases systematically in the early 1800s.
So the wolf gave lupus its haunting name centuries before anyone understood what the condition was, where it came from, or that it could reach far beyond the skin. The name endured; the meaning narrowed and deepened around it.
Older Roots: The Classical and Ancient Record
Historians of medicine often divide the history of lupus into three periods — classical, neoclassical, and modern — and the classical period reaches back, in a loose sense, to antiquity. Hippocrates (c. 460–c. 370 BCE) is frequently credited with describing destructive skin ulceration under the Greek term herpes esthiomenos, meaning roughly “gnawing” or “eating” skin disease. This should be read with caution: such a description records an appearance of eroding skin, not a diagnosis of lupus erythematosus as we define it, and many conditions could produce a gnawing ulcer. It is offered here as the deep historical backdrop to the later name, not as evidence that the ancient Greeks knew the disease.
For accessibility, these ancient and medieval works are named in this article as historical primary sources rather than as modern citations — the original Hippocratic and Salernitan texts predate the scientific-paper era by many centuries. The reliable, well-documented history of lupus as a defined clinical entity begins much later, in the early nineteenth century, when European dermatology emerged as an organized field and physicians such as Robert Willan and his pupil Thomas Bateman in Britain began producing systematic classifications and illustrations of skin disease.
The honest summary is this: lupus has a long verbal prehistory but a comparatively short scientific one. The wolf-name is medieval; the recognizable clinical disease is a creation of the 1800s; and the understanding of its cause belongs almost entirely to the twentieth century. Keeping those layers distinct is the key to reading the history accurately.
Paris, 1851: Cazenave and “Lupus Erythematosus”
The first decisive step toward the modern disease was taken in Paris. Pierre Louis Alphonse Cazenave (1795–1877), a dermatologist who trained under Laurent Biett at the Hôpital Saint-Louis, is the figure usually credited with the term “lupus érythémateux” (lupus erythematosus), which he is recorded as introducing in 1851. Cazenave attached the qualifier erythematosus — “reddened” — to separate this particular red, scaling, scarring facial eruption from the other destructive conditions that had all been lumped together under the old word “lupus,” including the infectious skin tuberculosis (lupus vulgaris) with which it was easily confused.
A point of accuracy: Cazenave had described essentially the same lesions earlier under a different name. In the 1830s he and his colleagues used the label érythème centrifuge (“erythema centrifugum”) for the spreading, ringed facial eruption. The contribution dated to 1851 is specifically the naming “lupus erythematosus” — the term that has survived, in modified form, to the present day. What Cazenave described corresponds most closely to what we now call discoid (chronic cutaneous) lupus: a disease, as he understood it, of the skin.
Cazenave’s work belongs to a broader nineteenth-century achievement — the gradual separation of lupus erythematosus from the look-alike conditions around it. His teacher Biett, the British dermatologists Willan and Bateman, and the Vienna school that followed all contributed pieces of this disentangling. By the mid-1800s, then, lupus erythematosus existed as a named, recognizable skin disease. The far larger discovery — that it was not merely a skin disease — was still two decades away, and it would come from Vienna.
Vienna: Hebra, the Butterfly Rash, and the First Atlas
The Vienna school of dermatology, led by Ferdinand von Hebra (1816–1880), refined the clinical picture of lupus in ways that still shape how the disease is recognized today. Hebra is credited with describing, around 1846, the characteristic “butterfly” distribution of the facial rash — the way the redness spreads symmetrically across the cheeks and over the bridge of the nose, in a shape suggesting a butterfly’s wings. This malar or butterfly rash remains one of the most familiar signs of lupus and one of its classification criteria. Hebra is also credited with publishing some of the first illustrated depictions of the disease, in his Atlas of Skin Diseases (the relevant volume dated to the mid-1850s), giving physicians across Europe a visual reference for what lupus erythematosus actually looked like.
