Eosinophilic Esophagitis
- Overview
- Epidemiology and Prevalence
- Pathophysiology — Th2 Immune Response
- Trigger Foods and Dietary Elimination
- Clinical Presentation
- Endoscopic Findings
- Diagnosis
- Treatment — PPI, Steroids, and Biologics
- Pediatric EoE
- Prognosis and Long-Term Management
- Research Papers
- Connections
- Featured Videos
Overview
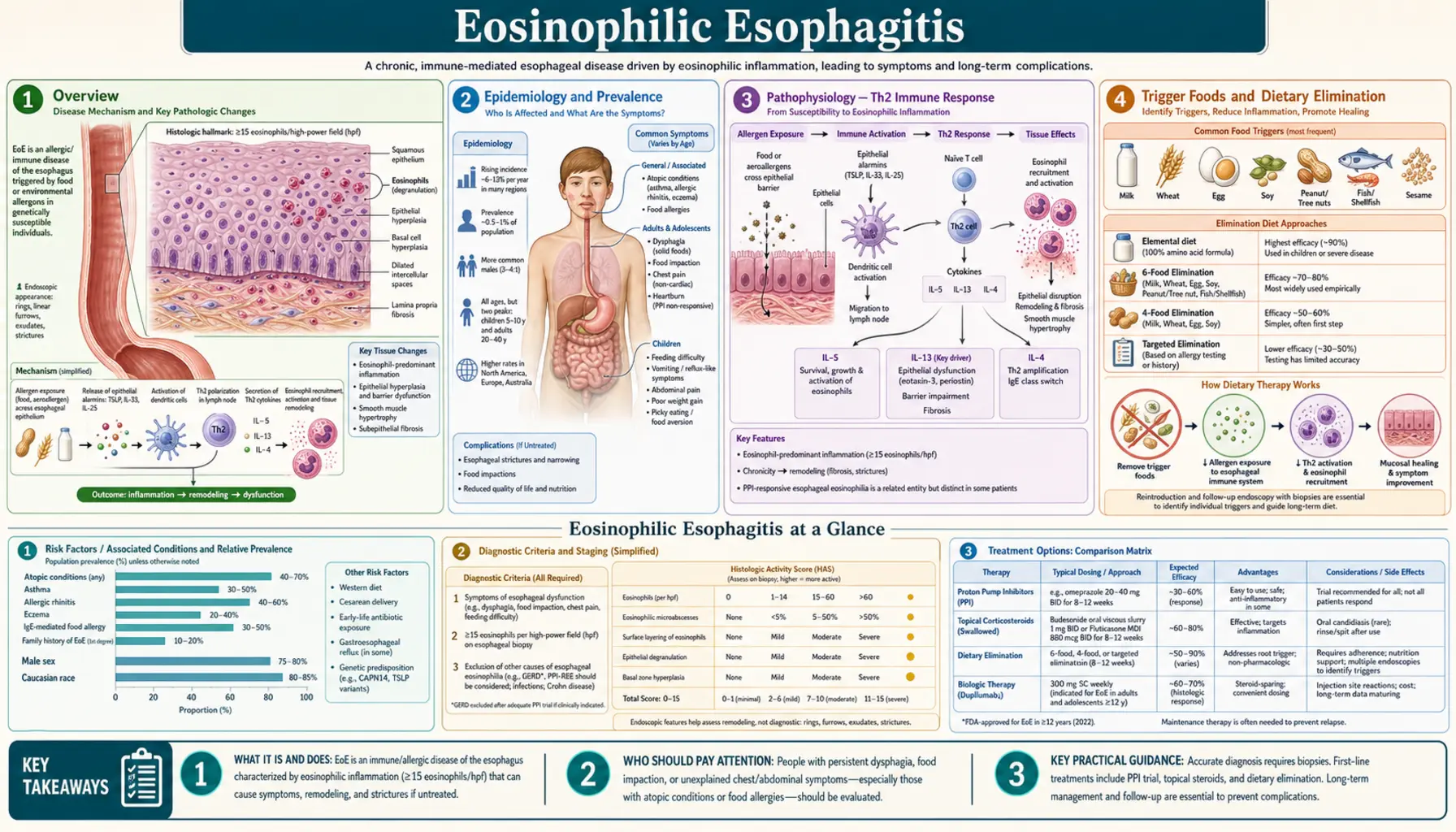
Eosinophilic esophagitis (EoE) is a chronic, antigen-driven, immune-mediated inflammatory disease of the esophagus. Unlike the stomach or intestine, the healthy esophageal epithelium contains no eosinophils at all — their presence in any number signals pathology. When eosinophils accumulate in the esophagus in response to food or environmental triggers, they cause both immediate inflammation and, over time, structural remodeling that narrows and stiffens the esophageal wall.
