Cerebral Venous Thrombosis
Cerebral venous sinus thrombosis (CVST) is thrombosis of the dural venous sinuses and/or cortical cerebral veins, obstructing venous drainage of the brain. Unlike arterial stroke — which follows well-defined vascular territories — CVST produces venous hypertension, cytotoxic and vasogenic edema, and hemorrhagic venous infarction in a distribution that does not respect arterial boundaries. It disproportionately affects young adults and women of childbearing age; oral contraceptive use is the single most common identifiable risk factor in developed countries. Because headache is the predominant and often isolated presenting symptom and brain CT is frequently normal, CVST is among the most commonly missed neurological diagnoses. Prompt recognition and anticoagulation are critical — most patients recover fully with treatment, but delayed diagnosis leads to irreversible brain injury and death.
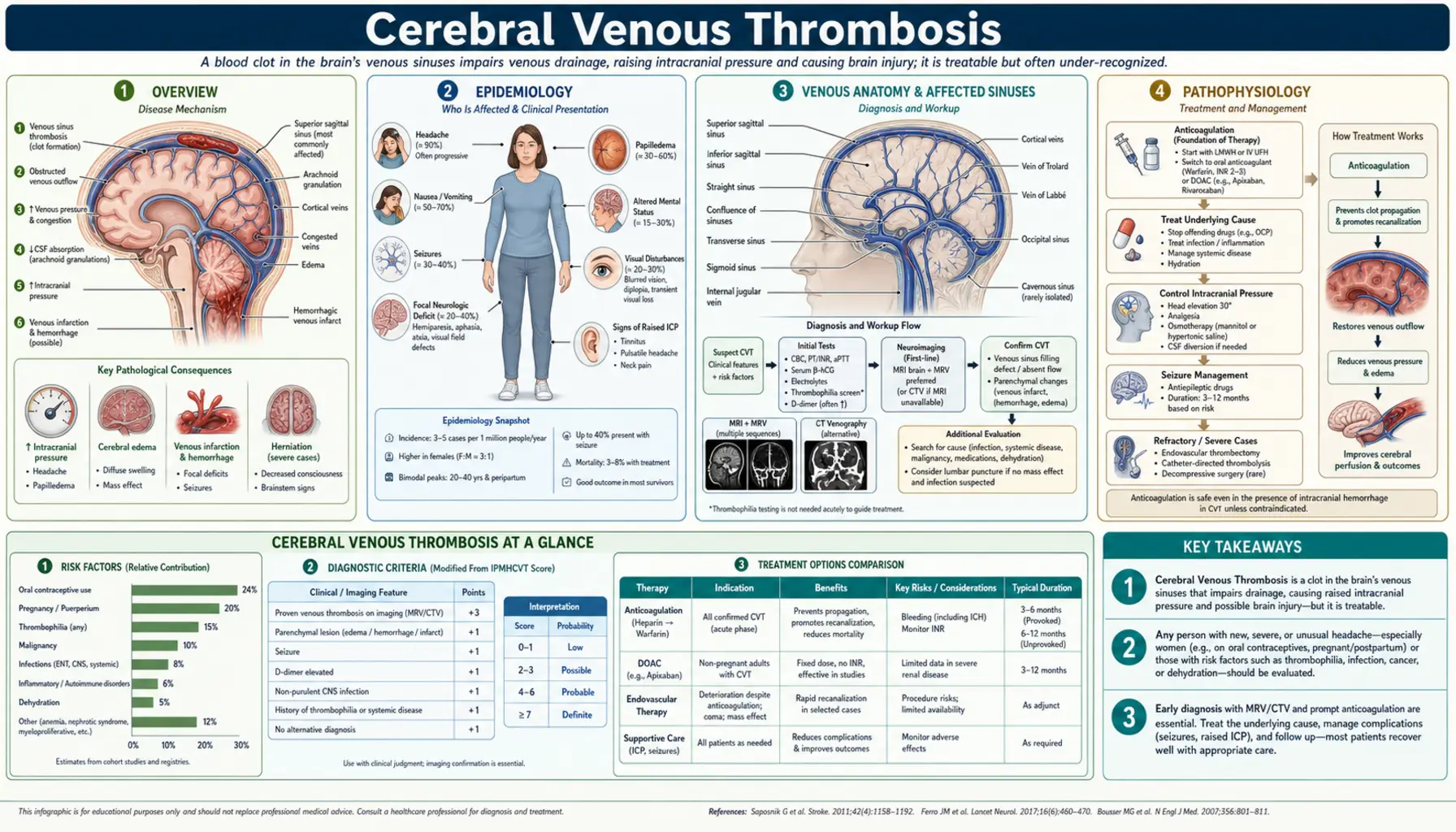
Table of Contents
- Overview
- Epidemiology
- Venous Anatomy and Affected Sinuses
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Prognosis and Outcomes
- Special Populations
- Key Research and Recent Advances
- References
- Featured Videos
1. Overview
CVST encompasses thrombosis affecting the large dural venous sinuses (superior sagittal sinus, lateral/transverse sinuses, straight sinus, cavernous sinus) as well as the smaller cortical veins draining into them. The superior sagittal sinus is involved in more than 50% of cases, followed by the lateral sinuses (44%), straight sinus (18%), and cortical veins (17%); multiple sinus involvement occurs in approximately 30% of cases. The condition must be distinguished from idiopathic intracranial hypertension (IIH/pseudotumor cerebri), arterial stroke, encephalitis, and brain tumor — all of which can present with headache, papilledema, or focal deficits.
