Multiple Sclerosis: History and Discovery
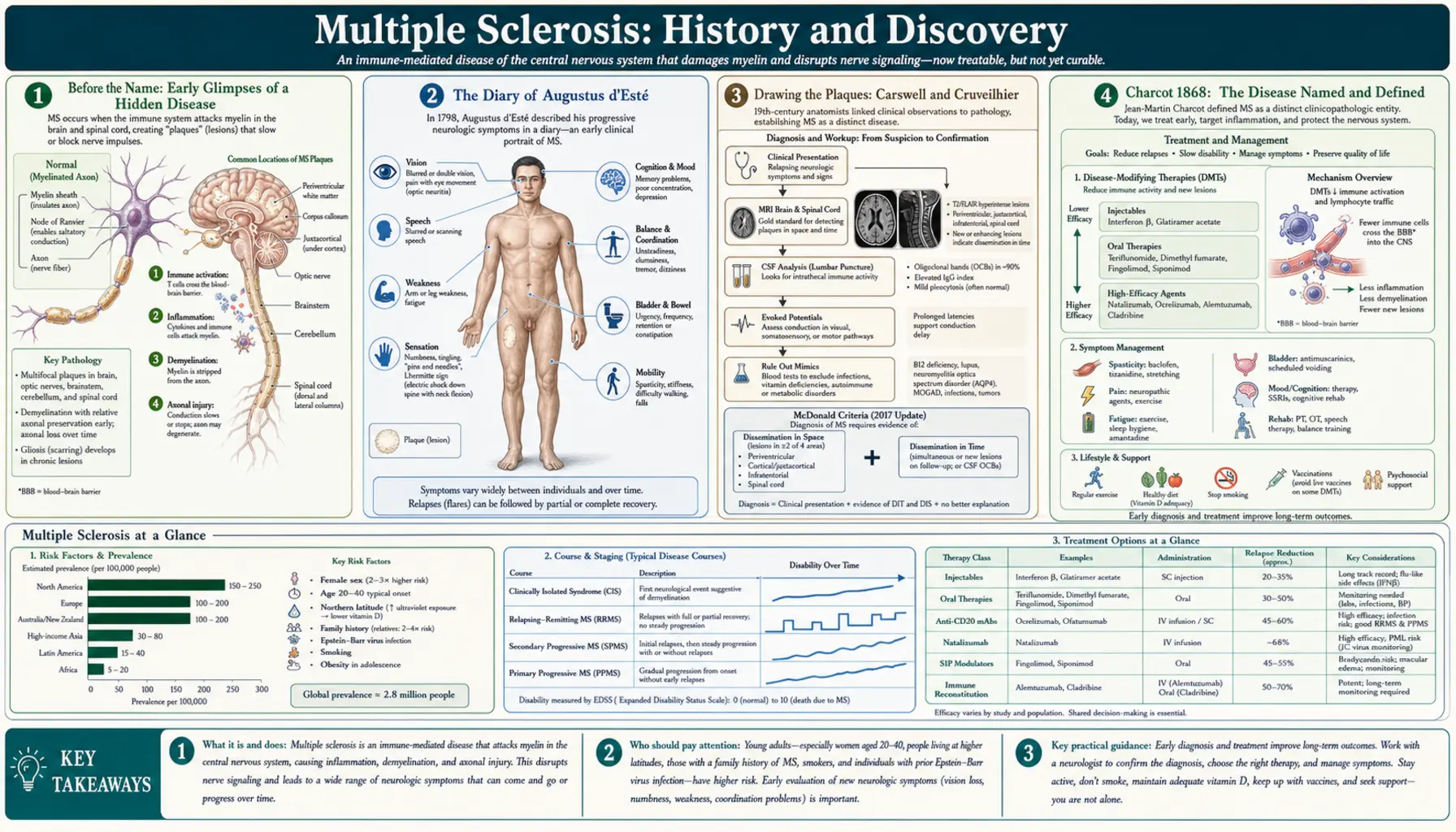
The story of multiple sclerosis is a study in how a disease becomes visible. For centuries its scattered, relapsing symptoms were mistaken for unrelated afflictions, witnessed only as a personal ordeal — most movingly in the diary that the Englishman Augustus d'Esté kept of his own decline in the 1820s. Pathologists drew the disease's scars before anyone knew what they meant: Robert Carswell illustrated them in 1838 and Jean Cruveilhier shortly after. It fell to the French neurologist Jean-Martin Charcot in 1868 to fuse the bedside and the autopsy table into a single, named disease — sclérose en plaques. The century and a half since has been a slow campaign to see further still: into the cerebrospinal fluid, onto the MRI scanner, and finally toward a cause. That cause remains incompletely understood, but it is no longer a mystery: a powerful 2022 study tied MS firmly to the Epstein–Barr virus, the strongest clue yet in a search that is still open.