The hallmark diagnostic threshold is ≥15 eosinophils per high-power field (eos/HPF) on esophageal biopsy, alongside compatible symptoms and exclusion of other causes. EoE is emphatically distinct from gastroesophageal reflux disease (GERD): it is not driven by acid but by a Th2-skewed immune response involving interleukins IL-4, IL-5, IL-13, and the chemoattractant eotaxin-3 (CCL26).
EoE affects all ages but has a bimodal presentation — young children and adults — and is considerably more common in males (male-to-female ratio approximately 3:1). Prevalence is approximately 1 in 2,000 people in Western countries. Incidence has risen steadily since the disease was first clearly described in the early 1990s and is now estimated at 1–5 per 10,000 per year, making EoE one of the most important causes of upper gastrointestinal symptoms in both children and adults.
Epidemiology and Prevalence
EoE was barely recognized before 1993 but has since emerged as a major cause of esophageal disease across the Western world. Current prevalence estimates range from 34–56 per 100,000 in the United States and Europe, with some population-based studies exceeding 1 in 2,000. Whether this reflects a true rise in incidence or improved recognition — or both — remains debated, though most experts believe incidence genuinely increased through the 1990s and 2000s.
Age and sex distribution: EoE occurs at any age, from infancy through late adulthood, but two peaks dominate:
- Children and adolescents: Predominantly young boys. Symptoms tend to be nonspecific — food refusal, vomiting, abdominal pain, failure to thrive.
- Adults (20s–50s): Men outnumber women roughly 3:1. The cardinal complaint shifts to dysphagia and food impaction.
Atopic comorbidity: Approximately 70–80% of EoE patients carry at least one other atopic condition — asthma, allergic rhinitis, atopic dermatitis, or food allergy. EoE is increasingly understood as part of the atopic march, a developmental sequence of IgE-mediated and non-IgE-mediated allergic diseases. Patients with multiple atopic diagnoses, a family history of atopy, or early-onset allergic disease are at heightened risk.
Geography and environment: EoE is more prevalent in cold-climate, higher-altitude regions; less prevalent in tropical and subtropical settings. Aeroallergen exposure — specifically seasonal pollen — correlates with symptom flares, suggesting that environmental triggers play a role beyond food alone. The "old friends" hypothesis (reduced microbial exposure in early life) is also invoked to explain the parallel rise of EoE and other atopic diseases.
Pathophysiology — Th2 Immune Response
EoE is driven by a Th2-polarized adaptive immune response to ingested food antigens and, in some patients, inhaled aeroallergens. The sequence of events is distinct from GERD, which is mediated by acid and pepsin. In EoE, acid is incidental; the inflammatory engine is immunological.
Key molecular players:
- IL-5: The master cytokine for eosinophil survival, differentiation, and bone-marrow release. Blocking IL-5 reduces circulating and tissue eosinophils.
- Eotaxin-3 (CCL26): Produced by esophageal epithelial cells in response to IL-13 and allergen exposure, eotaxin-3 is the primary chemoattractant that draws blood eosinophils into the esophageal mucosa. CCL26 gene expression is markedly upregulated in EoE biopsies.
- IL-13: Drives epithelial barrier dysfunction (reducing filaggrin and desmoglein expression), promotes eotaxin-3 production, and stimulates subepithelial fibrosis via TGF-β signaling.
- IL-4 and TSLP (thymic stromal lymphopoietin): Amplify the Th2 response and promote mast cell activation.
- TGF-β: Secreted by eosinophils and mast cells, TGF-β activates esophageal fibroblasts, leading to subepithelial fibrosis — the structural change responsible for rings, strictures, and loss of esophageal compliance over years of untreated disease.
