Q Fever
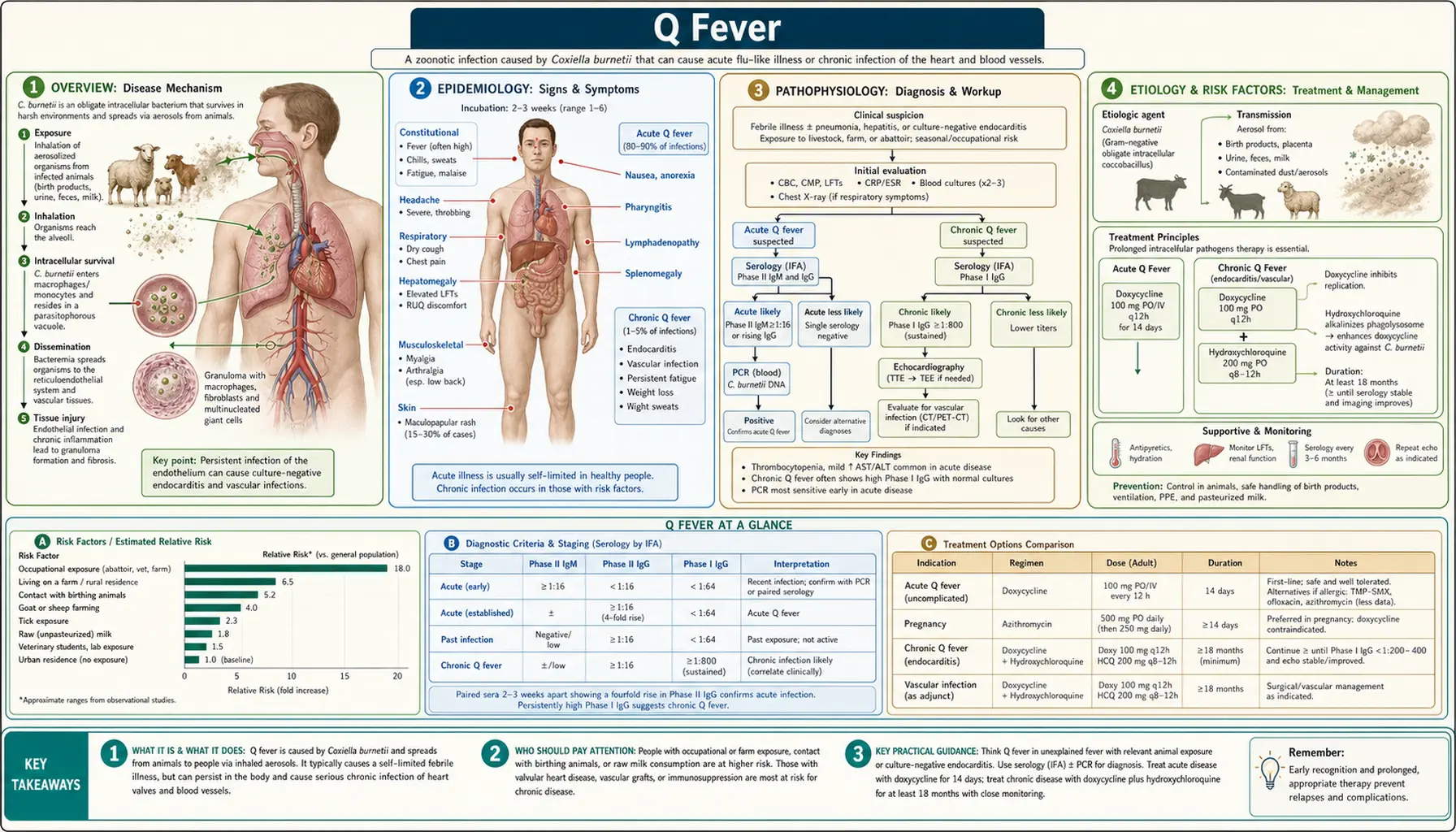
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research
- References
- Featured Videos
1. Overview
Q fever is a zoonotic infection caused by Coxiella burnetii, an obligate intracellular gram-negative bacterium. The "Q" stands for "query" — the name was assigned by Edward Derrick in Brisbane, Australia in 1937 when the disease first came to attention in abattoir workers and the causative organism had not yet been identified ("query fever"). Frank Burnet and Mavis Freeman isolated the organism in 1937; it was simultaneously and independently isolated in Montana by Herald Rea Cox and Gordon Davis — hence the name Coxiella burnetii combining both investigators' names.
