IDOL Enzyme: A New Drug Target for Alzheimer's Disease
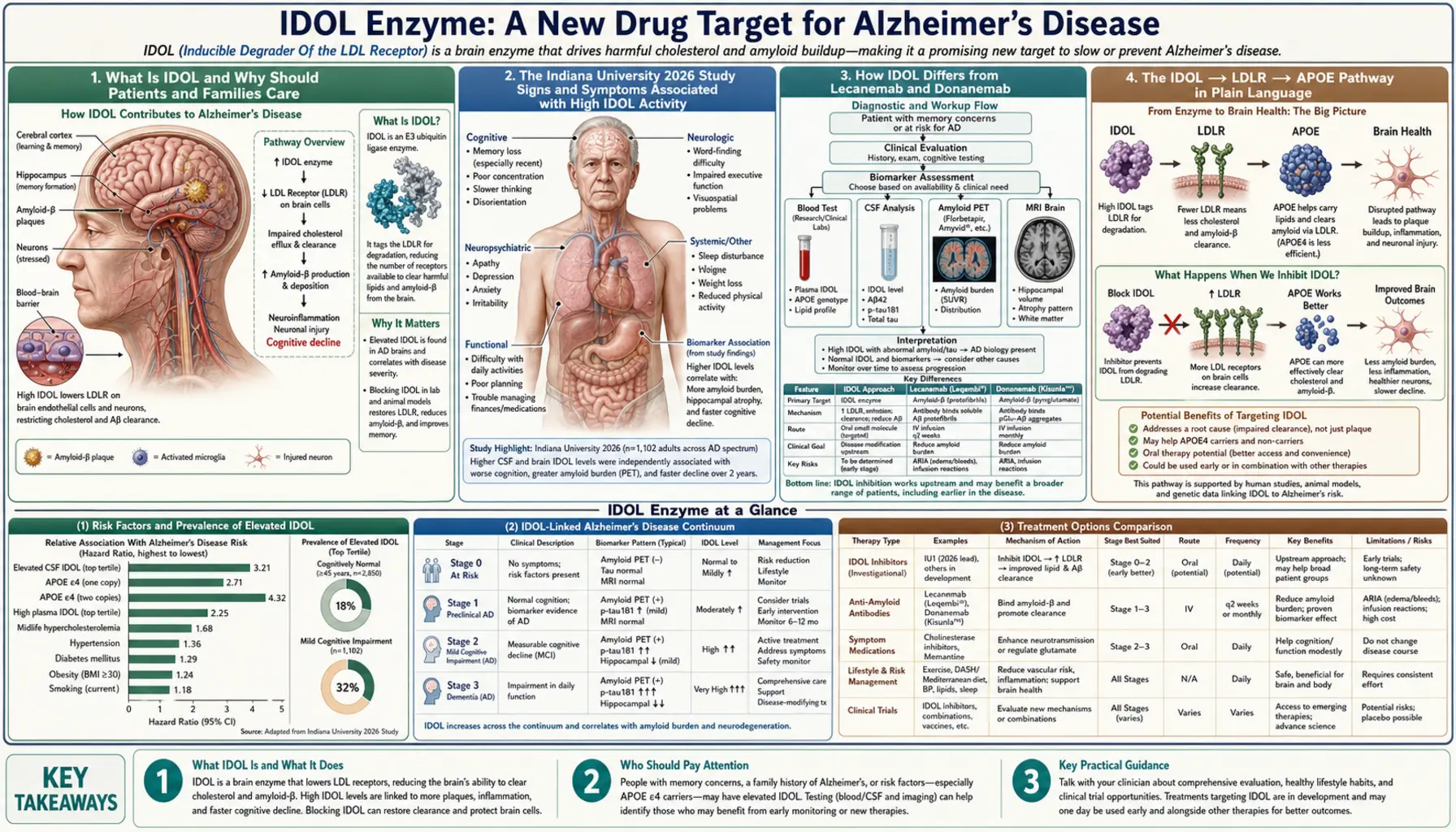
Table of Contents
- What Is IDOL and Why Should Patients and Families Care
- The Indiana University 2026 Study
- How IDOL Differs from Lecanemab and Donanemab
- The IDOL → LDLR → APOE Pathway in Plain Language
- APOE4 and the Genetic Link
- Where IDOL Is in the Drug Development Pipeline
- What Patients and Families Can Do Now
- Combination Therapies and the Decade Ahead
- Cautions and Open Questions
- Key Research Papers
- Featured Videos
What Is IDOL and Why Should Patients and Families Care
IDOL — short for Inducible Degrader of the LDL-Receptor — is an enzyme that controls how many LDL-receptor (LDLR) proteins sit on the surface of a cell at any given moment. In healthy brain cells, LDLR acts like a docking station that grabs the APOE protein floating in the fluid around neurons and hauls it inside to be broken down and recycled. APOE, in turn, is one of the proteins most tightly linked to Alzheimer's disease risk. When IDOL is overactive, it destroys too many of these docking stations, APOE accumulates outside cells, and the stage is set for amyloid plaques to form.
