Insulin Resistance: History and Discovery
The story of insulin resistance is really three stories braided together: a concept, a measurement, and a syndrome. The concept that some people's tissues respond poorly to insulin was sketched out in the 1930s — most clearly by Harold Himsworth in 1936, building on earlier Viennese work — long before anyone could actually measure insulin in blood. That measurement only became possible in 1959–1960, when Rosalyn Yalow and Solomon Berson invented the radioimmunoassay and made the startling discovery that many people with type 2 diabetes have high, not low, insulin levels. Quantifying resistance precisely then took the euglycemic clamp (DeFronzo, 1979) and, for everyday use, the HOMA-IR index (Matthews and colleagues, 1985). Finally, Gerald Reaven's 1988 Banting Lecture tied insulin resistance to heart-disease risk as "Syndrome X." This page traces that arc, keeping a careful line between what was hypothesized and what was proven.
Interactive Visualization Blood Sugar & Insulin — eat a meal and watch glucose move Watch insulin escort glucose into cells and the liver bank glycogen, then switch on insulin resistance and see the curve change. Launch →Table of Contents
- Before Insulin: Diabetes as a Single Disease
- Two Kinds of Diabetes: Falta and the 1930s Idea
- Himsworth 1936: The Foundational Distinction
- The Measurement Breakthrough: Yalow and Berson's Radioimmunoassay
- A Counter-Intuitive Discovery: High Insulin in Type 2 Diabetes
- The Gold Standard: DeFronzo and the Euglycemic Clamp (1979)
- A Practical Index: HOMA-IR (1985)
- Reaven's Syndrome X: Insulin Resistance and the Heart (1988)
- From Syndrome X to the Modern Era
- Research Papers and References
- Connections
- Featured Videos
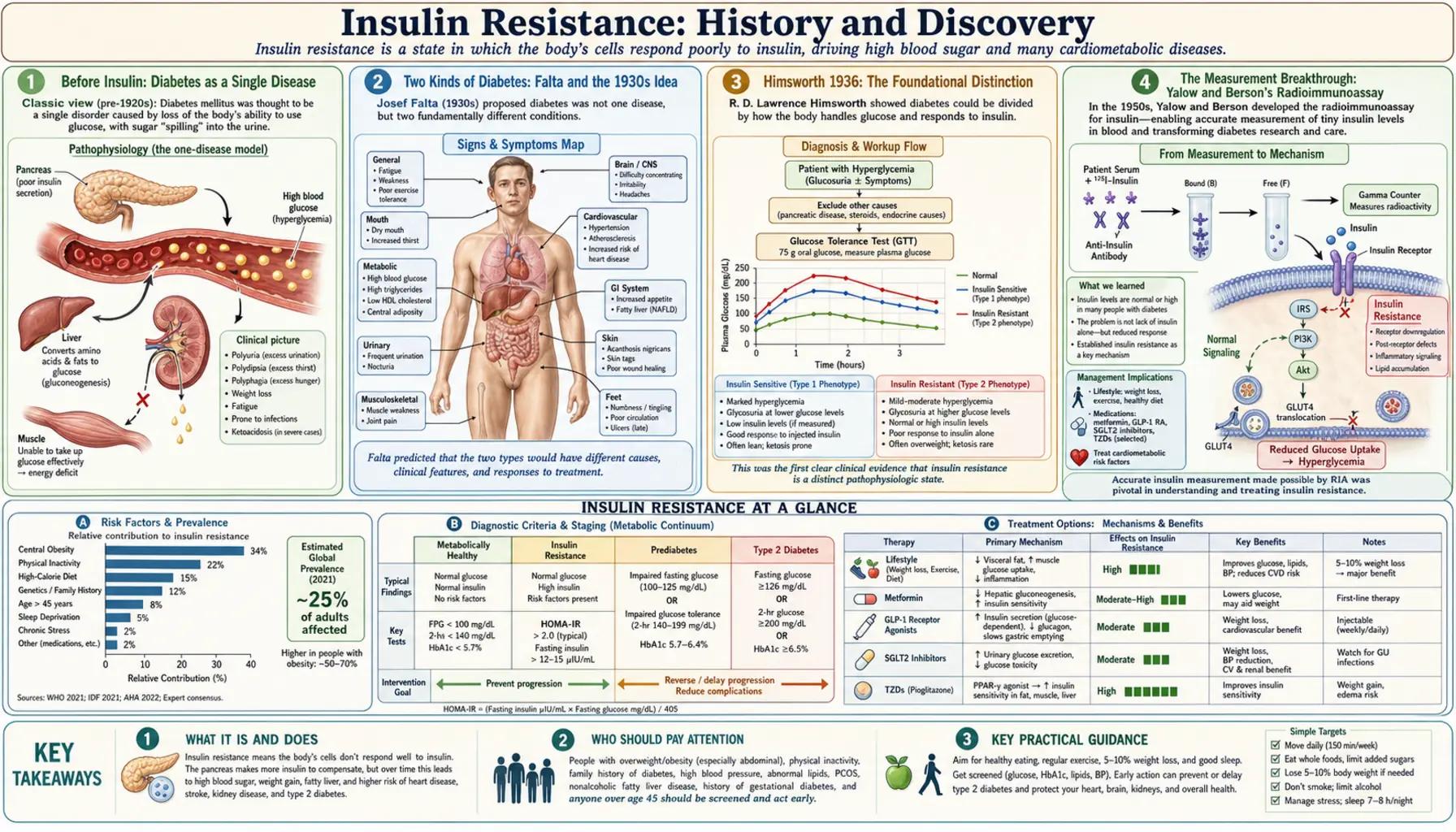
Before Insulin: Diabetes as a Single Disease
For most of medical history, diabetes was understood as one disease, recognized by its most dramatic sign: the sweet, copious urine that ancient physicians described and that gives the condition its name (diabetes mellitus, roughly "to pass through, honey-sweet"). Clinicians did distinguish, broadly, between the young patient who wasted away and died quickly and the older, often heavier patient whose course was slower and milder — but they had no way to explain why. The internal chemistry of the disease was invisible.