A landmark shift in CVST understanding occurred in 2021 with the recognition of vaccine-induced immune thrombocytopenia and thrombosis (VITT), a rare but severe CVST syndrome triggered by adenoviral vector COVID-19 vaccines (AstraZeneca/ChAdOx1; J&J/Ad26.COV2.S). VITT-associated CVST is characterized by anti-PF4 antibodies (identical to heparin-induced thrombocytopenia, HIT type 2) and is treated differently — heparin is contraindicated, and IVIG is first-line. This discovery has reinforced the importance of checking platelet count in every CVST patient before starting anticoagulation.
2. Epidemiology
The annual incidence of CVST is approximately 1.32–1.57 cases per 100,000 population, making it far less common than arterial stroke but with similar or greater diagnostic challenge due to variable presentation. Women are disproportionately affected, with a female-to-male ratio of approximately 3:1 overall, driven by oral contraceptive use and pregnancy/puerperium risk. The peak incidence is in young adults aged 20–35 years, though CVST occurs at all ages including neonates and children (where infection and dehydration are the leading causes) and the elderly (where malignancy and hyperviscosity predominate).
CVST accounts for approximately 0.5–1% of all strokes but up to 15% of strokes in women under 45 years of age. Despite its rarity, CVST is important because it disproportionately affects young productive adults and, with prompt treatment, carries substantially better outcomes than arterial stroke (case fatality 8–10% in modern series, compared to 25–30% for large-vessel arterial stroke). In-hospital mortality in contemporary cohorts is 3–4% with appropriate anticoagulation.
3. Venous Anatomy and Affected Sinuses
The dural venous sinuses are endothelium-lined venous channels within the dura mater, lacking valves (allowing bidirectional flow) and receiving drainage from cortical veins, diploic veins (skull), and emissary veins (scalp). Key sinuses and their clinical correlates:
- Superior sagittal sinus (SSS): Runs in the superior dural fold from the crista galli to the torcular Herophili (confluence of sinuses); drains most of the cerebral convexity via cortical veins. SSS thrombosis → bilateral cortical venous infarction (often parasagittal), bilateral leg weakness (characteristic "man in a barrel" pattern), seizures, raised intracranial pressure, and in severe cases herniation. Most commonly affected sinus (>50% of cases).
- Lateral (transverse + sigmoid) sinuses: Each transverse sinus runs laterally from the torcular; the sigmoid sinus is its S-shaped continuation leading to the jugular bulb. Thrombosis causes headache, papilledema, and isolated intracranial hypertension mimicking IIH — particularly common with lateral sinus thrombosis. Left lateral sinus thrombosis may cause aphasia via involvement of draining Labbé vein territory.
- Straight sinus: Receives the great cerebral vein of Galen; drains deep structures (basal ganglia, thalami). Straight sinus thrombosis → deep venous infarction with bilateral thalamic edema — associated with altered consciousness, coma, and poor prognosis. The least common but most dangerous single-sinus involvement.