Hebra’s importance to this story is also institutional and personal: his clinic in Vienna trained the man who would make the single greatest conceptual leap in lupus before the twentieth century. Moriz Kaposi — born Moriz Kohn — was Hebra’s student and later his son-in-law, and he worked within the same Viennese tradition of careful, image-rich clinical observation. It was Kaposi who took the next, larger step.
At this stage of the history, then, two complementary descriptions were in place: Cazenave in Paris had given the disease its enduring name and characterized its discoid (skin-scarring) form, while Hebra in Vienna had pinned down the butterfly rash and produced the first atlas illustrations. Both men, however, still understood lupus erythematosus as fundamentally a disorder of the skin.
Kaposi, 1872: Lupus as a Systemic Disease
The pivotal recognition — that lupus is not confined to the skin — is credited to Moriz Kaposi in 1872. In a landmark publication usually rendered in English as New Contributions to the Knowledge of Lupus Erythematosus, Kaposi reported that some patients with the skin disease also suffered a cluster of internal, constitutional problems: fever, joint pain and arthritis, swollen lymph nodes (lymphadenopathy), weight loss, and anemia, sometimes with subcutaneous nodules. Crucially, he observed that these systemic symptoms could be grave and that the disease could, in serious cases, end in death.
From this, Kaposi drew the distinction that organizes lupus medicine to this day. He separated two forms: a discoid type that was essentially limited to the skin, and a disseminated (systemic) type in which the disease reached into the body and threatened internal organs. This was the conceptual birth of systemic lupus erythematosus as a distinct idea — the recognition that the wolf-named facial rash could be the visible surface of a far more dangerous, body-wide illness. Kaposi’s 1872 article was important enough to be translated into English (in 1880), carrying the insight beyond the German-speaking world.
It is worth stating precisely what Kaposi did and did not do. He recognized and described the systemic nature of lupus — that it can affect more than the skin. He did not discover its cause; the idea that lupus is an autoimmune disease, in which the immune system mistakenly attacks the body’s own tissues, lay nearly a century in the future and required tools (immunology, the concept of autoantibodies) that did not yet exist. Kaposi’s achievement was clinical and observational, and on that level it was profound: he changed lupus from a skin condition into a systemic disease in the minds of physicians.
William Osler and the Visceral Manifestations
The systemic concept that Kaposi opened was broadened and reinforced around the turn of the twentieth century, most influentially by the Canadian-born physician Sir William Osler (1849–1919), working at Johns Hopkins in Baltimore. Between 1895 and 1904, Osler published a series of papers on what he called the visceral (internal-organ) complications of the “erythema group” of skin diseases. His first paper, “On the visceral complications of erythema exudativum multiforme,” appeared in The American Journal of the Medical Sciences in 1895; a major follow-up in 1904 described a cohort of twenty-nine patients who had skin disease together with clear systemic or visceral involvement.
A careful caveat is needed, and the historical literature itself insists on it: not all of the patients in Osler’s “erythema group” series had what we would today diagnose as systemic lupus erythematosus — his category was broader than lupus alone. Nevertheless, Osler’s contribution was real and significant. He documented in detail how a disease that announces itself on the skin can attack the joints, kidneys, heart, and nervous system, and he helped establish the medical understanding — through his emphasis on the word and concept of systemic involvement — that lupus erythematosus belongs among the diseases that affect the whole body. His meticulous case descriptions of visceral involvement gave the systemic view clinical weight in the English-speaking medical world.
With Kaposi and Osler, the clinical picture of systemic lupus was essentially complete by the early 1900s: a disease that could scar the skin, paint a butterfly across the face, inflame the joints, damage the kidneys, and prove fatal. What remained entirely unknown was why. There was no laboratory test, no marker, and no theory of cause. That final, transforming chapter began in 1948.