That changed in 1921–1922, when Frederick Banting, Charles Best, J.J.R. Macleod, and James Collip at the University of Toronto isolated insulin and showed that injecting it could rescue dying diabetic patients. Insulin's arrival was one of the great therapeutic miracles of the twentieth century, and it earned Banting and Macleod the 1923 Nobel Prize. But the very success of the new hormone immediately raised a puzzle that would take decades to unravel.
Within just a few years of insulin's introduction, physicians noticed that the drug did not behave the same way in every patient. Some people responded beautifully to small doses; others — often the older, heavier patients — needed surprisingly large amounts of insulin to bring their blood sugar down, and even then responded sluggishly. The hormone that explained so much had, paradoxically, exposed a deep difference between diabetics that pure insulin deficiency could not account for. Something else was going on.
Two Kinds of Diabetes: Falta and the 1930s Idea
The first serious attempts to explain this difference came in the late 1920s and early 1930s. The Viennese physician Wilhelm Falta is widely credited as one of the earliest to propose, in work published in Vienna around 1931, that a reduced sensitivity to insulin — rather than a simple shortage of it — distinguished one form of diabetes from another. In this telling, some patients lacked insulin, while others made insulin but could not use it effectively. The notion of insulin insensitivity, or resistance to insulin's action, was being born.
It is worth being precise about credit here, because popular accounts often compress the history. The general idea that the body might resist insulin was in the air in the 1930s and had more than one parent; Falta's Vienna work is the most frequently cited early statement of it. What was still missing, however, was a rigorous clinical demonstration in living patients — a way to show, at the bedside, that some diabetics genuinely responded less to a given amount of insulin than others did. That demonstration is what made the next step a landmark rather than a footnote.
This early-1930s phase belongs firmly to the concept-origin chapter of the story. No one could yet measure how much insulin a patient's own pancreas was producing, so "resistance" was an inference drawn from how patients behaved when insulin was injected — a clinical and conceptual argument, not a direct chemical one. That distinction between idea and measurement runs through the whole history and is the key to reading it accurately.
