SIBO (Small Intestinal Bacterial Overgrowth): History and Discovery
Small intestinal bacterial overgrowth (SIBO) is, in plain terms, too many bacteria living in the wrong place — the small intestine, which is normally kept relatively sparse — producing bloating, gas, diarrhea, and sometimes malabsorption of nutrients. The idea did not arrive fully formed. Its deepest roots are in the mid-twentieth-century recognition of blind loop (or stagnant loop) syndrome, where a surgically created pouch, a stricture, or a pocket of stagnant bowel let bacteria multiply and rob the body of vitamin B12 and fat. From there the story runs through the classic diagnostic test of culturing fluid drawn from the upper small bowel, through the invention of non-invasive breath testing in the 1970s, and into a far more contested modern chapter: the proposal, advanced from the early 2000s, that SIBO is a major hidden cause of irritable bowel syndrome. This page traces that history honestly — including the parts that remain genuinely unsettled, where careful scientists still disagree.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →Table of Contents
- What SIBO Means — and Why History Matters
- Blind Loop and Stagnant Loop Syndrome: The Origin
- The Telltale Clues: B12 Deficiency and Fat Malabsorption
- The Classic Diagnosis: Jejunal Aspirate and the 105 Threshold
- Breath Testing: A Non-Invasive Window (1970s Onward)
- The Contested Turn: SIBO as a Cause of IBS
- Methane, Archaea, and the Reframing as IMO
- Where the Science Stands Today
- Research Papers and References
- Connections
- Featured Videos
What SIBO Means — and Why History Matters
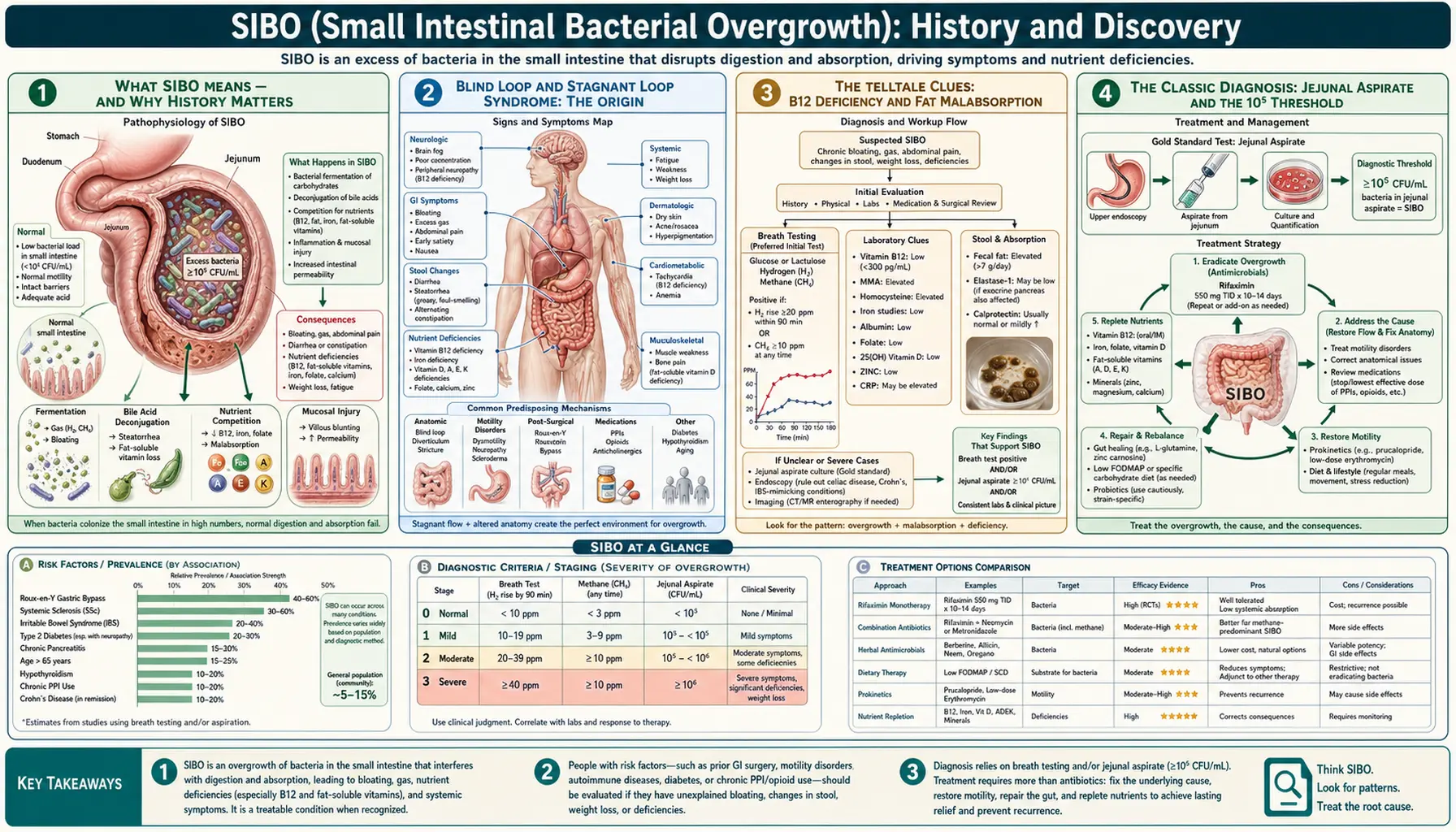
The small intestine is where most digestion and nutrient absorption happen. Unlike the colon, which teems with trillions of bacteria, the small bowel is normally kept relatively clean by a combination of stomach acid, bile, pancreatic enzymes, an intact intestinal wall, and the rhythmic sweeping contractions that move contents along. When those defenses fail and bacterial numbers climb too high in the small intestine, the result is what we now call small intestinal bacterial overgrowth. The microbes ferment carbohydrates before the body can absorb them, producing the gas and bloating that patients describe, and they can interfere with the absorption of fats and vitamins.