- Cavernous sinus: Paired sinus flanking the sella turcica, receiving drainage from the orbit and superior ophthalmic vein. Cavernous sinus thrombosis (CST) is usually septic (from facial infection, sinusitis, dental abscess) and presents with orbital pain, chemosis, proptosis, ophthalmoplegia (CN III/IV/VI palsies), and periorbital edema — often bilateral due to sinus intercommunication.
- Cortical vein thrombosis: Isolated cortical vein thrombosis without sinus involvement is underdiagnosed; presents with focal seizures or focal deficits corresponding to the draining territory; visible on MRI FLAIR/T1 (cord sign = hyperdense vein) + susceptibility-weighted imaging (SWI).
4. Pathophysiology
CVST causes brain injury through two simultaneous mechanisms that often coexist in the same patient, accounting for the heterogeneous MRI appearance:
Venous Hypertension and Edema
Thrombotic obstruction of a venous sinus raises venous pressure in draining cortical veins. When venous pressure exceeds capillary perfusion pressure, cerebral blood flow in the drained territory falls — a mechanism fundamentally different from arterial occlusion. The resulting edema is initially vasogenic (blood-brain barrier disruption from venous hypertension) and, as ischemia deepens, becomes cytotoxic. Critically, venous collateral drainage (leptomeningeal veins, diploic channels) often develops rapidly, limiting infarction — this explains why large SSS thromboses can present with only headache and papilledema with no parenchymal injury, while smaller thrombi in poor-collateral territories cause massive hemorrhagic infarction.
Hemorrhagic Venous Infarction
When venous hypertension exceeds the capacity of collateral drainage, venules rupture into the parenchyma, producing hemorrhagic venous infarction. These lesions do not follow arterial territories, are often bilateral and parasagittal (for SSS thrombosis), and typically show surrounding edema exceeding the hemorrhage volume. The hemorrhagic nature of CVST lesions historically led to inappropriate withholding of anticoagulation — a practice now recognized as harmful, since the heparin trials demonstrated that anticoagulation reduces mortality and improves outcomes despite hemorrhage.
Raised Intracranial Pressure
Impaired CSF absorption at arachnoid granulations (which drain into the SSS) — combined with reduced venous capacitance — raises intracranial pressure (ICP). This mechanism is responsible for the IIH-like syndrome of isolated intracranial hypertension seen in lateral sinus thrombosis, with headache and papilledema but no focal deficits or parenchymal injury.
5. Etiology and Risk Factors
Hormonal and Pregnancy-Related (Young Women)
- Combined oral contraceptives (OCP): Estrogen-containing OCPs increase coagulation factor levels (II, VII, VIII, X, fibrinogen) and reduce protein S; relative risk of CVST is approximately 13-fold; risk further amplified by concomitant thrombophilia (factor V Leiden + OCP = 30-fold risk). The most common identifiable cause of CVST in developed countries.
- Pregnancy and puerperium: Third trimester and the first 4 weeks post-partum are the highest-risk period; puerperal CVST (formerly the most common cause historically) still accounts for 5–20% of cases in developing countries with high rates of pregnancy-related infection and dehydration. Pathophysiology: physiological hypercoagulability of pregnancy + venous stasis + local injury from delivery.
- Hormone replacement therapy (HRT): Similar mechanism to OCP though lower estrogen doses than first-generation pills; smaller increase in relative risk.
Thrombophilia
- Factor V Leiden (G1691A): Most common inherited thrombophilia in Europeans (~5% carrier frequency); responsible for activated protein C resistance; increases CVST risk 3–4-fold alone, multiplicatively with OCP.
- Prothrombin G20210A mutation: Second most common inherited thrombophilia (~2% frequency); increases prothrombin (factor II) levels; OR for CVST approximately 2.5–5.
- Antithrombin, protein C, or protein S deficiency: Rarer but high-risk hereditary thrombophilias; evaluate in young patients with unprovoked CVST and family history of thrombosis.
- Antiphospholipid syndrome (APS): Acquired thrombophilia; anticardiolipin antibodies, anti-β2-glycoprotein-I, and lupus anticoagulant increase arterial and venous thrombosis risk; mandates long-term anticoagulation.
- Hyperhomocysteinemia: Elevated homocysteine impairs endothelial function; associated with MTHFR mutations and B vitamin deficiencies (B6/B9/B12); moderate risk factor for CVST.