Table of Contents
- Before the Name: Early Glimpses of a Hidden Disease
- The Diary of Augustus d'Esté
- Drawing the Plaques: Carswell and Cruveilhier
- Charcot 1868: The Disease Named and Defined
- After Charcot: Spreading the Knowledge
- Seeing Inside: Spinal Fluid, MRI, and Modern Diagnosis
- The Search for a Cause: Autoimmunity, Genes, and Environment
- The Epstein–Barr Breakthrough of 2022
- From No Treatment to Many: A Therapeutic Revolution
- Research Papers and References
- Connections
- Featured Videos
Before the Name: Early Glimpses of a Hidden Disease
Multiple sclerosis almost certainly affected people for centuries before it was recognized as a single disease. Its hallmark — symptoms that come and go, strike different parts of the body at different times, and partly recover — is exactly what makes a disease hard to name. A patient with transient blindness one year, numb legs the next, and unsteady hands the year after that does not obviously have one illness, and before the rise of clinical neurology there was no framework to connect such episodes. As a result, early possible cases survive only as scattered anecdotes that later historians have read back through modern eyes, with appropriate caution.
The case most often cited from the medieval period is that of Lidwina of Schiedam (1380–1433), a Dutch holy woman whose chroniclers described a decades-long illness beginning after a fall while ice-skating: difficulty walking, weakness, episodes of blindness, and waxing-and-waning paralysis that spared her until her death. Several authors have suggested this is a plausible early description of MS, though such a retrospective diagnosis from devotional hagiography can never be confirmed and should be treated as suggestive rather than certain. What these early fragments establish is not a firm diagnosis but a backdrop: the raw experience of MS existed long before the concept did.
The reason the disease stayed hidden is partly geographic and partly conceptual. MS is more common in temperate, higher-latitude regions, and its relapsing course meant that even attentive physicians saw only isolated episodes rather than a unifying pattern. The disease needed two things to become visible: detailed long-term observation of individual patients, and the post-mortem study of the brain and spinal cord. Both arrived in the nineteenth century, and the first to supply the former did so without any medical training at all — he simply wrote down, year after year, what was happening to his own body.
The Diary of Augustus d'Esté
The earliest record from which a confident diagnosis of multiple sclerosis can be made belongs not to a physician but to a patient: Sir Augustus Frederick d'Esté (1794–1848), a grandson of King George III. Beginning around 1822, d'Esté kept a private diary in which he meticulously recorded the course of a baffling illness that would shadow the rest of his life. His account is so clear and so clinically detailed that, when the diary was finally published in the twentieth century, neurologists could read in it the unmistakable signature of MS — making him, in the words of later historians, the first person for whom a definite diagnosis of multiple sclerosis can be established.
D'Esté's first symptom, around 1822, was a transient loss of vision — an episode consistent with optic neuritis, a common opening act of MS — which came on after he travelled to a funeral and strained to suppress his grief. Over the following years his diary records the disease unfolding in the classic relapsing-remitting manner: bouts of double vision, weakness and numbness in the legs, unsteadiness, bladder trouble, and problems that would partly recede only to return from a new direction. He documented the remedies of his era too — bleeding, plasters, steel-and-quinine tonics, mineral baths, electrical treatments, and a strikingly modern-sounding emphasis on horseback riding and exercise — leaving an unusually intimate portrait of living with a chronic neurological disease two centuries ago.
