Wuchereria bancrofti (Lymphatic Filariasis)
Wuchereria bancrofti is a thread-like parasitic roundworm that lives inside the human lymphatic system — the network of vessels and glands that drains fluid from our tissues and helps run our immune defenses. It is the leading cause of lymphatic filariasis, and in its most severe form it produces the swollen, thickened limbs known as elephantiasis. Because the disease disfigures and disables some of the poorest people in the world, the World Health Organization counts it among the "neglected tropical diseases" and has targeted it for global elimination. This page explains, in plain language, what the parasite is, how a tiny worm carried by mosquitoes can cause such dramatic swelling, who is really at risk (long-term residents of endemic regions, not brief travelers), how the infection is found and treated, and why lymphatic filariasis is one of public health's genuinely hopeful stories.
Table of Contents
- What Is Wuchereria bancrofti?
- The Parasite and Its Life Cycle
- How Infection Happens
- Symptoms: From Silent Damage to Elephantiasis
- Tropical Pulmonary Eosinophilia
- Who Is Most at Risk
- Diagnosis
- Treatment
- Prevention and Global Elimination
- The Honest Bottom Line
- Key Research Papers
- Featured Videos
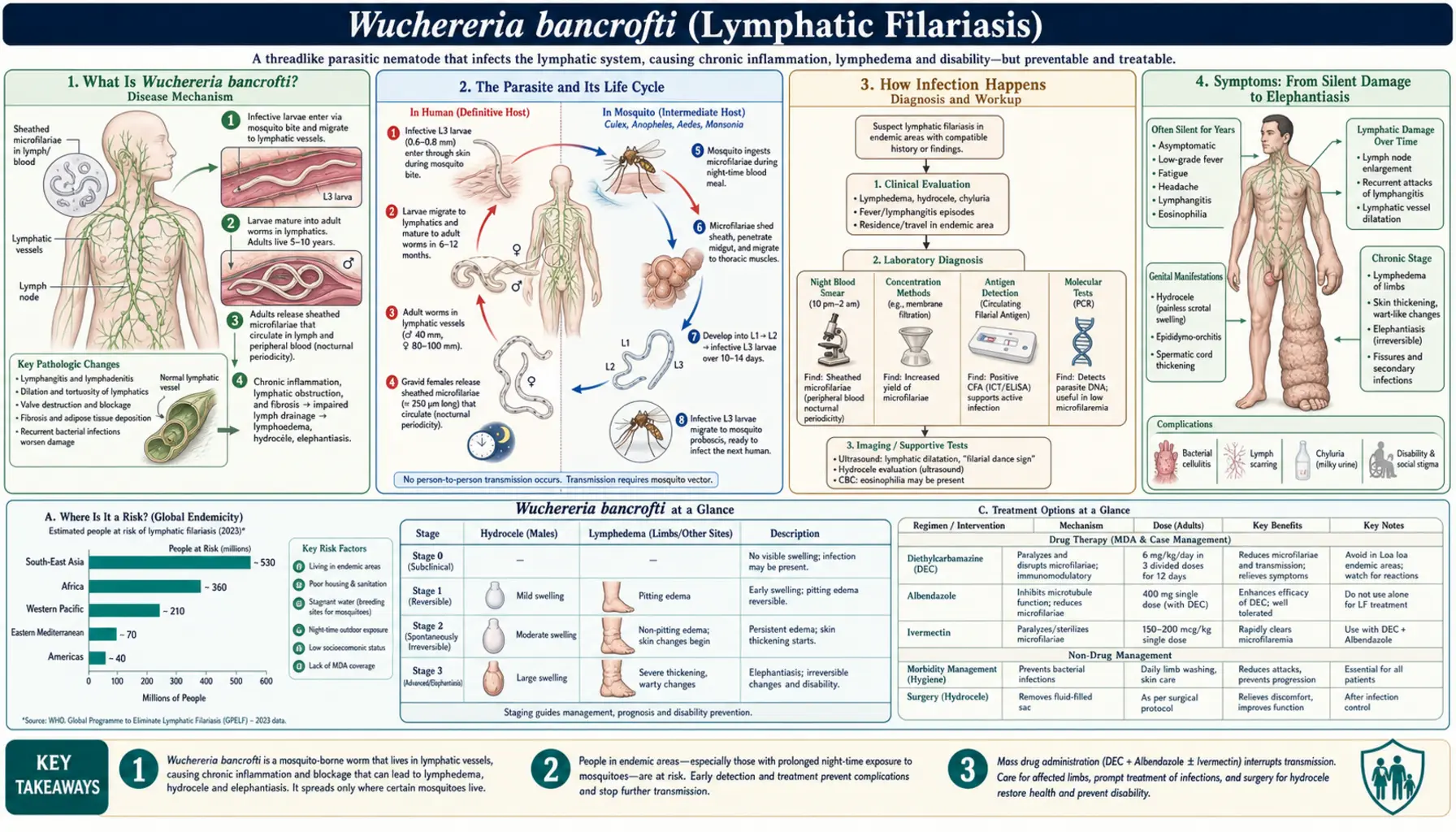
1. What Is Wuchereria bancrofti?
Wuchereria bancrofti is a filarial worm — a long, slender roundworm (nematode) named "filarial" because the adults are as fine as threads. Unlike the intestinal worms that live in the gut, filarial worms live deep in the body's tissues. W. bancrofti makes its home in the lymphatic vessels and lymph nodes, the plumbing that carries a clear fluid called lymph back toward the bloodstream and that houses much of the immune system. Damage to that plumbing is what makes this infection so distinctive and, over time, so disabling.
The illness these worms cause is called lymphatic filariasis. W. bancrofti is responsible for the large majority of cases worldwide — roughly nine in ten. Two closely related worms, Brugia malayi and Brugia timori, cause the rest and are found mainly in parts of Asia and the western Pacific. All three produce a similar disease, but W. bancrofti is by far the most widespread and is the only one that also commonly affects the male genitals.