Infection
- Otogenic lateral sinus thrombosis: Otitis media/mastoiditis spreads to sigmoid/transverse sinus via emissary veins; formerly called "otitic hydrocephalus"; treated with antibiotics ± anticoagulation ± mastoidectomy.
- Sinusitis-related SSS/cavernous sinus thrombosis: Frontal sinusitis → SSS thrombosis (Pott's puffy tumor); ethmoid/sphenoid sinusitis → cavernous sinus thrombosis; common pathogens: Staphylococcus aureus, Streptococcus spp., gram-negative organisms.
- Meningitis: Bacterial meningitis (especially in neonates and children) can cause CVST as a complication of infectious vasculitis and local thrombogenic inflammation.
- COVID-19: SARS-CoV-2 infection associated with increased CVST risk via endothelial injury, hypercoagulability, and platelet activation.
Malignancy and Hematological Disorders
- Solid tumor compression or direct invasion of venous sinuses (meningioma, metastasis)
- Paraneoplastic hypercoagulability; L-asparaginase chemotherapy depletes antithrombin
- Polycythemia vera, essential thrombocythemia — myeloproliferative neoplasms; JAK2 V617F mutation testing is important in young patients with unprovoked CVST
- Paroxysmal nocturnal hemoglobinuria (PNH) — rare but important cause in young adults with unexplained venous thrombosis in unusual sites
Other Causes
- Head trauma (direct venous laceration or delayed thrombosis)
- Intracranial hypotension (CSF leak — after lumbar puncture, spontaneous, post-neurosurgery); downward brain shift stretches bridging veins and sinuses promoting thrombosis
- Dehydration (common in neonates and elderly)
- Inflammatory bowel disease (Crohn's, ulcerative colitis) — especially during flares
- Systemic lupus erythematosus, Behçet's disease (vasculitis)
- Nephrotic syndrome (loss of antithrombin and protein C/S in urine)
- VITT (post-adenoviral vector COVID-19 vaccine): anti-PF4 antibody-mediated platelet activation — distinct mechanism requiring non-heparin anticoagulation
6. Clinical Presentation
Headache — The Cardinal Symptom
Headache is the presenting symptom in approximately 90% of CVST patients and is the sole symptom in 25% of isolated intracranial hypertension presentations. Unlike the thunderclap headache of subarachnoid hemorrhage, CVST headache typically has a subacute onset over days to weeks, is diffuse, progressive, and worsening — often positional (worse lying flat due to elevated ICP) or worsening with Valsalva. However, thunderclap CVST onset does occur (15% of cases) and must be included in the differential diagnosis of sudden severe headache alongside SAH. The headache may be accompanied by nausea, vomiting, and photophobia, mimicking migraine or tension headache — leading to delayed diagnosis of 1–4 weeks on average.
Focal Neurological Deficits
- Hemiparesis or monoparesis — particularly leg-predominant (parasagittal cortex drained by SSS) or bilateral leg weakness (bilateral parasagittal infarction from SSS thrombosis)
- Aphasia — left hemisphere cortical vein or left lateral sinus thrombosis
- Hemianopia or cortical visual loss
- Sensory deficits in a cortical distribution
- Bilateral thalamic syndrome — altered level of consciousness, memory impairment, movement disorder — from deep venous thrombosis (straight sinus/Galen vein)
Seizures
Seizures occur in approximately 40% of CVST patients — a substantially higher rate than arterial stroke (8–10%), reflecting cortical irritation from hemorrhagic venous infarction and perilesional edema. Focal-onset seizures with secondary generalization are most common; status epilepticus occurs in 5–10% and carries significantly worse prognosis. Early seizures (within 2 weeks) predict higher risk of further seizures but do not independently worsen long-term outcome when controlled. Prophylactic antiepileptics are recommended in patients with cortical lesions or early seizures for at least 1 year.
Isolated Intracranial Hypertension Syndrome
Approximately 20–40% of CVST — predominantly lateral sinus thrombosis — presents as isolated intracranial hypertension without focal deficits or parenchymal injury, clinically indistinguishable from idiopathic intracranial hypertension (IIH/pseudotumor cerebri). These patients have headache, papilledema, and visual obscurations; CSF opening pressure is elevated; brain MRI parenchyma is normal. CVST must be excluded by MRV in every patient diagnosed with IIH for the first time — particularly in men, older women, and patients without the typical obese young woman demographic.