Coxiella burnetii is exceptional among human pathogens for its extreme environmental resistance. It forms a small-cell variant (SCV) that functions as a spore-like form — it is not a true spore but behaves similarly, surviving months to years in soil, dust, and dried biological materials. It is highly resistant to heat, desiccation, ultraviolet light, and many disinfectants, and is considered the most environmentally resistant non-spore-forming pathogen known. Crucially, the infectious dose is estimated at as few as 1–10 organisms, making it one of the most infectious pathogens in nature and a Category B bioterrorism agent (CDC classification).
Q fever presents in two distinct phases: acute Q fever (a self-limiting febrile illness in most cases, with some developing pneumonia or hepatitis) and chronic Q fever (a severe, life-threatening syndrome developing months to years after primary infection in a minority of patients, almost always in the context of pre-existing cardiovascular or immunologic vulnerabilities, manifesting most dangerously as culture-negative endocarditis).
2. Epidemiology
Q fever is distributed worldwide (with the exception of New Zealand and Antarctica). Major outbreaks include: the Netherlands 2007–2010 (largest recorded Q fever outbreak — over 4,000 human cases linked to dairy goat farms with abortion storms; traced through wind dispersal of contaminated dust up to 5 km from farms); Australia (endemic, high incidence among abattoir workers and farmers); France (particularly southern France with high sheep density). Sporadic cases occur globally wherever livestock farming is practiced.
Reservoir animals: Sheep, goats, and cattle are the primary reservoirs. Infected females shed massive quantities of Coxiella burnetii during parturition — 109 organisms per gram of placenta. Cats (particularly during parturition), dogs, and rabbits may also be sources of human infection. Ticks (especially Dermacentor, Ixodes, and Amblyomma species) are competent hosts and contribute to animal-to-animal transmission but are not the primary route of human infection.
Incidence: Estimated 50 million people at risk globally; annual incidence is highly variable by region and dramatically underestimated due to subclinical cases (only 40–60% of primary infections cause recognizable illness). In the US, approximately 100–200 cases are reported annually to the CDC, with actual incidence likely much higher. Occupational risk groups include farmers, shepherds, veterinarians, abattoir workers, and hide and wool processors.
3. Pathophysiology
Coxiella burnetii is classified in Gammaproteobacteria (order Legionellales); historically grouped with Rickettsiales, but genomics has clarified its placement. Its cell biology is unique: it exploits a highly modified lysosomal vacuole for intracellular replication. Unlike most intracellular pathogens that escape phagosomal acidification, Coxiella paradoxically requires an acidic, hydrolase-rich phagolysosome-like vacuole (the "Coxiella-containing vacuole," CCV) — metabolic activity requires low pH (4.5–5.0). The CCV is a large, spacious parasitophorous vacuole derived from autophagolysosomal fusion, containing tens to hundreds of organisms.
Phase variation: C. burnetii expresses two distinct lipopolysaccharide phases. Phase I LPS (found in natural infections) has a full polysaccharide chain and is antigenically distinct from Phase II LPS (truncated O-antigen, expressed in laboratory-passaged organisms and vaccines). This phase variation is clinically critical: Phase I antibodies (particularly Phase I IgG ≥1:800) are the serological hallmark of chronic Q fever and endocarditis, while Phase II antibodies dominate in acute infection (Phase II IgG or IgM typically exceeds Phase I in acute disease). Monitoring Phase I IgG titers guides treatment duration.