Lymphatic filariasis is a disease of scale and of poverty. By the World Health Organization's estimates, roughly 51 million people were living with the infection as of 2018 — a large drop from an estimated 120 million around the year 2000 — while hundreds of millions more still live in places where transmission can occur. It is one of the WHO's neglected tropical diseases, so called because they persist among the world's poorest communities and have historically received little attention or funding. One hopeful biological fact underpins the whole elimination effort: for W. bancrofti, humans are essentially the only reservoir. The worm has no important animal host to hide in, so if transmission between people and mosquitoes can be interrupted for long enough, the parasite has nowhere left to go.
2. The Parasite and Its Life Cycle
The life of W. bancrofti plays out in two very different places: inside a human being and inside a mosquito. Understanding this back-and-forth explains almost everything about the disease.
Inside the human host, the adult worms live coiled together in the lymphatic vessels and nodes, usually in the legs, arms, or groin. They are long and thread-like — females can reach several centimeters — and they are surprisingly long-lived, surviving on the order of five to eight years. The adults are not what circulate in the blood. Instead, the females release enormous numbers of tiny larvae called microfilariae, thousands each day, which slip out of the lymphatics and travel in the bloodstream.
These microfilariae have a remarkable habit. In most parts of the world, they show nocturnal periodicity: they surge into the peripheral blood mainly at night, peaking roughly between 10 p.m. and 2 a.m., and largely disappear from the small vessels during the day. This nighttime rhythm is no accident — it is exquisitely matched to the biting schedule of the mosquitoes that carry the parasite, maximizing the chance that a feeding mosquito will pick them up. (In some Pacific island regions the local strain is "subperiodic," circulating more evenly through the day to match day-biting mosquitoes there.)