Barrier dysfunction: In EoE, the esophageal epithelial barrier is intrinsically weakened — filaggrin expression is reduced even in uninflamed EoE mucosa — allowing food antigens to penetrate into the lamina propria and contact antigen-presenting cells. This creates a self-reinforcing cycle: barrier damage permits antigen entry, which perpetuates inflammation, which further impairs barrier function.
Mast cells are prominent in EoE biopsies and contribute to immediate hypersensitivity symptoms (rapid-onset dysphagia after a specific food) as well as chronic remodeling through mediator release.
Trigger Foods and Dietary Elimination
Food antigens are the primary drivers of EoE in most patients. Unlike classic IgE-mediated food allergy (immediate hives/anaphylaxis), EoE reactions are non-IgE-mediated and delayed — symptoms worsen over weeks to months of exposure, not minutes. Standard allergy skin-prick or serum IgE testing is unreliable for identifying EoE trigger foods; repeated endoscopy is the only definitive test.
The "Big Six" trigger foods (eliminated in the six-food elimination diet, 6FED):
- Milk/dairy — the single most common trigger, implicated in 40–50% of cases
- Wheat/gluten-containing grains
- Eggs
- Soy
- Peanuts and tree nuts
- Seafood (fish and shellfish)
Step-up dietary approach: Because 6FED is burdensome (multiple repeat endoscopies over 6–12 months) and milk alone accounts for nearly half of triggers, many gastroenterologists now use a step-up protocol:
- 2-food elimination diet (2FED): Remove milk and wheat/gluten first. If histological remission (biopsy <15 eos/HPF) is achieved, reintroduce one food at a time with a 6–8 week trial and repeat endoscopy to confirm whether the reintroduced food caused relapse.
- 4-food elimination diet (4FED): Add eggs and legumes/soy if 2FED fails.
- 6FED: Full six-food removal for non-responders to 4FED.
Elemental formula (amino acid-based, completely allergen-free liquid diet) achieves histological remission in 90%+ of patients but is highly unpalatable, expensive, and impractical for adults. It is primarily reserved for children who fail dietary elimination or who require rapid symptom control.
Aeroallergen seasons (tree pollen in spring) can trigger or worsen EoE symptoms independent of diet, explaining why some patients improve with food elimination but never fully remit until aeroallergen exposure is also managed.
Clinical Presentation
EoE presents differently depending on age. The unifying theme is that symptoms relate to esophageal dysfunction — the inflamed, progressively fibrotic esophagus struggles to propel food normally.
Adults and older adolescents:
- Dysphagia — the cardinal symptom in adults. Patients describe progressive difficulty swallowing solids (bread, meat, rice) while liquids pass easily. Many develop behavioral adaptations over years: chewing excessively, eating slowly, drinking large amounts of water with meals, cutting food into tiny pieces, or avoiding dense solids entirely. By the time they seek care, the dysphagia has often been present for years.
- Food impaction — bolus impaction (food lodged in the esophagus requiring endoscopic removal) is the presenting emergency in 30–50% of adults at first diagnosis. The impaction itself is painful and frightening; the underlying esophageal narrowing is the structural consequence of years of untreated inflammation.
- Heartburn and chest pain — EoE mimics GERD closely, and many patients are treated for GERD for years before EoE is diagnosed. Unlike GERD, EoE-associated heartburn responds incompletely to acid suppression alone.
- Globus sensation — a persistent feeling of something stuck in the throat, even between meals.
- Regurgitation — undigested food returning to the mouth without nausea.
Children:
- Infants and toddlers: Feeding difficulties, refusal to eat certain textures, prolonged mealtimes, excessive drooling, vomiting.
- Older children: Abdominal pain, nausea, vomiting, food avoidance, failure to thrive in severe cases.
- Adolescents: Dysphagia and food impaction, mirroring the adult pattern, become more prominent.
Because symptoms overlap so substantially with GERD, functional dyspepsia, and anxiety-related eating disorders, the average delay from symptom onset to diagnosis in adults exceeds 4–6 years. Raising awareness of EoE is essential to shortening this diagnostic lag.