Cavernous Sinus Thrombosis
Septic cavernous sinus thrombosis presents with periorbital edema, proptosis, chemosis, ophthalmoplegia (CN III/IV/VI), and retinal venous congestion, often progressing from unilateral to bilateral within 24–48 hours via the intercavernous sinus. Fever, leukocytosis, and identifiable primary infection source (facial cellulite, sinusitis, dental abscess) differentiate septic CST from aseptic orbital apex syndrome. Urgent antibiotics (with antifungal cover if mucormycosis is suspected in immunocompromised or diabetic patients) are primary therapy.
Encephalopathy and Coma
Progressive encephalopathy, bilateral thalamic dysfunction, coma, or decerebrate posturing indicate deep venous involvement (straight sinus ± Galen vein thrombosis) — the most severe presentation with the worst prognosis. Bilateral thalamic hyperintensity on MRI in a young patient without arterial risk factors should immediately raise suspicion for deep CVST.
7. Diagnosis
Brain CT — Initial Emergency Scan
Non-contrast CT is typically the first imaging obtained. It may show:
- Dense (hyperdense) cord sign: Hyperdense thrombus in a cortical vein on non-contrast CT, visible as a tubular cord-like density — specific but only present in 25–30% of cases.
- Dense triangle sign: Triangular hyperdensity in the posterior superior sagittal sinus — fresh thrombus; present in 10–20% of cases.
- Empty delta sign (contrast CT): Triangular filling defect in the posterior SSS on contrast-enhanced CT, representing thrombus surrounded by collateral flow — present in 35–40% of cases with SSS thrombosis; classic but not pathognomonic (absent in acute phase, before collateral opacification).
- Hemorrhagic venous infarction: bilateral parasagittal hemorrhages not conforming to arterial territories
- Diffuse cerebral edema, sulcal effacement
- Normal CT (in up to 30–40% of cases) — a normal CT does not exclude CVST
MRI Brain + MRV — Gold Standard
MRI with MR venography (MRV) is the gold standard investigation, with sensitivity approaching 90–95% for CVST when T1, T2, FLAIR, DWI, susceptibility-weighted imaging (SWI), and time-of-flight (TOF) MRV sequences are combined:
- T1-weighted: Isointense (acute, days 1–5) → hyperintense (subacute, days 5–14) thrombus signal within the sinus; hyperintense on T1 is highly specific when combined with MRV absence of flow
- T2/FLAIR: Hyperintense thrombus (subacute); venous edema/infarction in drained territory; cortical/subcortical signal change not following arterial boundaries
- SWI/GRE (susceptibility-weighted imaging): Blooming artifact (hypointense) from hemoglobin breakdown products in thrombus and microhemorrhages; excellent for detecting cortical vein thrombosis and early hemorrhagic change
- DWI: Restricted diffusion in cytotoxic edema component of venous infarction; ADC map helps distinguish reversible (high ADC) from irreversible (low ADC) injury
- TOF MRV/phase-contrast MRV: Demonstrates absent or markedly reduced flow in thrombosed sinuses; TOF has false positives from flow-related saturation in slow flow; gadolinium-enhanced MRV improves specificity
- CT venography (CTV): Excellent alternative to MRV, particularly in acute setting or when MRI is contraindicated; fast acquisition; filling defects in sinuses on CTV match MRV sensitivity for major sinuses; requires iodinated contrast and radiation
Laboratory Investigations
- D-dimer: Elevated in most CVST patients but non-specific; a normal D-dimer makes CVST unlikely (negative predictive value ~99% in low-pretest-probability patients) — useful to guide imaging decision in low-probability headache workup. However, D-dimer may be normal in isolated headache/papilledema CVST presentations.