When a mosquito bites an infected person, it draws up microfilariae with the blood meal. Inside the mosquito, the larvae do not multiply, but they do develop — maturing over about one to two weeks into an infective stage that migrates to the insect's mouthparts. At the mosquito's next bite, these infective larvae are deposited onto the skin and crawl into the tiny wound. Once inside a new person, they travel to the lymphatic vessels and slowly grow into adult worms over the following months, and the cycle begins again. A crucial point follows from this: the worms do not reproduce and build up inside you the way bacteria do. Each mature adult comes from a separate infective bite, so a heavy worm burden reflects many, many bites over a long time — which is exactly why the serious disease is tied to years of exposure.
3. How Infection Happens
Lymphatic filariasis is spread entirely by the bite of an infected mosquito. It is not contagious in the everyday sense: you cannot catch it from touching, sharing food with, or living alongside an infected person, and it does not pass through water or soil. Several kinds of mosquito serve as vectors depending on the region — Culex mosquitoes are the main carriers in many urban areas of Asia and the Americas, Anopheles mosquitoes (the same genus that transmits malaria) carry it across much of rural Africa, and Aedes mosquitoes are important in parts of the Pacific.
The single most reassuring fact about transmission is how inefficient it is. Because the worms cannot multiply inside a person and each adult requires its own infective bite, acquiring a mature, disease-causing infection generally takes repeated bites over months to years — often many hundreds of infective bites accumulated through long residence in an endemic area. For this reason, lymphatic filariasis is fundamentally a disease of long-term residents of places where the parasite is common, not of short-term visitors. A tourist, aid worker, or business traveler spending days or weeks in an endemic region is at very low risk of developing the disease, even though avoiding mosquito bites is always sensible.
4. Symptoms: From Silent Damage to Elephantiasis
One of the hardest things to grasp about lymphatic filariasis is how enormously it varies. Two people carrying the same worms can look completely different — one apparently healthy, the other severely disabled. It helps to think of the disease as a spectrum.
Silent infection with hidden damage
A great many infected people have no outward symptoms at all. Yet "asymptomatic" does not mean "unharmed." Studies using ultrasound and other imaging have shown that even people who feel completely well often already have dilated, damaged lymphatic vessels where the adult worms live, and many have microscopic evidence of kidney irritation such as blood or protein in the urine. The damage is quietly under way long before anything shows on the surface — which is part of why finding and treating infection early matters so much.
Acute attacks
Many infected people suffer recurring acute episodes known as acute adenolymphangitis (ADL). These come on as bouts of fever and chills together with painful, swollen, tender lymph nodes and red, hot streaks tracking along an inflamed lymph vessel, most often in a leg, an arm, or the scrotum. Importantly, researchers have learned that many of these flares are triggered not by the worm itself but by ordinary bacterial and fungal skin infections that take hold in skin whose drainage is already compromised. This insight is genuinely useful, because it means simple skin care can prevent a large share of these miserable, disabling attacks.
Chronic lymphedema and elephantiasis
The manifestation everyone associates with this disease develops over years. As lymphatic vessels are repeatedly inflamed and scarred, they can no longer drain fluid, and it accumulates in the tissues — a swelling called lymphedema. Most often it affects the legs, but the arms, breasts, and genitals can also be involved. With time the trapped fluid, repeated infections, and hardening of the tissue thicken and roughen the skin into folds and warty nodules, producing the massive, firm, elephant-like limb that gives elephantiasis its name. Beyond the physical disability, the disfigurement carries a heavy toll of stigma, social exclusion, lost work and income, and mental-health suffering. It is one of the leading causes of long-term disability in the world.
Hydrocele and genital disease in men
Because W. bancrofti so often settles in the lymphatics of the groin, men frequently develop hydrocele — a collection of fluid around the testicle that swells the scrotum, sometimes to a very large and disabling size. In many endemic communities hydrocele is actually the most common chronic form of the disease among men. Some people also develop chyluria, in which milky, fat-laden lymph leaks into the urine. These genital and urinary problems, like leg lymphedema, can be deeply distressing and socially isolating.