Endoscopic Findings
Upper endoscopy (esophagogastroduodenoscopy, EGD) is the primary diagnostic tool for EoE and the only way to obtain biopsies. Endoscopic findings are scored using the EoE Endoscopic Reference Score (EREFS), which assesses five features:
- E — Exudates: White plaques or spots representing eosinophilic microabscesses in the mucosa. Grade 0 (absent) to 2 (confluent plaques covering >10% of the esophageal surface).
- R — Rings (trachealization): Circular concentric rings creating a corrugated, trachea-like appearance — the so-called feline esophagus. Rings indicate subepithelial fibrosis and loss of distensibility. Grade 0 to 3.
- E — Edema: Mucosal pallor and loss of the normal vascular pattern. Edema reflects acute mucosal inflammation.
- F — Furrows: Vertical linear furrows running the length of the esophagus, created by longitudinal muscle contraction and mucosal folding over inflamed submucosa.
- S — Stricture: Fixed narrowing of the esophageal lumen. Strictures are the end-stage fibrostenotic consequence of longstanding EoE.
A critical pitfall: 10–30% of EoE patients have a normal-appearing endoscopy. The mucosa can look completely normal even when eosinophilic infiltration is severe histologically. This is why current guidelines mandate biopsy in all patients with dysphagia or food impaction, regardless of endoscopic appearance.
Biopsy protocol: at least 6 biopsies distributed between the proximal esophagus (upper third) and distal esophagus (lower third) are required, because EoE can be patchy. A single distal biopsy — standard in GERD evaluation — misses proximal-predominant or mid-esophageal disease in a meaningful proportion of patients.
The endoscopist should note mucosal friability ("crêpe paper" tearing on scope contact) — a sign of severe disease that also signals increased risk of mucosal laceration during esophageal dilation.
Diagnosis
The diagnosis of EoE requires all three of the following (2018 updated consensus definition, AGA/CAG):
- Symptoms of esophageal dysfunction (dysphagia, food impaction, heartburn, chest pain, feeding difficulties)
- Esophageal biopsy showing ≥15 eosinophils per high-power field (eos/HPF) on at least one specimen from the esophagus
- Exclusion of other causes of esophageal eosinophilia
Important 2018 update — PPI-responsive esophageal eosinophilia (PPI-REE): Prior to 2018, patients whose eosinophilia resolved on proton pump inhibitor (PPI) therapy were classified separately as "PPI-REE" and excluded from an EoE diagnosis. Current guidelines have abandoned this distinction. PPIs have direct anti-inflammatory and barrier-protective effects on the esophageal epithelium that are independent of acid suppression. PPI response does NOT rule out EoE — it is part of EoE treatment. A PPI trial is still recommended as a first-line step, but a response does not change the underlying diagnosis.
Differential diagnosis — other causes of esophageal eosinophilia to exclude:
- GERD: Acid-driven; typically <15 eos/HPF confined to the distal esophagus; responds to acid suppression
- Eosinophilic gastroenteritis: Eosinophils throughout the GI tract, not limited to the esophagus
- Hypereosinophilic syndrome: Systemic eosinophilia with organ involvement including heart, lungs, skin
- Achalasia: Esophageal motility disorder; can coexist with EoE but distinct mechanism
- Celiac disease, Crohn's disease, connective tissue disorders: Can be associated with esophageal eosinophilia
- Drug hypersensitivity reactions, parasitic infection: Rare but must be considered
Adjunctive testing: Esophageal string test (Cytosponge-like devices), esophageal impedance-planimetry (EndoFLIP — measures esophageal distensibility, an objective marker of fibrostenotic disease), and salivary/blood eosinophil counts are being studied as less-invasive monitoring tools but are not yet standard of care for initial diagnosis.
Treatment — PPI, Steroids, and Biologics
EoE management follows three therapeutic pillars: pharmacologic, dietary, and endoscopic. Most patients require long-term treatment, as EoE is a chronic relapsing disease — discontinuing therapy typically leads to histological and symptomatic relapse within weeks to months.
1. Proton pump inhibitors (PPIs) — first-line pharmacologic therapy
Twice-daily PPI therapy (e.g., omeprazole 20–40 mg, or equivalent) achieves histological remission in approximately 30–50% of EoE patients. The mechanism is not purely acid suppression — PPIs reduce eotaxin-3 expression and improve epithelial barrier function directly. All patients should receive a PPI trial at diagnosis. Responders may continue PPI monotherapy as maintenance. Non-responders proceed to topical steroids or dietary elimination.