A point of honest historical nuance deserves mention: because his earliest symptoms were visual and his course was relapsing, some modern reviewers have asked whether d'Esté might instead have had neuromyelitis optica (NMO), a related but distinct demyelinating disease that was not separated from MS until much later. The mainstream reading remains that his diary describes MS, but the debate is itself instructive: it shows that even the founding case of the disease sits at the edges of categories that medicine is still refining. Either way, d'Esté's diary is rightly regarded as the first true case history of MS, written from the inside.
Drawing the Plaques: Carswell and Cruveilhier
While d'Esté was documenting the disease from within, anatomists in Paris and beyond were beginning to capture it from without — on the dissection table and in the engraver's plate. The disease's defining lesions are the hardened patches of scar tissue, or plaques, that form where the insulating myelin sheath of nerve fibers has been destroyed; the very name multiple sclerosis means "many scars." In the 1830s, two pathologists independently illustrated these plaques in the brain and spinal cord, years before anyone connected them to a recognized clinical syndrome.
The Scottish pathologist Robert Carswell (1793–1857) is generally credited with the first published illustration of the lesions. Working from specimens in Paris hospitals, he produced exquisite watercolor drawings of diseased tissue for his atlas Pathological Anatomy: Illustrations of the Elementary Forms of Disease, published in 1838, in which a plate depicts the brown, atrophied patches in the spinal cord that we now recognize as MS plaques. Carswell described what he saw faithfully but did not understand it as a distinct disease — he was cataloguing forms of pathology, not defining a clinical entity. His drawings are nonetheless the earliest known depiction of the lesions of MS.
His French contemporary Jean Cruveilhier (1791–1874), professor of pathological anatomy in Paris, illustrated and described very similar lesions in his own great atlas around the same period. Cruveilhier is sometimes named as the first illustrator, partly because the title page of the relevant volume bears an earlier date, but his atlas was issued in installments over many years, and careful bibliographic work indicates that the pages showing the MS-like lesions were actually published around 1841 — a few years after Carswell's 1838 plate. Crediting one over the other is therefore a genuine historical subtlety rather than a settled fact; what matters is that, by the early 1840s, the pathological appearance of the disease had been recorded in print by two independent observers. The image of the disease existed; its meaning did not yet.
Charcot 1868: The Disease Named and Defined
The decisive figure in the history of multiple sclerosis is Jean-Martin Charcot (1825–1893), the French physician often called the founder of modern neurology, who worked at the vast Salpêtrière hospital in Paris. Earlier observers had seen pieces of the puzzle — the patient's symptoms, the pathologist's plaques — but no one had assembled them into a single, coherent disease. In a celebrated series of lectures delivered in 1868, Charcot did exactly that: he correlated the clinical picture he observed in living patients with the scarred lesions found in their nervous systems after death, and in doing so defined multiple sclerosis as a distinct disease entity. He gave it the name by which it is still known in French, sclérose en plaques ("sclerosis in patches").
Charcot described the plaques in microscopic detail, noting the destruction of the myelin sheaths while the underlying nerve fibers (axons) were relatively spared in places, and the inflammation and scarring at the lesion sites. On the clinical side he identified a cluster of three signs that became famous as the Charcot triad: nystagmus (rhythmic involuntary eye movements), intention tremor (shaking that worsens as the hand reaches for a target), and scanning speech (a slow, broken-up, syllable-by-syllable manner of speaking, sometimes called telegraphic speech). He further divided the disease into cerebral, spinal, and mixed forms according to where the lesions predominated. It is worth being precise about the triad's status today: it is a genuine and historically important clinical observation, but it is now understood to be present in only a minority of patients and is no longer used to make the diagnosis — its value is descriptive and historical, not diagnostic.