- CBC with platelet count: Critical before anticoagulation — thrombocytopenia suggests VITT or HIT; polycythemia or thrombocytosis suggest myeloproliferative neoplasm
- Anti-PF4 antibody (ELISA or CLIA): Test in all patients with recent adenoviral vector COVID-19 vaccine (within 4–28 days) + thrombocytopenia
- Coagulation screen: PT, aPTT, fibrinogen; lupus anticoagulant (aPTT-based assay)
- Thrombophilia workup: Antithrombin activity, protein C activity, protein S free antigen (defer protein S/C/antithrombin testing until off anticoagulation; levels unreliable during acute thrombosis); factor V Leiden PCR; prothrombin G20210A PCR; anticardiolipin IgG/IgM; anti-β2-GP1 IgG/IgM; JAK2 V617F mutation (if clinical suspicion for myeloproliferative neoplasm)
- Homocysteine: Elevated in vitamin B12/B9/B6 deficiency, MTHFR mutations
- Blood cultures + inflammatory markers (CRP, ESR): If septic CVST or cavernous sinus thrombosis suspected
- PNH screen (flow cytometry): In young patients with unexplained CVST + cytopenias or hemolysis
Lumbar Puncture
LP can be performed safely after imaging confirms no mass lesion or significant midline shift. CSF findings in CVST: elevated opening pressure (often >25 cmH2O), mildly elevated protein (50–100 mg/dL), mild pleocytosis (<50 cells/mm³), or xanthochromia (if subarachnoid blood). LP is also therapeutic for severe papilledema with visual deterioration (reduces ICP acutely). CSF analysis also helps exclude meningitis/encephalitis, which may coexist with or mimic CVST.
8. Treatment
Anticoagulation — First-Line Therapy
Anticoagulation is the cornerstone of CVST treatment, despite the frequent presence of hemorrhagic venous infarction. Two small but influential randomized controlled trials (Einhäupl 1991; de Bruijn 1999) and multiple meta-analyses demonstrate that heparin anticoagulation reduces mortality and severe disability without significant increase in hemorrhagic complications. The pathophysiological rationale is compelling: anticoagulation arrests thrombosis propagation and allows natural thrombolysis to restore venous drainage, reducing venous hypertension and preventing further infarction. The hemorrhagic component of venous infarction does not worsen significantly with anticoagulation — it is a consequence of venous hypertension, not the anticoagulant.
- Acute phase: Low molecular weight heparin (LMWH, e.g., enoxaparin 1 mg/kg twice daily) or unfractionated heparin (UFH) IV — UFH preferred when rapid reversal may be needed (severe hemorrhage, need for urgent surgery). LMWH is generally preferred for its predictable pharmacokinetics and lower HIT risk.
- VITT exception: Standard heparin (UFH or LMWH) is contraindicated in VITT-associated CVST (anti-PF4 antibody positive + thrombocytopenia). Use non-heparin anticoagulation: argatroban, fondaparinux, or direct oral anticoagulants (apixaban/rivaroxaban). IVIG 1 g/kg/day × 2 days is first-line to neutralize anti-PF4 antibodies and halt platelet activation. Platelet transfusion contraindicated (worsens thrombosis by providing fuel for anti-PF4-driven platelet activation).
- Transition and duration: After acute LMWH/UFH, transition to oral anticoagulation:
- Warfarin (target INR 2.0–3.0) for 3–6 months for provoked (reversible risk factor) CVST; 6–12 months for unprovoked; indefinite if thrombophilia (APS, antithrombin deficiency) or recurrent thrombosis
- Dabigatran (RE-SPECT CVST trial) is non-inferior to warfarin with better tolerability; now a guideline-endorsed alternative
- Rivaroxaban and apixaban used in practice (extrapolated from VTE trials) though RCT data for CVST are limited beyond dabigatran
Endovascular Thrombectomy and Local Thrombolysis
Endovascular treatment — mechanical thrombectomy (aspiration, stent-retriever) ± local catheter-directed thrombolysis (urokinase, tPA) via the venous sinuses — is reserved for patients with severe CVST deteriorating despite therapeutic anticoagulation. The ISCVT registry identifies factors predicting poor outcome with anticoagulation alone: coma (GCS <9), deep venous thrombosis, ICH at presentation, and bilateral motor deficits. Endovascular treatment has not been evaluated in an RCT against anticoagulation, but case series report recanalization in 70–80% of treated patients; the TODAM registry provides the largest contemporary data. Endovascular treatment is reserved for ≤10% of CVST cases.
Antiepileptic Drugs (AEDs)
Prophylactic AEDs are recommended for patients with cortical lesions or supratentorial hemorrhagic infarction even without clinical seizures, given high spontaneous seizure risk (40%). Levetiracetam is preferred (minimal drug interactions, no hepatic induction). Valproate and phenytoin are alternatives. Duration: generally continue for 1 year in patients with cortical lesions; earlier discontinuation is reasonable in those without seizures and with lesion resolution. Routine prophylaxis in patients without cortical lesions is not strongly supported by evidence.