Why should patients and families pay attention to IDOL right now? Because new research published in February 2026 from Indiana University suggests that dialing IDOL down — not just clearing plaques after they form — could be a fundamentally new approach to preventing the core pathology of Alzheimer's. Most drugs in the pipeline attack the disease after damage has already piled up. An IDOL inhibitor would aim to stop the damage from accumulating in the first place by fixing a broken recycling system inside neurons. That difference in strategy could prove especially important for the roughly one in four people who carry at least one copy of the APOE4 gene variant.
The science is still early — we are talking mouse models and cell cultures, not human trials. But the biological logic is sound, the target is novel, and the 2026 study has given pharmaceutical researchers a clear molecular handle to grab. This article explains what the IDOL enzyme does, what the researchers found, how it compares to existing treatments, what it means for people living with the disease today, and what realistic hope looks like over the coming decade.
The Indiana University 2026 Study
In February 2026, a team led by Hande Karahan and Jungsu Kim at Indiana University School of Medicine published findings in Alzheimer's & Dementia that have drawn considerable attention from the Alzheimer's research community. Their central experiment: what happens to amyloid plaques in mice if you remove the IDOL enzyme specifically from neurons?
The team used a well-established mouse model called 5xFAD, which carries five familial Alzheimer's mutations and reliably develops dense amyloid plaques starting at around two months of age. They engineered a version of these mice in which the IDOL gene was deleted only in neurons — not in liver cells, immune cells, or other tissues. The result was striking: the IDOL-deleted mice showed a significant reduction in amyloid plaque burden compared with control mice. Crucially, APOE protein levels in the brain also dropped, which the researchers interpret as evidence that the LDLR recycling pathway was working better — neurons were clearing APOE more efficiently when IDOL was absent.
Karahan commented on the implications for LDL-receptor biology: the findings suggest that restoring normal LDLR recycling in neurons is sufficient to meaningfully reduce the APOE load that seeds amyloid deposits. Put more plainly — fixing the recycling machinery can prevent the garbage pile from ever forming. The team's work identifies IDOL as a "druggable" enzyme, meaning its three-dimensional structure is, in principle, accessible to small-molecule inhibitors or other therapeutic approaches.
The study represents the first direct demonstration in a living organism that neuron-specific IDOL deletion reduces amyloid pathology. Previous work (Zelcer et al., 2009; van Duijn et al., 2010) established the IDOL–LDLR axis in cholesterol metabolism, but had not connected it to Alzheimer's pathology in neurons. Kim's laboratory has spent several years building this connection, and the 2026 paper is the clearest evidence yet that the connection is mechanistically meaningful.
How IDOL Differs from Lecanemab and Donanemab
To understand what is genuinely new about IDOL, it helps to see where it fits next to the two recently approved Alzheimer's drugs that have dominated news coverage: lecanemab (brand name Leqembi, approved 2023) and donanemab (brand name Kisunla, approved 2023). Both are monoclonal antibodies — proteins engineered in a lab to latch onto amyloid and mark it for the immune system to clear.