Charcot's achievement was not the discovery of an unknown thing — the symptoms, the patients, and even the plaques had all been seen before. His achievement was conceptual: he turned a collection of separate observations into a defined, named, teachable disease, and in doing so he created the model for how clinical neurology would identify diseases thereafter. For this reason 1868 is rightly treated as the founding moment of MS as a medical concept, and Charcot as the man who, more than anyone, made the disease visible. The year 2018 was widely marked as the 150th anniversary of his account.
After Charcot: Spreading the Knowledge
Once Charcot had defined the disease, recognition of it spread quickly through the neurological world of the later nineteenth century. His lectures at the Salpêtrière drew students and visitors from across Europe and North America, and the new entity of sclérose en plaques — rendered in German as multiple Sklerose and in English first as "insular sclerosis," "disseminated sclerosis," and eventually "multiple sclerosis" — entered the textbooks. Charcot's own pupil Pierre Marie took an early interest in the possibility that infection might play a role in the disease, an idea that would prove remarkably prescient more than a century later, though the tools to test it did not yet exist.
The decades after Charcot were largely a period of careful clinical and pathological refinement rather than of dramatic breakthroughs. Physicians catalogued the disease's many presentations, mapped its tendency to relapse and remit, and debated its possible causes — toxins, infections, vascular problems, and inherited weakness were all proposed and argued over without resolution. A crucial conceptual advance came in the early twentieth century with the growing understanding that the plaques represented the loss of myelin, the fatty insulating sheath that lets nerve signals travel quickly; MS was increasingly understood as a demyelinating disease, even though why the myelin was being destroyed remained unknown.
For patients, however, this growing medical knowledge changed little. Through the first half of the twentieth century a diagnosis of MS still meant an illness that doctors could name and describe but could neither explain nor treat. The disease could only be diagnosed clinically — by observing the telltale pattern of neurological events separated in space and time — and confirmed only at autopsy. The great practical advances would have to wait for the second half of the century, when new technologies finally let physicians look inside the living nervous system.
Seeing Inside: Spinal Fluid, MRI, and Modern Diagnosis
For nearly a century after Charcot, diagnosing MS in a living person remained an exercise in clinical pattern-recognition: a neurologist looked for evidence of damage scattered across the nervous system (dissemination in space) and occurring at more than one time (dissemination in time), the two principles that still anchor the diagnosis today. The first laboratory aid came from the cerebrospinal fluid, the clear liquid bathing the brain and spinal cord. Researchers found that many people with MS have oligoclonal bands — distinctive bands of antibody that appear when the fluid is analyzed — signaling abnormal immune activity inside the central nervous system. This finding gave clinicians their first objective, if imperfect, biological marker of the disease.
The transformation came with magnetic resonance imaging (MRI), which from the early 1980s onward allowed the plaques Charcot had seen only at autopsy to be visualized, painlessly, in living patients. MRI could reveal lesions scattered through the white matter of the brain and spinal cord and, with repeat scanning, could show new lesions appearing over time — in effect, dissemination in space and time made visible. This was the single most important practical advance in MS since Charcot: it made earlier, more confident diagnosis possible and became the central tool for monitoring the disease and testing new treatments.
Diagnostic criteria evolved to keep pace. A committee chaired by George Schumacher published the first formal criteria in 1965, defining MS in purely clinical terms; the Poser criteria of 1983 added laboratory support including CSF findings. The landmark McDonald criteria, named after the neurologist W. Ian McDonald and first published in 2001 under the auspices of the U.S. National MS Society, formally incorporated MRI, allowing scan findings to stand in for clinical evidence of dissemination in space and time and thereby permitting diagnosis after a single attack in the right circumstances. Revised several times since (notably in 2010, 2017, and again in the 2020s), the McDonald criteria — with oligoclonal bands now able to substitute for dissemination in time — remain the international standard, enabling diagnosis far earlier than in Charcot's day.
The Search for a Cause: Autoimmunity, Genes, and Environment
The single most important honest statement in any history of MS is this: the ultimate cause is still not fully known. What has emerged over the past century, however, is a clear and broadly agreed framework. MS is understood as an autoimmune disease in which the body's own immune system — chiefly certain T cells and B cells — attacks the myelin sheath of nerves in the brain, spinal cord, and optic nerves, producing the inflammation, demyelination, and scarring that Charcot first described. Why the immune system turns on the body in this way is the question that the rest of MS research has spent decades trying to answer, and the consensus is that no single factor is to blame: MS arises from a combination of genetic susceptibility and environmental triggers.