5. Tropical Pulmonary Eosinophilia
A smaller number of people develop a strikingly different presentation called tropical pulmonary eosinophilia (TPE). Here the problem is not swollen limbs but the lungs. TPE is an intense allergic-type reaction in which the immune system attacks microfilariae as they pass through the lungs, clearing them so thoroughly that the tiny larvae usually cannot be found in the blood. The result is a set of asthma-like symptoms — cough, wheeze, and breathlessness that are typically worst at night — together with fatigue and sometimes weight loss.
The laboratory picture is distinctive: a very high eosinophil count (a type of white blood cell tied to allergy and parasites), markedly elevated antibody (IgE) levels, and strongly positive antifilarial antibody tests. TPE is more commonly recognized in parts of South Asia and tends to affect men. It is important to identify because it is frequently mistaken for ordinary asthma or tuberculosis, it responds well to the antiparasitic drug diethylcarbamazine, and if it is left untreated the ongoing inflammation can gradually scar the lungs.
6. Who Is Most at Risk
The people who bear this disease are, overwhelmingly, long-term residents of endemic tropical and subtropical regions. Lymphatic filariasis is still transmitted across parts of sub-Saharan Africa, South Asia (including India and Bangladesh, historically the heaviest burden), Southeast Asia, many Pacific island nations, and pockets of the Americas such as Haiti and parts of Brazil and Guyana. Within those regions, risk is tightly linked to poverty: crowded housing, standing water and poor drainage that breed mosquitoes, and limited access to protection or health care all raise exposure.
Because the disease builds up with cumulative mosquito bites, risk rises with the number of years a person lives in an endemic area, and lifelong residents carry the greatest burden. The forms the disease takes are shaped partly by sex: men are especially prone to hydrocele and other genital disease, while women disproportionately live with leg and breast lymphedema and the stigma that accompanies it. Children can be infected early and accumulate silent lymphatic damage long before symptoms appear. Short-term travelers, by contrast, are at very low risk.
7. Diagnosis
Diagnosing lymphatic filariasis has been transformed over the past few decades, and there are now several complementary ways to confirm it.
The classic method is to find the microfilariae themselves on a blood smear examined under the microscope. Because of the parasite's nocturnal rhythm, this requires the awkward step of drawing blood at night — typically between about 10 p.m. and 2 a.m. — when the larvae are circulating. The timing is inconvenient for patients and programs alike, which spurred the development of better tools.
The mainstay for W. bancrofti today is the circulating filarial antigen test, a simple point-of-care assay (the immunochromatographic card test, or ICT, and its successor the Filariasis Test Strip, or FTS). It detects a protein released by the adult worms and, crucially, can be done at any time of day, regardless of the microfilarial rhythm. A positive antigen test is strong evidence of active W. bancrofti infection and has become the backbone of mapping and diagnosis. Antibody tests add another layer, and are especially useful for surveillance and for detecting exposure in children as programs work toward elimination.
Imaging can be strikingly direct. High-frequency ultrasound of the scrotum or breast can reveal living adult worms writhing inside a dilated lymphatic vessel — a shimmering motion nicknamed the "filarial dance sign." Molecular (PCR) tests that detect worm DNA are also available. It is worth noting that in long-standing elephantiasis the worms may already be dead and microfilariae absent, and in TPE the immune reaction clears them from the blood — so a negative blood smear never rules out the disease on its own.
8. Treatment
Treatment of lymphatic filariasis has two distinct goals that both matter: killing or clearing the worms, and managing the damage they leave behind. A person can need one, the other, or both.
Drugs that target the worms
Diethylcarbamazine (DEC) has been the mainstay for decades; it rapidly clears microfilariae from the blood and kills some adult worms. It is frequently combined with albendazole. The right combination depends heavily on where a person lives, because two other filarial infections change the calculus: DEC can provoke severe reactions in people who also have onchocerciasis ("river blindness"), and the combination of ivermectin or DEC with heavy Loa loa (loiasis) infection can be dangerous. In much of sub-Saharan Africa, where these coexist, DEC is therefore avoided and ivermectin plus albendazole is used instead. Where onchocerciasis and loiasis are not a concern, a newer triple therapy of ivermectin, DEC, and albendazole (IDA) has been shown to clear microfilariae far more completely and durably than older regimens, and is now being scaled up. Separately, a course of the antibiotic doxycycline works in an ingenious way: it kills Wolbachia, bacteria that live inside the worms and that the worms depend on to survive and reproduce. Several weeks of doxycycline can sterilize and kill adult worms and, in trials, improve lymphedema — a useful option for treating individuals, though the long course makes it impractical for mass programs.