Virulence mechanisms: The Dot/Icm Type IV secretion system (homologous to Legionella's system) injects effector proteins into the host cytoplasm that subvert CCV biogenesis, block apoptosis, modulate NF-κB signaling, and interact with the autophagy pathway. The SCV form resists environmental stress and facilitates aerosol transmission. In chronic infection, Coxiella persists despite apparently adequate antibiotic therapy due to its intracellular location — doxycycline alone cannot achieve sufficient intracellular concentrations; combination with hydroxychloroquine alkalinizes the CCV, dramatically improving antibiotic efficacy.
4. Etiology and Risk Factors
Causative organism: Coxiella burnetii (single species, though genomic groups are recognized). The primary route of human infection is inhalation of contaminated aerosols and dusts — from birth products, placenta, amniotic fluid, feces, urine, or wool from infected animals. An estimated infectious dose of 1–10 organisms via aerosol makes this exceptionally efficient. Other routes include ingestion of raw or unpasteurized dairy products (especially goat and sheep milk), contact with infected animals or contaminated materials through skin abrasions, and rarely tick bite.
Risk factors for acquisition:
- Occupational exposure to parturient livestock (especially goats and sheep at lambing)
- Proximity to farms or abattoirs (wind-borne spread documented up to 5–10 km from source)
- Processing hides, wool, or fertilizer from animal products
- Veterinary practice or animal research laboratory work
- Laboratory exposure to Coxiella cultures or infected specimens (BSL-3 pathogen)
Risk factors for progression to chronic Q fever:
- Pre-existing valvular heart disease (native or prosthetic) — the single most important risk factor
- Vascular prostheses or grafts
- Immunosuppression (HIV, chemotherapy, organ transplant, immunosuppressive medications)
- Pregnancy
- Chronic kidney disease
- Congenital heart disease
Approximately 1–5% of primary infections progress to chronic Q fever; among those with pre-existing valve disease, risk approaches 30–40%.
5. Clinical Presentation
Acute Q Fever (incubation period 2–6 weeks)
40–60% of primary C. burnetii infections cause recognizable illness; the remainder are subclinical and detected only by serology.
- Classic presentation: Abrupt onset of high fever (38.5–40°C), severe headache (often frontal, described as "splitting"), profound myalgia and fatigue, chills, and diaphoresis.
- Pneumonia (20–40% of symptomatic cases): Atypical pneumonia with dry cough, dyspnea, pleuritic chest pain; chest X-ray shows patchy consolidation, ground-glass opacities, or pleural effusions. Clinically and radiographically indistinguishable from Legionella, Mycoplasma, or Chlamydophila pneumonia.
- Hepatitis (30–40%): Elevated transaminases (typically 2–5× ULN), hepatomegaly; liver biopsy shows the distinctive "doughnut granuloma" (fibrin ring granuloma with a central lipid vacuole) — pathognomonic for Q fever hepatitis though not universally present; rarely fulminant hepatic failure.
- Pericarditis and myocarditis: Uncommon but recognized; pericarditis may cause chest pain and friction rub.
- Meningoencephalitis: Rare (<1%); aseptic meningitis, encephalitis, or Guillain-Barré syndrome.
- Rash: Uncommon (~10%); maculopapular or purpuric.
- Course: Self-limited in most patients; fever resolves within 2–3 weeks, though fatigue may persist for months.
Chronic Q Fever (develops months to years after primary infection)
- Culture-negative endocarditis (~65–70% of chronic Q fever): Almost always on previously abnormal or prosthetic valves; insidious onset; symptoms of weight loss, night sweats, clubbing, hepatosplenomegaly, purpura (immune complex deposition); absent or low-grade fever; new or changing murmur; embolic events; anemia of chronic disease. Diagnosis is often delayed months to years.