On the genetic side, MS is not inherited in a simple way, but susceptibility clearly runs in families and is shaped by many genes. The strongest genetic signal lies in the HLA region (the human leukocyte antigen genes that govern immune recognition), where a particular variant known as HLA-DRB1*15:01 is the best-established genetic risk factor; large studies have since identified more than two hundred additional genetic variants that each nudge risk slightly. These genes do not cause MS by themselves — most people who carry them never develop the disease — but they set the immunological stage on which environmental factors act.
On the environmental side, several factors have been repeatedly linked to MS risk. The disease becomes markedly more common with distance from the equator, a latitude gradient long suspected to reflect differences in sunlight and therefore vitamin D: lower vitamin D levels are associated with higher MS risk, making vitamin D one of the most studied environmental factors, though whether supplementation prevents or alters the disease remains under active investigation and should be described as plausible rather than proven. Cigarette smoking, adolescent obesity, and low sun exposure are other consistently identified risk factors. And looming over all of them is a viral infection that turned out to matter more than any — the subject of the next section.
The Epstein–Barr Breakthrough of 2022
For decades, infection was suspected as a trigger for MS — Charcot's pupil Pierre Marie had floated the idea in the nineteenth century — and one virus drew particular suspicion: the Epstein–Barr virus (EBV), the extremely common herpesvirus that causes infectious mononucleosis ("mono") and infects the great majority of all adults worldwide. The trouble was proving cause rather than coincidence. Because almost everyone is eventually infected with EBV, simply noting that people with MS have been exposed to it proves little; demonstrating that the infection actually precedes and raises the risk of the disease required following enormous numbers of people over many years.
That evidence arrived in a landmark study published in the journal Science in January 2022 by Kjetil Bjornevik and colleagues at the Harvard T.H. Chan School of Public Health. The researchers used stored blood samples from more than ten million young adults on active duty in the U.S. military, collected over roughly two decades, which let them check each person's EBV status before MS appeared. The result was striking: the risk of developing MS rose about 32-fold after infection with EBV, while infection with other viruses (including the similarly transmitted cytomegalovirus) carried no such risk. Crucially, a blood marker of nerve damage called neurofilament light chain only began to rise after EBV infection, indicating that the viral infection came first and the neurological injury followed.
This study is widely regarded as the strongest evidence to date that EBV is a necessary — though clearly not sufficient — cause of multiple sclerosis. The careful word here is necessary: EBV infection appears to be required for MS to develop, but since billions of people carry EBV and only a small fraction ever develop MS, the virus must act together with genetic susceptibility and other factors to produce the disease. The mechanism is still being worked out, with leading hypotheses including molecular mimicry, in which immune cells trained against the virus cross-react with a similar-looking protein in myelin. It is fair to call the EBV finding the most important advance in understanding the cause of MS in a generation — while keeping firmly in view that the full causal chain is not yet complete, and that the cause of MS remains, in the strict sense, not fully resolved.
From No Treatment to Many: A Therapeutic Revolution
For most of its recognized history, MS could be named but not treated. From Charcot's era through the mid-twentieth century, physicians had nothing that altered the disease's course; care meant managing symptoms and supporting the patient. The first crack in this wall came with corticosteroids in the mid-twentieth century, which were found to shorten acute relapses (though not to change the long-term trajectory) and remain in use for flare-ups today. But the disease itself still could not be slowed.
The true revolution began in the 1990s with the first disease-modifying therapies. The interferon-beta drugs and glatiramer acetate, approved in that decade, were the first treatments shown to reduce the frequency of relapses and the accumulation of new MRI lesions — the first time in history that the underlying disease process could be partly held back. Their arrival was a watershed: MS shifted from an untreatable diagnosis to a manageable chronic condition, and MRI, by then in wide use, gave clinicians an objective way to measure whether the new drugs were working.