Managing the disease itself — the most hopeful part
Here lies a message of real hope. In people who already have lymphedema and elephantiasis, killing the worms does not reverse the swelling — but the swelling can still be controlled, and much of the suffering prevented, with simple, low-cost daily care. This approach, called morbidity management and disability prevention, centers on meticulous hygiene: washing the affected limb gently with soap and clean water every day, carefully treating the small skin wounds and fungal infections that let bacteria in, keeping nails and skin healthy, elevating the limb, moving and exercising it, and using compression or bandaging where appropriate. Done faithfully, this routine dramatically reduces the painful acute attacks and can halt or slow the progression to worse elephantiasis — even when the worms are long gone. For hydrocele, a relatively straightforward surgical repair (hydrocelectomy) can be life-changing. None of this requires expensive technology, which is exactly why it can reach the communities that need it.
9. Prevention and Global Elimination
In 2000 the World Health Organization launched the Global Programme to Eliminate Lymphatic Filariasis (GPELF), one of the largest public-health campaigns ever attempted. It rests on two pillars. The first is mass drug administration (MDA): giving safe, single-dose antiparasitic medicines once a year to entire at-risk communities — DEC plus albendazole, or ivermectin plus albendazole where onchocerciasis is present, or the newer IDA triple therapy where it can be used safely. The drugs do not necessarily kill every adult worm, but by keeping the level of microfilariae in the community very low, repeated year after year for at least five years, they starve the mosquitoes of parasites and break the chain of transmission. The second pillar is morbidity management and disability prevention — the hygiene-based limb care and hydrocele surgery described above — to relieve those already affected.
Mosquito control reinforces both pillars, and there is a valuable synergy with malaria programs: where Anopheles mosquitoes transmit both diseases, insecticide-treated bed nets fight filariasis and malaria at once. Because humans are the parasite's only meaningful reservoir, this combined strategy can actually finish the job. And it has been working: transmission has been interrupted across vast areas, hundreds of millions of treatments have been delivered, and roughly twenty countries and territories have already been validated by the WHO as having eliminated lymphatic filariasis as a public-health problem. For an individual living in or traveling to an endemic area, ordinary bite prevention — repellent, covering the skin, and sleeping under a net — remains sensible, but the story at the population level is one of steady, hard-won progress.
10. The Honest Bottom Line
Lymphatic filariasis is, at heart, a preventable and treatable cause of one of the world's most visible and stigmatizing disabilities. It is a disease of place and poverty, built up over years of mosquito bites — not something a short trip is likely to cause. The worms themselves are often silent, but the damage they do to the lymphatic system can, over time, devastate a person's body, livelihood, and standing in their community.
The genuinely hopeful truth is that we have the tools to end it. Inexpensive annual pills, given across whole communities, can stop transmission — and because the parasite has nowhere to hide outside of humans, that can drive it out of a country for good. For the millions already living with swelling, simple daily limb hygiene and, when needed, minor surgery can prevent much of the suffering, even after the worms are gone. Lymphatic filariasis remains a serious global problem, but it is also one of public health's real success stories in the making, with a growing list of nations that have already left it behind. If you live in or come from an endemic region, ask a clinician about a filarial antigen test; and if swelling has begun, know that gentle, consistent, hygiene-based care can make an enormous difference.
Key Research Papers
Peer-reviewed reviews and clinical trials on Wuchereria bancrofti and lymphatic filariasis — covering the parasite's biology and the pathology it causes, how the disease is diagnosed, the drugs used to treat it (including the doxycycline–Wolbachia approach and the newer triple-drug therapy), morbidity management, and the global elimination programme. Journal names appear as plain text; the year/volume/pages link opens the full citation via DOI.