Understanding SIBO's history matters because the term covers two quite different things that have, over time, been blurred together. The first is a well-established, anatomically explained disorder — bacteria overgrowing behind a surgical blind loop, a stricture, or a pocket of stagnant bowel — that gastroenterologists have recognized and treated for more than seventy years. The second is a far broader and more controversial modern claim: that a milder, often invisible form of overgrowth underlies common functional gut complaints, especially irritable bowel syndrome. The same three letters carry both meanings, and much of the present-day debate comes from the gap between them.
This page therefore keeps a careful distinction throughout between what is settled and what is hypothesis. The classical syndrome rests on solid ground. The newer, expansive interpretation is influential, actively researched, and genuinely disputed — and it is presented here as such, with the uncertainty made plain rather than smoothed over.
Blind Loop and Stagnant Loop Syndrome: The Origin
The clinical roots of SIBO lie in the mid-twentieth-century recognition of blind loop syndrome, also called stagnant loop syndrome or, more generally, the bacterial overgrowth syndrome. The setting was usually surgical or anatomical: after certain stomach and intestinal operations, surgeons sometimes left behind a blind loop — a length of bowel that food bypassed and in which intestinal contents pooled and stagnated. Strictures (narrowings), small-bowel diverticula (out-pouchings), fistulas, and surgical anastomoses such as those of the Billroth II or Roux-en-Y reconstructions created similar pockets of stasis. Where contents stagnate, bacteria multiply.
An influential early thread runs back to 1939, when Barker and Hummel, writing in the Bulletin of the Johns Hopkins Hospital, described macrocytic anemia occurring together with intestinal strictures and surgical anastomoses — one of the earliest formal clinical descriptions linking abnormal small-bowel anatomy to a malabsorption picture. Over the following decades, experimental and clinical work established that the trouble was not the loop itself but the altered bacterial flora that flourished within it: investigators showed that the bacteria in a stagnant small-bowel loop come to resemble those of the colon, with a rise in organisms such as Escherichia coli and streptococci. The phrase "blind loop syndrome" entered the gastroenterology vocabulary to name this whole sequence — stasis, overgrowth, malabsorption.