- Vascular infections (~15%): Aortic aneurysm infection, vascular graft infections — present as bacteremic febrile illness or local signs.
- Persistent granulomatous hepatitis.
- Osteomyelitis: Rare.
- Post-Q fever fatigue syndrome (QFFS): 10–20% of acute Q fever patients develop persistent fatigue, musculoskeletal pain, and cognitive impairment persisting more than 6 months (similar to myalgic encephalomyelitis/chronic fatigue syndrome; immune dysregulation has been proposed as the biological basis).
6. Diagnosis
Serology — indirect immunofluorescence assay (IFA): Gold standard for diagnosis. The critical distinction between acute and chronic Q fever rests on phase-specific antibody titers:
- Acute Q fever: Phase II IgG ≥1:200 AND/OR Phase II IgM ≥1:50 (Phase II antibodies dominate acutely).
- Chronic Q fever (endocarditis/vascular): Phase I IgG ≥1:800 — this criterion is highly specific for chronic infection (sensitivity ~95–100%, specificity ~90%). Phase I IgG <1:800 argues strongly against chronic Q fever. Monitor Phase I IgG titers during treatment — the treatment goal is a 4-fold decline by 18 months.
PCR (real-time PCR on blood): Highly sensitive during the acute febrile phase (blood PCR positive in 70–80% in the first 2 weeks of illness); sensitivity drops significantly after antibiotic initiation. Useful on valve tissue and vascular graft material obtained at surgery. Can distinguish Coxiella genotypes for outbreak investigation.
Culture: Performed only at BSL-3 reference laboratories; not routine clinical practice due to extreme biohazard risk.
Echocardiography: Mandatory for all confirmed C. burnetii infection — evaluate for valve disease that predisposes to chronic Q fever. Also diagnostic in suspected endocarditis (vegetations may be small or absent on transthoracic echo — transesophageal echocardiography is preferred).
Liver biopsy: Fibrin ring granuloma ("doughnut granuloma") on biopsy is highly suggestive of Q fever hepatitis, though not always present.
FDG-PET/CT: Increasingly used to detect occult vascular infection, aortic aneurysm seeding, or extracardiac chronic foci — now recommended as part of the chronic Q fever diagnostic workup.
7. Treatment
Acute Q Fever
- Doxycycline 100 mg PO twice daily × 14–21 days — first-line; started early, markedly shortens fever duration (from a median of 15 days untreated to 4–5 days with treatment).
- Fluoroquinolones (moxifloxacin, ofloxacin): Second-line alternative for patients who cannot tolerate doxycycline.
- Hydroxychloroquine is NOT needed for acute uncomplicated Q fever.
- Pregnancy: TMP-SMX (960 mg twice daily) throughout pregnancy until 5 weeks postpartum — doxycycline is contraindicated in pregnancy; pregnancy increases the risk of fetal loss and chronic Q fever.
Chronic Q Fever (Endocarditis/Vascular)
- Doxycycline 100 mg PO twice daily + Hydroxychloroquine 200 mg three times daily (600 mg/day), minimum 18 months for native valve endocarditis, ≥24 months for prosthetic valve endocarditis or vascular infection.
- Rationale for combination: Hydroxychloroquine alkalinizes the acidic CCV, enhancing doxycycline's intracellular bactericidal activity (MBC decreases 8-fold at pH 7.0 vs pH 4.5); prevents emergence of doxycycline tolerance; reduces relapse rate from ~50% (doxycycline alone) to <5% (combination).
- Monitoring: Phase I IgG titers every 3–6 months (target 4-fold decline); hydroxychloroquine plasma levels; ophthalmologic monitoring for retinal toxicity (hydroxychloroquine cumulative dose concern).
- Valve surgery: Required in many endocarditis patients due to hemodynamic deterioration, large vegetations, or embolic events; antibiotic continuation for ≥18 months post-surgery.
- Alternative regimen: Doxycycline + ofloxacin/moxifloxacin for patients unable to tolerate hydroxychloroquine.