The LE Cell, 1948: The Immunological Era Begins
The modern, immunological understanding of lupus was launched by a discovery at the Mayo Clinic in Rochester, Minnesota. In 1948, the hematologist Malcolm M. Hargraves, together with his colleagues Helen Richmond and Robert Morton, identified a strange cell in the bone marrow of lupus patients — a white blood cell that had engulfed the nuclear material of another cell. They named it the “LE cell” (lupus erythematosus cell). Their report, “Presentation of two bone marrow elements: the ‘tart’ cell and the ‘L.E.’ cell,” appeared in the Proceedings of the Staff Meetings of the Mayo Clinic in early 1948.
The significance of this finding is hard to overstate. For the first time, lupus had a laboratory marker — something a pathologist could see down a microscope that pointed to the diagnosis. Just as importantly, the LE-cell phenomenon hinted at the underlying mechanism. The reason a white cell was devouring another cell’s nucleus was that something in the patient’s blood was reacting against nuclear material. That “something” would soon be identified as an antibody directed against the body’s own cell nuclei — an autoantibody. In other words, the LE cell was the first concrete clue that lupus is an autoimmune disease, in which the immune system attacks self.
The LE-cell test became the standard laboratory aid for diagnosing systemic lupus for roughly a decade, and it reframed the entire disease. After 1948, lupus was no longer only a clinical picture to be recognized by eye; it was a problem of immunology to be investigated in the laboratory. The discovery effectively opened the “modern era” of lupus that historians describe — the era in which the cause, not just the appearance, finally came within reach.
From the LE Cell to ANA and Anti-DNA Antibodies
The clue offered by the LE cell was pursued quickly. Researchers reasoned that if a patient’s serum could provoke a white cell to attack a nucleus, the serum must contain antibodies against nuclear components — antinuclear antibodies (ANA). In 1957, George J. Friou applied the then-new technique of immunofluorescence to detect these antinuclear antibodies directly, developing the fluorescent ANA test. This was a major advance over the cumbersome LE-cell preparation: the immunofluorescent ANA test became, and for many decades remained, the principal screening test for lupus and related connective-tissue diseases. (The substrate was later standardized on cultured human HEp-2 cells, which came into wide use from the 1970s.)
The same period pinned down a more specific marker. Also in 1957, several groups independently demonstrated antibodies that react with DNA in the serum of lupus patients — work associated with names including Ceppellini, Polli and Celada; Robbins, Holman, Deicher and Kunkel; and Seligmann. Through the early and mid-1960s these observations were refined, and in 1966 Tan, Schur, Carr and Kunkel established that antibodies to native, double-stranded DNA (anti-dsDNA) are highly specific for systemic lupus and tend to track with disease activity. Anti-dsDNA remains one of the defining autoantibodies of the disease today and a core part of its diagnostic criteria.
This sequence — LE cell (1948) → fluorescent ANA test (1957) → anti-dsDNA antibodies (1957–1966) — is the spine of modern lupus diagnosis, and it firmly established the disease as autoimmune in origin. The detailed clinical use of these tests, including how ANA and anti-dsDNA are interpreted today, is covered in the companion deep-dive article on ANA, dsDNA, and Lupus Autoantibodies. The honest framing remains: the autoimmune mechanism — that the immune system makes antibodies against the patient’s own nuclei and DNA — is the established cause of the disease’s activity, while the deeper question of why a given person’s immune system turns against itself (the interplay of genetics, hormones, and environmental triggers) is still an area of active research rather than a settled answer.
A Note on the History of Treatment
The history of treating lupus runs partly in parallel with the history of understanding it, and two threads are well documented. The first is the antimalarial thread. In 1894, J. F. Payne reported that quinine — the antimalarial drug derived from cinchona bark — was useful in treating lupus, and the combination of quinine with salicylates was soon noted to help as well. This empirical observation, made long before anyone understood lupus as autoimmune, eventually flowered into the modern use of synthetic antimalarials: chloroquine and then hydroxychloroquine (Plaquenil), the latter approved by the U.S. Food and Drug Administration in the mid-1950s and now a cornerstone of long-term lupus management. The fuller story of these drugs is told in the deep-dive article on Hydroxychloroquine and Antimalarials.