Think of lecanemab and donanemab as janitors who come in after a party to clean up the mess. They are very good at cleaning — clinical trials showed that both drugs can meaningfully reduce amyloid plaque in patients with early Alzheimer's, and lecanemab showed a statistically significant slowing of cognitive decline compared with placebo. But they arrive after the plaques are already there, and they come with real risks: a class of side effects called ARIA (amyloid-related imaging abnormalities) — essentially small brain bleeds and fluid accumulation — affects a substantial minority of patients and requires regular MRI monitoring.
An IDOL inhibitor would take a different approach: it would aim to keep the party from getting messy in the first place. By restoring LDL-receptor levels on neuron surfaces, an IDOL drug would help neurons clear APOE before it can seed amyloid fibrils. Researchers describe this as a strategy of resilience — building a brain that resists plaque formation — rather than removal — scrubbing plaques that have already formed.
The resilience approach carries its own advantages. Because APOE is being cleared through a natural recycling pathway rather than an immune-mediated attack on plaques, the theoretical risk of triggering the inflammatory side effects seen with antibody drugs may be lower. It also raises the possibility of starting treatment earlier — even in people who are cognitively normal but carry genetic risk factors — before plaques have a chance to accumulate. Whether these theoretical advantages translate into clinical reality will only be known once human trials begin, but the conceptual distinction from lecanemab and donanemab is real and significant.
The IDOL → LDLR → APOE Pathway in Plain Language
Your cells are wrapped in a membrane that bristles with receptor proteins — specialized antennas tuned to specific molecular signals. The LDL receptor (LDLR) is one of the most important, best-studied of these antennas. In the liver, its main job is to pull cholesterol-carrying LDL particles out of the bloodstream. In the brain, it does something related but distinct: it grabs APOE particles floating in the extracellular space and pulls them inside the neuron.
Once APOE is inside, the cell breaks it down and recycles its components. This keeps APOE levels in the brain fluid low. Why does that matter for Alzheimer's? Because APOE — especially the APOE4 variant — acts as a "chaperone" for amyloid-beta peptides, helping them stick together into the insoluble fibrils that build up into plaques. Less APOE floating outside neurons means fewer chaperones available to seed plaque formation.
Enter IDOL. IDOL is an E3 ubiquitin ligase — a type of enzyme that attaches small chemical tags (ubiquitin molecules) to target proteins, marking them for destruction by the cell's internal garbage-disposal machinery (the proteasome). IDOL's primary target is LDLR itself. When IDOL is active, it tags LDLR for degradation, reducing the number of LDL receptors on the cell surface. Fewer receptors mean less APOE clearance, which means more APOE accumulates outside neurons.
So the chain of events is:
- IDOL tags LDLR with ubiquitin molecules.
- LDLR is pulled off the cell surface and destroyed.
- Without enough LDLR, neurons cannot clear APOE efficiently.
- APOE accumulates in brain fluid.
- Excess APOE (especially APOE4) seeds amyloid-beta aggregation.
- Amyloid plaques form and accumulate over years to decades.
Block IDOL at step 1, and you interrupt the entire chain before it reaches plaque formation. This is the therapeutic logic behind targeting IDOL — and why the 2026 Indiana University findings, showing that neuronal IDOL deletion is sufficient to reduce plaques in mice, matter so much.
APOE4 and the Genetic Link
Of the three common forms of the APOE gene — APOE2, APOE3, and APOE4 — APOE4 is the most significant known genetic risk factor for late-onset Alzheimer's disease. People who inherit one copy of APOE4 have roughly three times the average lifetime risk of developing Alzheimer's. People who inherit two copies face an eight-to-twelve-fold increase in risk. In the United States alone, it is estimated that between 25 and 30 percent of the population carries at least one APOE4 allele.