It is fair to say that the names of the very first individuals to coin each term are not crisply or uncontroversially fixed in the literature, and this page does not attribute a single "discoverer." What is well documented is that by the 1950s and 1960s the syndrome was clearly characterized: anaerobic and colonic-type bacteria overgrowing in a stagnant segment of small bowel, causing anemia and malabsorption. This is the recognizable ancestor of the modern concept of SIBO, and the older literature is precisely where the threshold-based, culture-confirmed definition of overgrowth was forged.
The Telltale Clues: B12 Deficiency and Fat Malabsorption
Two laboratory and clinical findings became the classic fingerprints of bacterial overgrowth, and both make biological sense once you picture bacteria living where they should not. The first is vitamin B12 deficiency. In overgrowth, the resident bacteria consume dietary vitamin B12 in the small-bowel lumen before the body has a chance to absorb it further downstream, producing a deficiency that can show up as a macrocytic (large-red-cell) anemia — exactly the picture Barker and Hummel recorded in 1939. Adding to the puzzle's elegance, the same bacteria often synthesize folate, so overgrowth classically produces low B12 with normal or even high folate, a combination that helped clinicians recognize the syndrome.
The second fingerprint is fat malabsorption, which shows up as steatorrhea — pale, greasy, foul-smelling, hard-to-flush stools. Here the mechanism involves bile. Bacteria in the small intestine deconjugate bile acids prematurely, and without properly conjugated bile salts the gut cannot form the micelles needed to absorb dietary fat and the fat-soluble vitamins (A, D, E, and K). The result is fat in the stool, weight loss, and potential deficiencies of those vitamins. Damage to the brush border of the intestinal lining can add a degree of carbohydrate and protein malabsorption on top.
These two signatures — low B12 and fat malabsorption — anchored the classical understanding of bacterial overgrowth as a genuine cause of malnutrition, not merely a cause of discomfort. They also explain why the disorder was taken so seriously: a patient with a stagnant loop could become anemic and malnourished over time. Crucially, this severe, measurable malabsorption is far more characteristic of the anatomically driven overgrowth of blind loop syndrome than of the milder forms invoked in the later IBS debate, a distinction worth holding onto.
The Classic Diagnosis: Jejunal Aspirate and the 105 Threshold
For decades the reference standard for diagnosing bacterial overgrowth was direct and intuitive: sample the fluid, count the bacteria. Using a tube passed into the upper small intestine, clinicians aspirated fluid from the jejunum, cultured it, and counted the colonies. The historical diagnostic threshold that emerged from this work was 105 colony-forming units per milliliter (CFU/mL) — that is, one hundred thousand bacteria per milliliter of jejunal fluid was taken as the cut-off above which overgrowth was diagnosed. This jejunal (or duodenal) aspirate culture became known as the "gold standard."
That 105 figure, however, has a revealing back-story that bears directly on today's controversies. The high threshold was largely derived from patients with altered intestinal anatomy — the very blind-loop and post-surgical populations described above — in whom bacterial counts were dramatically elevated. When later investigators looked carefully at healthy people, they found that normal small-bowel bacterial counts rarely climb above roughly 102 to 103 CFU/mL. This mismatch prompted a re-examination, and modern expert reviews, including the 2017 North American Consensus and the American College of Gastroenterology, concluded that a lower threshold of 103 CFU/mL in a duodenal or jejunal aspirate more accurately identifies clinically meaningful overgrowth.
The aspirate method, for all its status as the reference standard, has well-recognized limitations that fueled the search for alternatives. The tube reaches only the upper small intestine and can miss overgrowth further down; the sample can be contaminated by mouth and throat bacteria on the way in; results vary with collection and culture technique; and fastidious anaerobes may not grow in culture at all. The procedure is also invasive, uncomfortable, and not widely standardized between laboratories. These shortcomings are a recurring theme: even the "gold standard" is imperfect, which is part of why the entire field has struggled to settle on firm diagnostic ground.