The second thread is the corticosteroid revolution of the mid-twentieth century. The introduction of cortisone / corticosteroid therapy, associated with Philip Hench and colleagues at the Mayo Clinic around 1948–1950 (work for which Hench shared a Nobel Prize), transformed the treatment of severe inflammatory and autoimmune disease, lupus among them. For the first time, physicians could powerfully suppress the inflammation that damages organs in a lupus flare. Steroids remain central to managing serious disease, even as their long-term side effects have driven the search for gentler alternatives.
From these foundations the modern therapeutic era has grown, through broad immunosuppressants to today’s targeted biologic therapies. The arc of the whole history is striking: a medieval name drawn from a wolf, a nineteenth-century skin disease, a systemic illness recognized in Vienna and Baltimore, an autoimmune cause uncovered at the Mayo Clinic after 1948, and a widening set of treatments built on that understanding — each chapter a genuine, datable advance rather than a single eureka moment.
Research Papers and References
The references below combine peer-reviewed historical reviews with authoritative patient-facing histories and curated PubMed topic-search links. Ancient and medieval texts (the Hippocratic corpus; the writings attributed to Rogerius) are named in the article as historical primary sources rather than as modern citations. Each external link opens in a new tab.
- Smith CD, Cyr M. The history of lupus erythematosus: from Hippocrates to Osler. Rheumatic Disease Clinics of North America. 1988;14(1):1–14. — PubMed: 3041483
- Blackmore K, et al. The history of lupus throughout the ages. Journal of the American Academy of Dermatology. 2021. — doi:10.1016/j.jaad.2020.04.150
- Mallavarapu RK, Grimsley EW. The history of lupus erythematosus. Southern Medical Journal. — PubMed: history of lupus erythematosus (review)
- Holubar K, et al. Moriz Kaposi (1837–1902) and the systemic concept of lupus erythematosus. — PubMed: Kaposi and systemic lupus (1872)
- Hochberg MC. The place of William Osler in the description of systemic lupus erythematosus. — PMC2783313
- Osler W and the development of the concept of systemic lupus erythematosus. Seminars in Arthritis and Rheumatism. 1997. — PubMed: 9287390
- Hargraves MM, Richmond H, Morton R. Presentation of two bone marrow elements: the “tart” cell and the “L.E.” cell (Mayo Clinic, 1948). — PubMed: Hargraves LE cell (1948)
- Hepburn AL. The LE cell — historical review. Rheumatology (Oxford). 2001. — PubMed: LE cell historical review
- Friou GJ. Clinical application of a test for lupus globulin–nucleohistone interaction using fluorescent antibody (immunofluorescent ANA, 1957). — PMC2603909
- Pisetsky DS. Anti-DNA antibodies — quintessential biomarkers of SLE. Nature Reviews Rheumatology. 2016;12(2):102–110. — doi:10.1038/nrrheum.2015.151
- Rahman A, Isenberg DA. Systemic lupus erythematosus (review). New England Journal of Medicine. 2008;358(9):929–939. — doi:10.1056/NEJMra071297
- Wallace DJ. The history of treating lupus with antimalarials (Payne 1894 to hydroxychloroquine). — PubMed: antimalarials in lupus (history)
- Cazenave and the naming of lupus erythematosus (1851); discoid lupus history. — PubMed: Cazenave and lupus erythematosus
- Ferdinand von Hebra, the butterfly rash, and early dermatologic illustration of lupus. — PubMed: Hebra and the butterfly rash
External Authoritative Resources
- Lupus Foundation of America — The History of Lupus
- NIAMS (NIH) — Lupus Health Information
- PubMed — History of Systemic Lupus Erythematosus
Connections
- Rheumatology
- Lupus (Systemic Lupus Erythematosus) — Main Article
- ANA, dsDNA, and Lupus Autoantibodies
- Hydroxychloroquine and Antimalarials
- Cutaneous Lupus and Photoprotection
- Sjögren’s Syndrome
- Raynaud’s Disease
- Arthritis
- All Conditions