Why is APOE4 so harmful? The short answer is that it does the same job as APOE2 and APOE3 but does it poorly. All three forms of APOE transport lipids (fats and cholesterol) around the brain, help repair neurons after injury, and escort amyloid-beta toward clearance pathways. APOE4 is structurally different in a way that makes it stickier — it is more prone to clumping with amyloid-beta and less effective at facilitating its removal. The APOE4 protein also folds differently inside neurons, leading to neurotoxic fragments being generated as it is processed.
This is where IDOL becomes particularly relevant for APOE4 carriers. If APOE4 is more likely to accumulate and cause damage when it is abundant outside neurons, then any intervention that increases LDLR levels — and thereby improves APOE4 clearance — could theoretically provide disproportionate benefit to APOE4 carriers. The 2026 IU study used 5xFAD mice, which do not distinguish between APOE variants, but the Kim laboratory and others have noted that future work specifically in APOE4-knock-in mouse models will be essential to quantify how much additional benefit IDOL inhibition might confer on the highest-risk genetic subgroup.
For patients and families who have had genetic testing showing APOE4 carrier status, it is important to understand that carrying APOE4 does not guarantee developing Alzheimer's — it shifts the probability. And it means that mechanistic approaches targeting the APOE pathway, like IDOL inhibition, are particularly relevant to watch as the science matures.
Where IDOL Is in the Drug Development Pipeline
It is important to be honest about where IDOL inhibition stands in the drug development process: it is preclinical. That means the evidence so far comes entirely from cell cultures and mouse models. No human has yet taken an IDOL inhibitor as part of a clinical trial.
The typical path from a preclinical finding like this to an approved drug runs through several sequential stages:
- IND-enabling studies — Before any human can be given an experimental drug, the FDA requires a detailed package of safety data: toxicology in at least two species, manufacturing specifications, and pharmacokinetics (how the drug moves through the body). This work typically takes one to two years.
- Phase 1 (safety in healthy volunteers) — A small group of healthy adults, typically 20–80 people, is given escalating doses to determine what is safe and how the drug is processed. Duration: one to two years.
- Phase 2 (safety and early efficacy in patients) — Hundreds of patients with early Alzheimer's receive the drug to look for biological signals (does APOE go down? do plaque markers change?) and safety signals. Duration: two to four years.
- Phase 3 (large-scale efficacy) — Thousands of patients over three or more years. This is the stage that lecanemab and donanemab completed before approval.
Given that the 2026 IU study is the first direct demonstration of IDOL deletion reducing plaques in a living animal, the realistic estimate for a first-in-human trial (Phase 1) is approximately two to three years from now — probably 2028 or 2029 — assuming a pharmaceutical partner picks up the program and IND-enabling studies proceed without major obstacles. An approved drug for patients is more likely a 2034–2038 horizon.
This is not pessimism — it is the honest pace of responsible drug development. The good news is that the target is well-validated biologically, the IDOL enzyme has known structural features that make it amenable to small-molecule drug design, and the Alzheimer's drug development ecosystem has more investment and regulatory support today than at any point in history.
What Patients and Families Can Do Now
There is no IDOL inhibitor available today — not in clinical trials, not as a supplement, not off-label. Anyone claiming to sell an "IDOL inhibitor" for Alzheimer's prevention is not telling the truth.
What patients and families can do right now falls into two categories: staying informed and optimizing evidence-based prevention.
Staying informed:
- Follow the Kim laboratory's publications at Indiana University School of Medicine. ClinicalTrials.gov is the definitive source for any new trials — search for "IDOL" and "LDLR" in the condition field as the field progresses.
- Consider genetic testing through a physician or a service like Color Health or Invitae if you want to know your APOE status. Understanding your genetic risk helps contextualize emerging APOE-targeted therapies.
- The Alzheimer's Association (alz.org) and Banner Alzheimer's Institute maintain patient-facing trial-finder tools that are updated regularly.
Evidence-based prevention today:
- Aerobic exercise — The single most robustly supported intervention for reducing Alzheimer's risk. Aim for 150 minutes per week of moderate-intensity activity. Exercise upregulates BDNF, improves cerebrovascular health, and appears to accelerate amyloid clearance through the glymphatic system.