- Treatment endpoint: Phase I IgG ≤1:200 for two consecutive tests ≥6 months apart is the proposed serologic cure criterion.
8. Complications
- Chronic Q fever endocarditis: Mortality 5–10% with optimal treatment, up to 30–60% if untreated or inadequately treated.
- Vascular graft or aneurysm infection: Often catastrophic if missed; requires prolonged antibiotic therapy and frequently surgical intervention.
- Stroke and systemic embolism from endocarditis vegetations.
- Chronic relapsing hepatitis.
- Osteomyelitis (rare).
- Post-Q fever fatigue syndrome (QFFS): Persistent fatigue, cognitive impairment, and musculoskeletal pain lasting months to years.
- Adverse pregnancy outcomes: Spontaneous abortion, preterm delivery, low birth weight, and fetal death — particularly with primary infection in the first trimester.
- Hydroxychloroquine retinal toxicity: Cumulative dose-dependent; requires routine ophthalmologic monitoring during long-term treatment.
9. Prognosis
Acute Q fever: Excellent with treatment; fatal outcomes are rare (<1%). Self-limited even without treatment in most patients, though fever duration is significantly shortened with doxycycline. Post-Q fever fatigue syndrome affects 10–20% of patients and may persist for years.
Chronic Q fever: Without diagnosis or treatment, mortality for endocarditis exceeds 50% within 2 years. With the doxycycline + hydroxychloroquine combination for a minimum of 18 months: survival approximately 95%, serologic cure approximately 75% at 5 years, relapse rate <5%. Predictors of poor outcome include delayed diagnosis, prosthetic valve involvement, immunosuppression, treatment duration <18 months, and failure of Phase I IgG titers to decline.
10. Prevention
Q-VAX (CSL Biotherapies): A whole-cell inactivated vaccine licensed in Australia (2001); not FDA-approved in the United States. Highly effective (>95% protection) in seronegative at-risk individuals (abattoir workers, veterinarians, research workers). Requires pre-vaccination skin test and serology — sensitized individuals may develop severe local reactions if vaccinated without screening. Recommended for Australian workers in high-risk occupations.
Occupational protective measures:
- Personal protective equipment (gloves, masks, eye protection) during animal parturition
- Decontamination of potentially contaminated materials and work surfaces
- Restricted access to lambing and calving areas for non-essential personnel
- Proper disposal of placental and birth materials from infected animals
Public health measures:
- Pasteurization of dairy products eliminates foodborne transmission risk
- Notification of animal Coxiella outbreaks to public health authorities
- Screening high-risk patients (valvular heart disease, immunosuppression, pregnancy) in endemic areas after exposure
No human vaccine is licensed outside Australia. Laboratory workers handling specimens or cultures must work under BSL-3 containment conditions.
11. Recent Research
Netherlands outbreak investigation (2007–2010): The largest recorded community Q fever outbreak defined the spatial extent of aerosol dispersal and enabled refined risk mapping; the investigation revealed a high chronic Q fever burden in goat-farming regions and the role of abortion storms as the proximate source of environmental contamination.
FDG-PET/CT for chronic Q fever staging: Enabling detection of occult vascular foci not visible on echocardiography or conventional CT; now recommended as part of the chronic Q fever diagnostic workup for all confirmed cases of chronic infection.
Coxiella genomics: Whole-genome sequencing has enabled SNP-based genotyping that can link human cases to specific animal sources during outbreak investigations, improving public health response capability.
Post-Q fever fatigue syndrome pathophysiology: Ongoing research into immune dysregulation, persistent low-grade Coxiella antigen stimulation, and shared mechanisms with myalgic encephalomyelitis/CFS; trials of cognitive behavioral therapy and graded exercise therapy have shown modest benefit.
Novel treatment endpoints: Phase I IgG titer decline kinetics and FDG-PET normalization are being evaluated as objective treatment endpoints for chronic Q fever, potentially enabling more individualized decisions about treatment duration.