Intracranial Pressure Management
- Head elevation (30°), avoid hypercapnia
- Acetazolamide (250–500 mg twice daily) reduces CSF production; useful for isolated intracranial hypertension phenotype
- Repeated therapeutic LPs for severe papilledema with visual deterioration
- Osmotic therapy (mannitol, hypertonic saline) for acute ICP crises
- Decompressive craniectomy: lifesaving in malignant cerebral edema (large hemorrhagic venous infarction + uncal herniation); may be required as a bridge to anticoagulation-mediated recanalization
- CSF diversion (ventriculostomy, ventriculoperitoneal shunt) for obstructive hydrocephalus
Infection Treatment (Septic CVST)
Intravenous antibiotics covering the causative pathogen are mandatory and should be started immediately upon suspicion of septic CVST, before culture results return. Empiric coverage: vancomycin + ceftriaxone ± metronidazole (for anaerobes from dental/sinus source). Duration typically 4–6 weeks IV followed by oral completion. Surgical source control (mastoidectomy, sinus drainage, dental extraction) is required for ongoing infectious foci — failure to control the source leads to refractory septic thrombosis. Anticoagulation in septic CVST remains controversial but is used at most centers for deteriorating patients without contraindication.
9. Prognosis and Outcomes
Modern CVST prognosis is substantially better than historical series, reflecting improved recognition and universal anticoagulation. The International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT, n=624) established the best available natural history data:
- Complete recovery: approximately 57% of patients at 16 months
- Disability (modified Rankin Scale ≥2): approximately 22%
- In-hospital mortality: 3.4–8%; total mortality at 16 months: 8.3%
- Recurrent venous thrombosis (any site): 2.2% per year; recurrent CVST: 1.5% in first year
- Seizure recurrence risk at 1 year: 10% in patients on AEDs; driving restriction typically 1 year seizure-free
Predictors of Poor Outcome (ISCVT Data)
- Deep venous thrombosis (straight sinus/Galen vein involvement) — strongest predictor of death/disability (OR 4.0)
- Coma (GCS <9) at presentation — independent predictor of mortality
- Intracranial hemorrhage at presentation
- Malignancy as underlying cause
- Age >37 years (in some series)
- VITT-associated CVST — high mortality if not recognized and treated promptly (mortality 22% in early case series, improving with IVIG protocols)
Recanalization
Partial or complete sinus recanalization occurs in approximately 80% of patients with anticoagulation, most within 3–6 months of treatment. Recanalization correlates with better functional outcomes but is not universal; partial or absent recanalization does not preclude good functional recovery if collateral drainage is adequate. MRV at 3–6 months after treatment is recommended to assess recanalization and guide anticoagulation duration decisions.
10. Special Populations
Pregnancy and Puerperium
LMWH is safe in pregnancy (does not cross the placenta) and is the anticoagulant of choice throughout pregnancy. Switch to UFH at 36 weeks to allow neuraxial anesthesia planning. Post-partum: restart LMWH within 12–24 hours of delivery; transition to warfarin or DOAC (not dabigatran — excreted in breast milk) after 6–12 weeks. Future pregnancies should be managed with LMWH prophylaxis, particularly during the puerperium. Oral contraception is permanently contraindicated after CVST from OCP.
Pediatric CVST
Neonatal CVST: most commonly presents with seizures in the first week of life; SSS and straight sinus predominantly affected; dehydration, perinatal asphyxia, infection are common causes; treatment with LMWH is reasonable but evidence base is weaker than adults; outcome generally good with appropriate treatment. Childhood/adolescent CVST: head/neck infection (otitis media, mastoiditis), leukemia, L-asparaginase chemotherapy, and iron-deficiency anemia are important causes not seen in adults.
Elderly CVST
Malignancy, myeloproliferative neoplasms, dehydration from intercurrent illness, and DOAC interruption or under-dosing are the primary etiologies. Presentation may be atypical (encephalopathy, confusion) without prominent headache. Higher hemorrhagic risk with anticoagulation in elderly; balance individualized.