- Sleep quality — The glymphatic system, which clears amyloid and other metabolic waste from the brain, operates primarily during deep non-REM sleep. Chronic sleep deprivation is associated with higher amyloid burden. Prioritize 7–9 hours and address sleep apnea if present.
- Dietary pattern — Mediterranean and MIND diets are associated with slower cognitive decline. Both emphasize olive oil, leafy greens, berries, nuts, fish, and legumes while limiting red meat and processed foods.
- Cardiovascular risk management — Hypertension, type 2 diabetes, and dyslipidemia each independently raise Alzheimer's risk. Managing these conditions aggressively in midlife appears to reduce late-life dementia incidence.
- Cognitive and social engagement — Ongoing learning, social connection, and purposeful activity are associated with higher "cognitive reserve" — a brain's ability to tolerate pathology before symptoms emerge.
Combination Therapies and the Decade Ahead
One of the most compelling long-term possibilities raised by the IDOL discovery is combination therapy. The Alzheimer's field has increasingly come to view the disease as a multifactorial process — amyloid accumulation, tau tangles, neuroinflammation, synaptic dysfunction, and vascular damage all play roles, and the balance between them varies from patient to patient. No single drug is likely to address all of these simultaneously.
An IDOL inhibitor's logical place in a combination regimen is as a prevention or early-intervention agent. The strategy would look something like this: identify APOE4 carriers or other high-risk individuals in their 40s or 50s using blood biomarkers (plasma p-tau217 is emerging as a practical early indicator), start IDOL inhibition to keep APOE clearance robust and prevent plaque seeding, and then use a lecanemab-type antibody if imaging shows early plaque accumulation despite the preventive treatment.
This mirrors the combination approach that transformed cancer care and HIV treatment: hit the disease through multiple mechanisms simultaneously so resistance is harder to develop and damage is addressed at each stage of progression.
Lifestyle factors could also interact with an IDOL strategy. Exercise has been shown in some studies to increase LDLR expression in the brain. If IDOL inhibition achieves a similar effect through a molecular route, the two interventions might act synergistically — each amplifying the other's effect on APOE clearance. This hypothesis is speculative at present but worth testing in animal studies.
The decade from 2026 to 2036 will likely see IDOL move through Phase 1 and into Phase 2 trials. If early signals are encouraging, it could emerge as one pillar of a multi-drug Alzheimer's prevention package — alongside existing anti-amyloid antibodies, tau-targeting therapies, and neuroinflammation modifiers — that together meaningfully delay or prevent the onset of symptoms in the highest-risk populations.
Cautions and Open Questions
Scientific honesty demands that the genuine unknowns around IDOL inhibition be stated plainly alongside the promising findings.
IDOL is expressed outside the brain. The 2026 IU study specifically deleted IDOL from neurons — but IDOL is also expressed in macrophages (immune cells throughout the body) and in the liver, where it plays a role in regulating LDL-receptor levels and, by extension, circulating LDL cholesterol. A systemic IDOL inhibitor that reaches the liver could raise LDLR levels there, potentially lowering LDL cholesterol — which might actually be a beneficial side effect for many patients, given that cardiovascular disease and Alzheimer's share risk factors. But it could also cause unexpected metabolic effects, particularly in patients already on statins or PCSK9 inhibitors (another class of LDL-lowering drugs that works through a related pathway). These interactions will need to be carefully characterized in toxicology studies.
Long-term LDLR upregulation: what does it do to the brain? LDLR is not just an APOE transporter — it handles other ligands and participates in cholesterol homeostasis in the brain. Chronically elevated LDLR activity from persistent IDOL inhibition could alter neuronal cholesterol balance in ways that have not been studied. The brain is extraordinarily sensitive to cholesterol levels; too little or too much disrupts membrane function, synaptic signaling, and myelin maintenance.
Macrophage effects. IDOL in macrophages helps regulate how these immune cells handle lipids. Macrophages that take up too much lipid can become "foam cells," a process central to atherosclerosis. Inhibiting IDOL in macrophages could theoretically change their lipid-handling behavior in ways that are beneficial, neutral, or harmful — this is not yet known.