Breath Testing: A Non-Invasive Window (1970s Onward)
The desire for a test that did not require swallowing a tube led to hydrogen breath testing, which developed from the 1970s onward. The principle is clever and rests on a quirk of human biology: human cells cannot produce hydrogen gas, so essentially all the hydrogen in a person's breath comes from bacteria fermenting carbohydrate in the gut. Some of that hydrogen is absorbed into the bloodstream, carried to the lungs, and exhaled, where it can be measured. Give a patient a dose of sugar, then sample their breath at intervals, and a rise in exhaled hydrogen reflects bacterial fermentation.
The breath-hydrogen technique was pioneered for studying carbohydrate digestion — early work by investigators including Calloway and Murphy, and Levitt and Ingelfinger, established breath hydrogen as a measure of gut fermentation, and it was first applied clinically to diagnose lactose intolerance. It was then adapted to probe for bacterial overgrowth. Two sugars came into use for SIBO testing: glucose, a simple sugar normally absorbed high in the small intestine (so that an early hydrogen rise suggests bacteria are present where they should not be), and lactulose, a non-absorbable sugar that travels the length of the small bowel (used both for overgrowth testing and to estimate how long it takes contents to reach the colon). Later, devices were developed to measure exhaled methane as well as hydrogen, because a substantial minority of people harbor gut microbes that consume hydrogen and produce methane instead — an addition that would prove important to the story.
Breath testing's great advantage is that it is cheap, non-invasive, and widely available, which is exactly why it spread so quickly. But its accuracy for diagnosing SIBO is genuinely debated, and this is not a minor caveat. The lactulose test in particular can be confounded by how fast the sugar moves through the gut: a quick transit can deliver lactulose to the colon's dense bacteria and produce a hydrogen rise that looks like small-bowel overgrowth but is not. Critics have shown that lactulose breath testing does not reliably distinguish patients with suspected SIBO from healthy controls. To bring order to a chaotic field, the 2017 North American Consensus (Rezaie and colleagues) proposed standardized criteria — a rise in hydrogen of at least 20 parts per million by 90 minutes as positive for SIBO, and a methane level of at least 10 parts per million as methane-positive. These cut-offs are now widely used, but they are expert consensus rather than settled biological truth, and the underlying question of how well any breath test measures small-bowel bacteria remains open.
The Contested Turn: SIBO as a Cause of IBS
The most consequential — and most contested — chapter in SIBO's history began around the year 2000, when Mark Pimentel and colleagues proposed that small intestinal bacterial overgrowth is a major underlying cause of irritable bowel syndrome (IBS), the common functional gut disorder marked by abdominal pain, bloating, and altered bowel habits. In an influential 2000 paper, the group reported that a large majority of IBS patients — about 78 percent in their series — had abnormal lactulose breath tests, and that treating the presumed overgrowth with antibiotics improved IBS symptoms. The hypothesis was attractive: it offered a concrete, treatable bacterial explanation for a syndrome that had long lacked one, and it pointed toward the poorly absorbed antibiotic rifaximin as a therapy.
This idea has been enormously influential. It reframed how many clinicians and patients think about IBS, drove a wave of breath testing, and contributed to large trials of rifaximin for IBS. It is essential, however, to state clearly that the SIBO-causes-IBS hypothesis is not settled science — it is contested. The central criticisms are serious and come from within academic gastroenterology. First, the breath test used to build the hypothesis — the lactulose hydrogen breath test — may not actually have been measuring small-bowel overgrowth at all; an early hydrogen peak can simply reflect fast transit of lactulose into the colon. Second, when rigorous studies applied modern IBS criteria, lactulose breath testing failed to separate IBS patients from healthy controls — one widely cited critique was pointedly titled "another nail in the coffin." Third, even where antibiotics such as rifaximin help IBS symptoms, that benefit does not prove that bacterial overgrowth was the cause, since antibiotics have several effects on the gut and its broader microbiome.