The years since have brought a steadily expanding arsenal of more powerful and more targeted therapies, including monoclonal antibodies that deplete or block the immune cells driving the disease — among them agents targeting the B cells that the EBV story has now thrown into sharp relief. Modern MS care can substantially reduce relapses and slow disability for many patients, and research has turned toward the harder problems of progressive MS and of repairing myelin rather than merely protecting it. The 2022 EBV discovery has even opened the prospect of prevention — through EBV vaccines or antiviral strategies — raising the once-unthinkable question of whether a disease first named in 1868 might one day be stopped before it starts. That remains a research goal rather than a present reality, but it is a measure of how far the understanding of MS has travelled from a patient's lonely diary and a pathologist's puzzling plates.
Research Papers and References
The references below combine key peer-reviewed and historical sources on the discovery and history of multiple sclerosis with curated PubMed topic-search links. Where a stable identifier is available it is given; the remaining entries open a PubMed search (National Library of Medicine) in a new tab. Historical primary works — Carswell's and Cruveilhier's atlases, Charcot's 1868 lectures, and d'Esté's diary — are named in the article as historical sources.
- Bjornevik K, Cortese M, Healy BC, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022;375(6578):296-301. — doi:10.1126/science.abj8222 (PMID: 35025605)
- Robinson WH, Steinman L. Epstein-Barr virus and multiple sclerosis. Science. 2022;375(6578):264-265 (perspective accompanying Bjornevik et al.). — doi:10.1126/science.abm7930
- Kumar DR, Aslinia F, Yale SH, Mazza JJ. Jean-Martin Charcot: the father of neurology. Clinical Medicine & Research. 2011;9(1):46-49. — doi:10.3121/cmr.2009.883
- Murray TJ. The history of multiple sclerosis: the changing frame of the disease over the centuries. Journal of the Neurological Sciences. 2009;277 Suppl 1:S3-S8. — PubMed: Murray, history of multiple sclerosis
- Pearce JMS. Historical descriptions of multiple sclerosis. European Neurology. 2005;54(1):49-53. — doi:10.1159/000087387
- Compston A. The 150th anniversary of the first depiction of the lesions of multiple sclerosis. Journal of Neurology, Neurosurgery & Psychiatry. 1988;51(10):1249-1252. — doi:10.1136/jnnp.51.10.1249
- Landtblom AM, Fazio P, Fredrikson S, Granieri E. The first case history of multiple sclerosis: Augustus d'Esté (1794-1848). Neurological Sciences. 2010;31(1):29-33. — doi:10.1007/s10072-009-0161-4
- Lassmann H. The 150th anniversary of Charcot's report and the history of multiple sclerosis pathology — PubMed: Charcot, 150 years, sclérose en plaques
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. The Lancet Neurology. 2018;17(2):162-173. — doi:10.1016/S1474-4422(17)30470-2
- McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis (the original 2001 McDonald criteria). Annals of Neurology. 2001;50(1):121-127. — doi:10.1002/ana.1032
- International Multiple Sclerosis Genetics Consortium. HLA-DRB1*15:01 and the genetics of multiple sclerosis susceptibility — PubMed: MS HLA-DRB1*15:01 genetic susceptibility
- Vitamin D, latitude, and multiple sclerosis risk — PubMed: vitamin D, latitude, and MS risk
- Robert Carswell and the first illustration of the lesions of multiple sclerosis — PubMed: Carswell, first illustration of MS
- History of disease-modifying therapy and interferon-beta in multiple sclerosis — PubMed: MS disease-modifying therapy history
External Authoritative Resources
- NINDS (NIH) — Multiple Sclerosis Information
- National Multiple Sclerosis Society
- PubMed — All research on the history and discovery of multiple sclerosis
Connections
- Neurology
- Multiple Sclerosis (MS)
- All Conditions
- ALS (Amyotrophic Lateral Sclerosis)
- Parkinson's Disease
- Myasthenia Gravis
- Lupus
- Vitamin D3