- Taylor MJ, Hoerauf A, Bockarie M. Lymphatic filariasis and onchocerciasis. The Lancet. 2010;376(9747):1175–1185. — A comprehensive clinical seminar covering both filarial diseases, from biology to treatment and control.
- Ottesen EA. Lymphatic filariasis: treatment, control and elimination. Advances in Parasitology. 2006;61:395–441. — An authoritative overview of the drugs and strategy underpinning the global elimination programme.
- Dreyer G, Norões J, Figueredo-Silva J, Piessens WF. Pathogenesis of lymphatic disease in bancroftian filariasis: a clinical perspective. Parasitology Today. 2000;16(12):544–548. — Explains how living and dying adult worms, plus secondary bacterial infection, drive lymphedema.
- Weil GJ, Ramzy RM. Diagnostic tools for filariasis elimination programs. Trends in Parasitology. 2007;23(2):78–82. — Reviews the circulating filarial antigen tests that replaced awkward nighttime blood smears.
- Taylor MJ, Makunde WH, McGarry HF, Turner JD, Mand S, Hoerauf A. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. The Lancet. 2005;365(9477):2116–2121. — Landmark trial showing doxycycline, by killing Wolbachia, kills adult worms.
- Debrah AY, Mand S, Specht S, et al. Doxycycline reduces plasma VEGF-C/sVEGFR-3 and improves pathology in lymphatic filariasis. PLoS Pathogens. 2006;2(9):e92. — Found that doxycycline can actually improve established lymphedema, not just clear the parasite.
- Thomsen EK, Sanuku N, Baea M, et al. Efficacy, safety, and pharmacokinetics of coadministered diethylcarbamazine, albendazole, and ivermectin for treatment of bancroftian filariasis. Clinical Infectious Diseases. 2016;62(3):334–341. — Early evidence that the triple-drug (IDA) combination clears microfilariae more completely.
- King CL, Suamani J, Sanuku N, et al. A trial of a triple-drug treatment for lymphatic filariasis. New England Journal of Medicine. 2018;379(19):1801–1810. — Pivotal trial establishing ivermectin–DEC–albendazole as durable single-dose clearance.
- Molyneux DH, Bradley M, Hoerauf A, Kyelem D, Taylor MJ. Mass drug treatment for lymphatic filariasis and onchocerciasis. Trends in Parasitology. 2003;19(11):516–522. — Lays out the rationale and logistics of community-wide annual preventive chemotherapy.
- Ottesen EA, Hooper PJ, Bradley M, Biswas G. The Global Programme to Eliminate Lymphatic Filariasis: health impact after 8 years. PLoS Neglected Tropical Diseases. 2008;2(10):e317. — Quantifies the infections and disease prevented in the programme's first eight years.
- Ramaiah KD, Ottesen EA. Progress and impact of 13 years of the Global Programme to Eliminate Lymphatic Filariasis on reducing the burden of filarial disease. PLoS Neglected Tropical Diseases. 2014;8(11):e3319. — An updated accounting of cases and disability averted worldwide.
- Shenoy RK. Clinical and pathological aspects of filarial lymphedema and its management. The Korean Journal of Parasitology. 2008;46(3):119–125. — A practical review of hygiene-based limb care and morbidity management.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Wuchereria bancrofti lymphatic filariasis
- Filarial elephantiasis and lymphedema
- Wuchereria bancrofti hydrocele
- Filarial circulating antigen test
- DEC, albendazole, ivermectin therapy
- Doxycycline and Wolbachia
- Tropical pulmonary eosinophilia
- Global elimination and mass drug administration
Connections
- All Parasites
- Malaria
- Schistosoma
- Leishmania
- Giardia
- Toxoplasma
- Entamoeba
- Hookworm
- Ascaris
- Tapeworm
- Infectious Disease
- All Conditions