11. Key Research and Recent Advances
The RE-SPECT CVST trial (2019, n=120) is the pivotal study demonstrating that dabigatran (150 mg twice daily) is non-inferior to warfarin for preventing recurrent venous thromboembolism after CVST, with comparable rates of major bleeding. This trial provided the first high-quality RCT evidence for a DOAC in CVST and has shifted clinical practice toward dabigatran as a warfarin alternative, with rivaroxaban and apixaban used based on class-effect extrapolation from VTE trials.
The identification of VITT as a CVST-specific syndrome in 2021 (Greinacher et al., NEJM; Schultz et al., NEJM) transformed understanding of immune-mediated thrombosis. VITT mimics HIT type 2 mechanistically (anti-PF4 IgG antibodies triggering FcγRIIA-mediated platelet activation) but without prior heparin exposure. The key clinical lesson: check platelet count in every CVST patient, and test for anti-PF4 antibodies in patients with recent adenoviral vector vaccine — heparin is contraindicated and IVIG is life-saving.
The TODAM registry (2022, 26 centers) reported outcomes of 70 endovascular-treated CVST patients, showing 73% functional independence at 90 days — providing the best contemporary data for a population at the severe end of the spectrum. The ongoing SWIFT DIRECT II trial is evaluating early mechanical thrombectomy + anticoagulation versus anticoagulation alone in severe CVST; results are expected to guide when endovascular treatment should be offered rather than reserved for rescue therapy.
Emerging biomarker research focuses on serum GFAP (astrocyte injury), NfL (axonal injury), and D-dimer trajectory as predictors of CVST severity and recanalization. Artificial intelligence analysis of MRI-MRV for automated sinus signal abnormality detection is under active development to reduce diagnostic delay.
12. References
- Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis. Stroke. 2004;35(3):664–670 — Search PubMed
- Coutinho JM, Ferro JM, Canhão P, et al. Cerebral venous and sinus thrombosis in women. Stroke. 2009;40(7):2356–2361 — Search PubMed
- Einhäupl K, Villringer A, Meister W, et al. Heparin treatment in sinus venous thrombosis. Lancet. 1991;338(8767):597–600 — Search PubMed
- de Bruijn SF, Stam J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke. 1999;30(3):484–488. PMID: 10066840
- Coutinho JM, Ferro JM, Zuurbier SM, et al. Dabigatran versus warfarin in cerebral venous thrombosis: RE-SPECT CVT trial. Stroke. 2019;50(11):3013–3021 — Search PubMed
- Greinacher A, Thiele T, Warkentin TE, et al. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med. 2021;384(22):2092–2101. PMID: 33835769
- Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791–1798. PMID: 15858188
- Saposnik G, Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous thrombosis. Stroke. 2011;42(4):1158–1192. PMID: 21293023
- Silvis SM, de Sousa DA, Ferro JM, Coutinho JM. Cerebral venous thrombosis. Nat Rev Neurol. 2017;13(9):555–565 — Search PubMed
- Dentali F, Gianni M, Crowther MA, Ageno W. Natural history of cerebral vein thrombosis: a systematic review. Blood. 2006;108(4):1129–1134. PMID: 16609071
- Ferro JM, Bousser MG, Canhão P, et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis — endorsed by the ESMINT and the ESNR. Eur J Neurol. 2017;24(10):1203–1213. PMID: 28833980
- Devasagayam S, Wyatt B, Leyden J, Kleinig T. Cerebral venous sinus thrombosis incidence is higher than previously thought: a retrospective population-based study. Stroke. 2016;47(9):2180–2182 — Search PubMed
PubMed Research Searches
- Cerebral venous sinus thrombosis anticoagulation treatment
- CVST diagnosis MRI MRV
- Cerebral venous thrombosis oral contraceptives thrombophilia
- VITT vaccine-induced immune thrombocytopenia and thrombosis CVST
- Cerebral venous thrombosis prognosis recanalization
Connections
- Neurology
- Transient Ischemic Attack (TIA)
- Stroke
- Intracranial Hypertension (IIH)
- Normal Pressure Hydrocephalus
- Migraine
- Epilepsy
- Vascular Dementia
- All Conditions
- Lab Tests
- Vitamin B12 (Homocysteine)
- Folate / Vitamin B9
- Headache — the cardinal presenting symptom of CVST, present in about 90% of cases and often the only one.