The disagreement is live and recent. In 2024, a clinical practice update endorsed by the European Society of Neurogastroenterology and Motility (ESNM) and the American Neurogastroenterology and Motility Society (ANMS) offered a critical appraisal concluding that, after two decades, the SIBO hypothesis of IBS "remains unproven" and warning that it had encouraged the widespread use of unreliable, unvalidated breath tests and the over-use of antibiotics. Other expert bodies take a somewhat more permissive view of breath testing in selected patients. The honest summary is that a real and important link between gut bacteria and IBS symptoms is plausible and actively studied — but the specific claim that classically defined SIBO is the cause of most IBS has not been established, and reasonable experts continue to disagree.
Methane, Archaea, and the Reframing as IMO
One of the more important refinements of recent years concerns methane. Researchers noticed that a subset of patients — particularly those whose dominant symptom is constipation rather than diarrhea — produce large amounts of methane on breath testing, and that higher methane levels track with slower intestinal transit. This pointed to a different cast of microbes. The organisms responsible for methane are not bacteria at all but archaea, a separate domain of single-celled life. The principal gut methane-producer is Methanobrevibacter smithii, which consumes hydrogen generated by other microbes and converts it to methane.
Because these methane-makers are archaea rather than bacteria, the label "small intestinal bacterial overgrowth" is literally inaccurate for them — the "B" in SIBO does not fit. To address this, researchers (including Pimentel and colleagues) proposed the term intestinal methanogen overgrowth (IMO) to describe an excess of methane-producing archaea, distinguishing it from hydrogen-dominant, truly bacterial overgrowth. IMO is associated with constipation-predominant symptoms and with constipation-predominant IBS, and it is not necessarily confined to the small intestine, which is another reason the older "small intestinal" framing is a poor fit. A third pattern, involving hydrogen sulfide gas and linked more to diarrhea, has also been described as the field's gas-by-gas picture has grown more detailed.
The move from "methane-predominant SIBO" to "IMO" is a good example of science correcting its own terminology as understanding deepens — renaming a phenomenon to match its actual biology. It should be read in the same spirit as the rest of this history: a genuinely useful clarification (methanogens really are archaea, and really are linked to constipation) layered on top of the same unresolved core questions about how to test for these overgrowths reliably and how strongly they cause symptoms. The terminology is sharper than it was; the diagnostic certainty is not yet settled.
Where the Science Stands Today
Pulling the threads together, SIBO's history is really two histories sharing one name. The classical disorder — bacterial overgrowth behind a blind loop, stricture, or stagnant segment, causing B12 deficiency and fat malabsorption — is well established, mechanistically understood, and not in serious dispute. It is a real cause of malabsorption in people with the relevant anatomy or with conditions that impair the gut's clearing mechanisms, such as certain motility disorders, scleroderma, and the aftermath of some surgeries. For this classical picture, the historical jejunal-aspirate culture and the malabsorption fingerprints remain conceptually sound, even if the exact colony-count threshold has been revised downward over time.
The broader modern concept — SIBO as a common, often subtle driver of everyday digestive symptoms and especially of IBS — is where genuine scientific uncertainty lives. The diagnostic tools are imperfect and disputed: aspirate culture is invasive and samples only one spot, while breath testing is non-invasive but of debated accuracy, with the lactulose test particularly prone to confounding by transit time. The causal link to IBS is plausible and influential but unproven, and serious expert bodies have urged caution about both over-testing and over-treatment with antibiotics. At the same time, the refinement of methane-predominant overgrowth into IMO shows the field is still productively evolving.