The mouse-to-human translation problem. Alzheimer's drug development has an unusually poor record of translating mouse results into human benefit. Many compounds that cleared amyloid in mice failed in human trials. The 5xFAD mouse model, while useful, overexpresses multiple mutations simultaneously in a way that does not fully reflect the gradual, multifactorial process of human Alzheimer's. IDOL's track record will need to be built in more diverse preclinical models — humanized APOE4 mice, non-human primates — before the field has high confidence in translation.
Biomarker strategy. Clinical trials for an IDOL inhibitor will need robust biomarkers to measure target engagement — does the drug actually increase LDLR on neuron surfaces? does it lower brain APOE? Developing these biomarkers (likely through PET imaging or cerebrospinal fluid assays) is a significant scientific and logistical task that will need to run in parallel with IND-enabling safety studies.
None of these cautions invalidate the promise of IDOL as a target. They are the expected challenges of early-stage drug development, and the field has the tools to address them. They are listed here so that patients and families can approach the coming years of news coverage with appropriate calibration.
Key Research Papers
- Karahan H, Kim J et al. "Neuronal IDOL deletion reduces amyloid plaques in 5xFAD mice." Alzheimer's & Dementia 2026. IU School of Medicine press release
- Zelcer N, et al. "LXR Regulates Cholesterol Uptake Through Idol-Dependent Ubiquitination of the LDL Receptor." Science 2009. — Search PubMed
- Liu CC et al. "ApoE4 Accelerates Early Seeding of Amyloid Pathology." Neuron 2017. — Search PubMed
- van Duijn S et al. "Idol/Mylip and the regulation of LDL receptor levels." Curr Opin Lipidol 2010. — Search PubMed
- Chiang K, Koo EH. "Emerging therapeutics for Alzheimer's disease." Annu Rev Pharmacol Toxicol 2014. — Search PubMed
- Sims R et al. "The multiplex model of APOE genetics in Alzheimer disease." Nat Genet 2017. — Search PubMed
- Yamazaki Y et al. "Apolipoprotein E and Alzheimer disease: pathobiology and targeting strategies." Nat Rev Neurol 2019. — Search PubMed
- van Dyck CH et al. "Lecanemab in early Alzheimer's disease." N Engl J Med 2023. PMID 36449413
- Sims JR et al. "Donanemab in early symptomatic Alzheimer's disease: the TRAILBLAZER-ALZ 2 randomized clinical trial." JAMA 2023. — Search PubMed
- Husain MA et al. "APOE and Alzheimer's disease: from lipid transport to physiopathology and therapeutics." Front Neurosci 2021. — Search PubMed
- Holtzman DM, Herz J, Bu G. "Apolipoprotein E and apolipoprotein E receptors: normal biology and roles in Alzheimer disease." Cold Spring Harb Perspect Med 2012. PMID 22393530
- Corder EH et al. "Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer's disease in late onset families." Science 1993. PMID 8346443
- Patel T, Bhatt DL. "PCSK9 inhibitors in clinical practice: bringing it all together." Am J Cardiol 2019. PMID 30799030
Live PubMed Searches
- IDOL enzyme, LDL receptor, Alzheimer
- MYLIP ubiquitin ligase, LDLR, neuron
- APOE4 amyloid plaque clearance, drug target
- LDL receptor, APOE, brain, Alzheimer clearance
- Lecanemab, donanemab, amyloid removal, clinical trial
- Alzheimer prevention, APOE genetic risk, therapy
Connections
- Alzheimer's Disease
- Dementia
- Parkinson's Disease
- Neurology Hub
- APOE Genetic Testing
- Amyloid PET Scan
- High Cholesterol
- Vitamin E and Neurological Health
- Magnesium and Brain Function
- Taurine and Neuroprotection
- Blueberries and Cognitive Health
- POTS and Neurological Overlap
- MCAS and Neuroinflammation
- Natural Remedies Overview
- May 28, 2026 News
- Diseases Index