2. Topical (swallowed) corticosteroids
- Swallowed fluticasone propionate: Actuated via metered-dose inhaler (MDI) without a spacer — the patient puffs into the mouth and swallows rather than inhaling. Doses vary (440–1760 mcg/day divided). Effective and inexpensive but requires patient education on proper swallowing technique.
- Budesonide oral suspension (BOS): A viscous slurry prepared from budesonide capsule contents mixed with sucralose; coats the esophageal mucosa more uniformly than inhaled fluticasone. Achieves histological remission in 50–70% in trials.
- Orodispersible budesonide tablet (Jorveza / Eohilia): Dissolved slowly on the tongue, the tablet delivers budesonide directly to the esophageal mucosa. FDA-approved in 2024 (as Eohilia) — the first FDA-approved pharmacological treatment specifically for EoE in adults. European approval (as Jorveza) was granted in 2018. Adrenal suppression is low but should be monitored with long-term use.
3. Biologic therapy — dupilumab
Dupilumab (Dupixent), a monoclonal antibody targeting the IL-4 receptor alpha subunit (IL-4Rα) — thereby blocking both IL-4 and IL-13 signaling — was FDA-approved for EoE in adults and adolescents ≥12 in 2022, the first biologic approved for EoE. In the pivotal PART A/B trials (Dellon et al., NEJM 2022), dupilumab 300 mg subcutaneous weekly achieved histological remission (peak eosinophil count <6 eos/HPF) in 59% versus 5% with placebo, and significantly improved dysphagia scores. It is approved for patients who have failed or cannot tolerate other options, and it also treats atopic dermatitis, asthma, and CRS with nasal polyps simultaneously — a significant advantage in the atopic EoE patient.
4. Dietary elimination
Described in detail in the Trigger Foods section above. For motivated patients, the step-up 2FED → 4FED → 6FED approach is preferred to maximize quality of life while minimizing unnecessary dietary restriction. Dietary therapy avoids systemic medication but requires multiple endoscopies and strict adherence.
5. Esophageal dilation
Dilation addresses fibrostenotic disease (rings, strictures) that does not resolve fully with anti-inflammatory therapy. It does not treat the underlying eosinophilic inflammation — it mechanically widens the lumen. Concerns about dilation causing perforation were historically overstated; modern series show perforation rates <0.5%. The main adverse effect is post-dilation chest pain (common, self-limiting over 1–3 days) and mucosal tearing ("crêpe paper" tears), which are superficial and rarely require intervention. Dilation may need to be repeated periodically if fibrosis recurs.
Pediatric EoE
EoE in children shares the same pathophysiological mechanism as adult disease but presents very differently, and the diagnostic challenge is compounded by children's difficulty articulating esophageal symptoms. A child who refuses food, eats very slowly, chews excessively, or has unexplained failure to thrive may have EoE rather than a behavioral feeding disorder.
Age-specific presentations:
- Infants (0–2 years): Feeding refusal, arching the back during feeds, spitting up, irritability. Indistinguishable clinically from infant GERD; EoE should be considered when standard GERD treatment fails.
- Toddlers and preschoolers (2–5 years): Food selectivity (strongly preferring soft textures, refusing meats or bread), prolonged mealtimes, gagging, choking episodes.
- School-age children: Abdominal pain, nausea, vomiting, food avoidance, poor appetite. Food impaction becomes more prominent as children enter adolescence.
- Adolescents: Adult-pattern dysphagia and food impaction, often after years of subtler symptoms.
Treatment in children: Dietary elimination (with elemental formula if needed) is preferred as first-line therapy in children given concerns about long-term corticosteroid exposure. Swallowed topical corticosteroids are used when dietary approaches are inadequate or impractical. Dupilumab is approved for adolescents ≥12 years. Endoscopic dilation is performed cautiously in children, usually only for significant strictures.
Growth and nutrition: Children with EoE who require extensive dietary elimination are at risk for nutritional deficiency and growth faltering. Dietitian involvement is essential to ensure adequate calories, calcium, protein, and micronutrients during elimination trials. When dairy is eliminated, vitamin D and calcium supplementation are particularly important.