Dot/Icm effector function: Recent structural biology studies of the Type IV secretion system effectors are identifying potential drug targets and vaccine antigens beyond the current whole-cell vaccine approach.
12. References
- Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12:518–553. PMID: 10515901. https://doi.org/10.1128/CMR.12.4.518
- Raoult D, Tissot-Dupont H, Foucault C, et al. Q fever 1985–1998. Clinical and epidemiologic features of 1,383 infections. Medicine. 2000;79:109–123. PMID: 10771709. https://doi.org/10.1097/00005792-200003000-00005
- van der Hoek W, Dijkstra F, Schimmer B, et al. Q fever in the Netherlands: an update on the epidemiology and control measures. Euro Surveill. 2010;15:19520. PMID: 20430028. https://doi.org/10.2807/ese.15.12.19520-en
- Fenollar F, Thuny F, Xeridat B, et al. Endocarditis after acute Q fever in patients with previously undiagnosed valvular heart disease. Clin Infect Dis. 2006;42:818–821. PMID: 16477562. https://doi.org/10.1086/500524
- Botelho-Nevers E, Fournier PE, Richet H, et al. Coxiella burnetii infection of aortic aneurysms or vascular grafts: report of 30 new cases and evaluation of outcome. Eur J Clin Microbiol Infect Dis. 2007;26:635–640. PMID: 17618468. https://doi.org/10.1007/s10096-007-0357-6
- Millar JA, Millar-Price L, Ormiston TM. Q fever endocarditis. QJM. 2000;93:491–493. PMID: 10874063. https://doi.org/10.1093/qjmed/93.8.491
- Raoult D, Marrie T, Mege J. Natural history and pathophysiology of Q fever. Lancet Infect Dis. 2005;5:219–226. PMID: 15792739. https://doi.org/10.1016/S1473-3099(05)70052-9
- Eldin C, Mélenotte C, Mediannikov O, et al. From Q fever to Coxiella burnetii infection: a paradigm change. Clin Microbiol Rev. 2017;30:115–190. PMID: 27856520. https://doi.org/10.1128/CMR.00045-16
- Frankel D, Richet H, Renvoisé A, Raoult D. Q fever in France, 1985–2009. Emerg Infect Dis. 2011;17:350–356. PMID: 21392421. https://doi.org/10.3201/eid1703.101348
- Camacho MT, Outschoorn I, Téllez A, Sequí J. Autoantibody profiles in the biological diagnosis of Q fever. Autoimmunity Reviews. 2005;4:375–378. PMID: 15990085. https://doi.org/10.1016/j.autrev.2005.02.007
- Million M, Thuny F, Richet H, Raoult D. Long-term outcome of Q fever endocarditis: a 26-year personal survey. Lancet Infect Dis. 2010;10:527–535. PMID: 20555326. https://doi.org/10.1016/S1473-3099(10)70135-3
- Marrie TJ. Q fever — a review. Can Vet J. 1990;31:555–563. PMID: 17423809. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1480654/
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Q Fever.
- Q fever Coxiella burnetii review
- Coxiella burnetii intracellular
- Q fever endocarditis doxycycline hydroxychloroquine
- Q fever chronic endocarditis
- Q fever Netherlands outbreak
- Coxiella burnetii phase antigen serology
- Q fever pneumonia atypical
- Q fever hepatitis granuloma
- Post-Q fever fatigue syndrome
- Q fever pregnancy outcomes
- Q fever vaccine prevention
- Coxiella burnetii bioterrorism
Connections
- Infectious Disease
- Brucellosis
- Typhoid Fever
- Lyme Disease
- Rocky Mountain Spotted Fever
- Pneumonia
- Endocarditis
- Hepatitis
- Meningitis
- Vitamin D3
- Garlic
- Immune Boosting
- Coxiella burnetii (Q Fever) — the bacterium behind this infection.