For readers trying to make sense of this, the responsible takeaway is balance. SIBO is a real phenomenon with a solid historical and biological core, and for some patients diagnosis and treatment clearly help. But it has also been over-claimed, particularly online, as an explanation for a vast range of complaints on the strength of tests whose reliability is contested. Good care means working with a knowledgeable clinician, looking for treatable underlying causes, and keeping a healthy skepticism toward both blanket dismissal and over-diagnosis. The history of SIBO is, fittingly, a history still being written — and the most accurate thing this page can say is that the debate is real, the uncertainty is honest, and the science is ongoing.
Research Papers and References
The list below combines key peer-reviewed papers — cited with real DOIs or PMIDs where the reference is confidently identified — with curated PubMed topic-search links into the historical and clinical literature on bacterial overgrowth, breath testing, and the SIBO–IBS debate. Several foundational descriptions of blind loop syndrome predate online indexing and are named in the article as historical sources. Each link opens at the National Library of Medicine in a new tab.
- Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal bacterial overgrowth reduces symptoms of irritable bowel syndrome. American Journal of Gastroenterology. 2000;95(12):3503-3506. — doi:10.1111/j.1572-0241.2000.03368.x (PMID: 11151884) — the influential paper that launched the contested SIBO–IBS hypothesis.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. American Journal of Gastroenterology. 2017;112(5):775-784. — doi:10.1038/ajg.2017.46 (PMID: 28323273) — the standardized breath-test cut-offs (H2 ≥20 ppm by 90 min; methane ≥10 ppm).
- Kashyap P, Moayyedi P, Quigley EMM, Simren M, Vanner S. Critical appraisal of the SIBO hypothesis and breath testing: A clinical practice update endorsed by the European Society of Neurogastroenterology and Motility (ESNM) and the American Neurogastroenterology and Motility Society (ANMS). Neurogastroenterology & Motility. 2024;36(6):e14817. — doi:10.1111/nmo.14817 — the recent expert appraisal concluding the hypothesis remains unproven.
- Barker WH, Hummel LE. Macrocytic anemia in association with intestinal strictures and anastomoses (historical, 1939, Bulletin of the Johns Hopkins Hospital) — PubMed: early blind-loop / macrocytic anemia history
- Blind loop syndrome / stagnant loop syndrome — pathophysiology and bacterial overgrowth — PubMed: blind loop / stagnant loop syndrome
- Vitamin B12 deficiency and fat malabsorption in small intestinal bacterial overgrowth — PubMed: SIBO B12 deficiency and fat malabsorption
- Jejunal/duodenal aspirate culture and the 105 vs 103 CFU/mL diagnostic threshold debate — PubMed: jejunal aspirate culture and colony-count threshold
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020. — doi:10.14309/ajg.0000000000000501 (PMID: 32023228) — current guideline including the lowered diagnostic threshold.
- History and development of hydrogen breath testing (Calloway, Levitt, and colleagues; lactose origin, 1970s) — PubMed: history of hydrogen breath testing
- Lactulose breath testing and IBS — the accuracy critique ("another nail in the coffin") — PubMed 18371132: lactulose breath test in IBS critique
- Questioning the bacterial overgrowth hypothesis of irritable bowel syndrome — epidemiologic and evolutionary perspective — PubMed: questioning the SIBO–IBS hypothesis
- Intestinal methanogen overgrowth (IMO), Methanobrevibacter smithii, methane and constipation — PubMed: intestinal methanogen overgrowth (IMO)
- Rifaximin for irritable bowel syndrome and recurrence of bacterial overgrowth after antibiotics — PubMed: rifaximin in IBS and SIBO recurrence
- Conditions predisposing to SIBO — motility disorders, scleroderma, surgery, and the migrating motor complex — PubMed: SIBO risk factors and motility
External Authoritative Resources
- NIDDK (NIH) — Digestive Diseases
- MedlinePlus — Blind Loop Syndrome
- PubMed — All research on small intestinal bacterial overgrowth
Connections
- Gastroenterology
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO (Small Intestinal Bacterial Overgrowth) Hub
- Irritable Bowel Syndrome (IBS)
- Inflammatory Bowel Disease
- Celiac Disease
- Crohn's Disease
- Gastroesophageal Reflux Disease
- All Conditions