School and social impact: EoE profoundly affects quality of life in children — anxiety around eating, social isolation at mealtimes, inability to participate in birthday parties or school lunches. Mental health support and school nurse education are underutilized but important parts of pediatric EoE management.
Prognosis and Long-Term Management
EoE is a chronic, lifelong condition in the majority of patients. Natural history studies (notably Straumann's landmark 11.5-year follow-up, Gastroenterology 2003) show that untreated EoE progresses from an inflammatory-predominant phenotype to a fibrostenotic phenotype over years. The key prognostic question is whether treatment prevents this structural remodeling — evidence increasingly suggests that it does.
Disease phenotypes over time:
- Inflammatory phenotype (early disease): Predominantly mucosal eosinophilia, edema, exudate, and furrows. Responsive to anti-inflammatory treatment. Reversible.
- Fibrostenotic phenotype (late disease): Rings, strictures, reduced esophageal distensibility. Results from years of untreated or undertreated inflammation driving TGF-β–mediated subepithelial fibrosis. Partially reversible with sustained therapy; may require dilation.
Relapse after treatment withdrawal: Most patients relapse histologically within 3–6 months of stopping therapy (steroids or dietary elimination), even if symptoms are slow to return. Long-term maintenance therapy is generally recommended for all patients who have achieved remission.
Monitoring: Current practice is to perform repeat endoscopy 6–12 weeks after initiating or changing therapy to confirm histological response (target: <15 eos/HPF, ideally <6 eos/HPF). Once in remission on stable therapy, surveillance endoscopy every 1–2 years is reasonable, though no consensus interval has been formally established. EndoFLIP distensibility measurement is emerging as a sensitive tool to detect ongoing subepithelial fibrosis not visible on standard endoscopy.
Risk of complications: Spontaneous esophageal perforation (Boerhaave-type) is rare but has been reported, particularly in patients with severe fibrostenotic disease. Food impaction requiring emergency endoscopy carries risk of mucosal injury and aspiration; patients should carry medical alert information. There is no established increased cancer risk in EoE — unlike Barrett's esophagus, EoE does not predispose to esophageal adenocarcinoma.
Quality of life: EoE substantially impairs quality of life through dietary restriction, fear of eating, social meal avoidance, and workplace impact (business meals, travel). Validated disease-specific patient-reported outcome measures (EEsAI, PEESS, DSQ) are increasingly used in both clinical trials and routine monitoring. Patients benefit from multidisciplinary care involving gastroenterology, allergy-immunology, dietetics, and when needed, psychology.
Research Papers
- Straumann A et al. Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years. Gastroenterology. 2003. PMID 11509120
- Furuta GT et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007. — Search PubMed
- Liacouras CA et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011. — Search PubMed
- Spergel JM et al. Efficacy of dietary interventions in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2012. — Search PubMed
- Dellon ES et al. ACG clinical guideline: evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013. — Search PubMed
- Molina-Infante J et al. Proton pump inhibitor-responsive esophageal eosinophilia: an entity challenging current diagnostic criteria for eosinophilic esophagitis. Gut. 2016. — Search PubMed
- Hirano I et al. AGA Institute and the Joint European Gastroenterology and European Academy of Allergy and Clinical Immunology technical review on the diagnosis and management of eosinophilic esophagitis. Gastroenterology. 2020. — Search PubMed
- Greuter T et al. Long-term treatment of eosinophilic esophagitis with swallowed topical corticosteroids: development and evaluation of a therapeutic concept. Am J Gastroenterol. 2017. — Search PubMed
- Kagalwalla AF et al. Identification of specific foods responsible for inflammation in children with eosinophilic esophagitis successfully treated with empiric elimination diet. J Pediatr Gastroenterol Nutr. 2011. — Search PubMed
- Dellon ES et al. Dupilumab in adults and adolescents with eosinophilic esophagitis. N Engl J Med. 2022. — Search PubMed
- Lucendo AJ et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017. — Search PubMed
- Katzka DA, Dellon ES. Eosinophilic esophagitis. JAMA. 2020. — Search PubMed
Connections
- GERD
- Dysphagia
- Celiac Disease
- Esophageal Stricture
- Crohn's Disease
- Food Allergy
- Barrett's Esophagus
- Gastritis
- Inflammatory Bowel Disease
- Herbs Overview