Himsworth 1936: The Foundational Distinction
The figure most associated with putting insulin resistance on a firm clinical footing is Sir Harold Percival Himsworth (1905–1993), working at University College Hospital in London. In 1936 he published a paper in The Lancet with the now-famous title "Diabetes Mellitus: Its Differentiation into Insulin-Sensitive and Insulin-Insensitive Types" (Lancet, 1936; volume 227, pages 127–130). In it he argued, from clinical testing, that diabetes was not one disease but at least two — one driven by a lack of insulin, and another in which insulin was present but the body failed to respond to it properly.
Himsworth devised tests in which he gave patients glucose together with insulin and watched how their blood sugar moved. Patients whose glucose fell readily he called insulin-sensitive; those whose glucose barely budged despite the injected insulin he called insulin-insensitive. He proposed that the insensitive type was not due to a shortage of insulin but to the lack of some factor needed to make tissues respond to it. In modern terms, he had drawn the essential line between what we now call type 1 (insulin-deficient) and type 2 (insulin-resistant) diabetes — and he had done it decades before insulin could actually be measured in blood.
Himsworth's achievement is best described as foundational rather than as the discovery of insulin resistance outright. He sharpened and clinically validated an idea whose seeds had been sown in the early 1930s, and he framed it so clearly that it became the conceptual backbone of everything that followed. Modern reviewers — including a 2011 retrospective in Diabetic Medicine marking 75 years since his paper, and a widely cited 2004 essay in Cell Metabolism tracing the line "from Harold Himsworth to the insulin resistance syndrome" — treat his 1936 work as the genuine starting point of the field. Himsworth later became a leading figure in British science as secretary of the Medical Research Council.
The Measurement Breakthrough: Yalow and Berson's Radioimmunoassay
For more than two decades after Himsworth, insulin resistance remained a concept that could be inferred but not directly weighed, because no one could measure how much insulin was actually circulating in a person's blood. The hormone exists in such tiny quantities that the chemistry of the day simply could not detect it. The breakthrough that finally cracked this open came not from a diabetes clinic but from a physics-and-medicine partnership at the Bronx Veterans Administration Hospital in New York.
There, the medical physicist Rosalyn Sussman Yalow (1921–2011) and the physician Solomon Aaron Berson (1918–1972) developed the radioimmunoassay (RIA) over 1959–1960. The method used radioactively labeled insulin and insulin antibodies in a competitive binding system so exquisitely sensitive that it could measure hormone concentrations far below anything previously possible. Yalow regarded 1959 as the year the era of radioimmunoassay genuinely opened. It was a general-purpose technique — it would soon be used to measure hundreds of substances — but insulin was where it began, and where it had its first revolutionary impact.
For their invention, Yalow was awarded the Nobel Prize in Physiology or Medicine in 1977 (shared with Roger Guillemin and Andrew Schally for related neuroendocrine work). She was only the second woman to win that prize. Berson, her essential collaborator, had died in 1972; because the Nobel Prize is not awarded posthumously, he could not share in it — a point Yalow herself stressed, and a poignant footnote to one of the most consequential partnerships in twentieth-century medicine.
A Counter-Intuitive Discovery: High Insulin in Type 2 Diabetes
When Yalow and Berson turned their new assay on patients, they made a discovery that was genuinely surprising and that confirmed Himsworth's decades-old inference in hard numbers. The reasonable expectation had been that all diabetics would have low insulin — after all, diabetes is a disease of high blood sugar, and insulin lowers blood sugar, so a shortage seemed the obvious culprit. That expectation held for the lean, young, insulin-dependent patients.
But in many of the older, heavier patients — the very group Himsworth had labeled "insulin-insensitive" — the assay revealed the opposite: their blood insulin was normal or even high, not low. Here was direct chemical proof that their problem could not be a simple lack of insulin. Their bodies were producing plenty of the hormone; the tissues were failing to respond to it. The pancreas, in fact, was working overtime, pumping out extra insulin to overcome the resistance — producing the state of high insulin (hyperinsulinemia) alongside high glucose that is a hallmark of insulin resistance.
This was the moment the concept earned its measurement. Himsworth had argued from how patients behaved; Yalow and Berson now showed the underlying chemistry. Insulin resistance was no longer merely a plausible interpretation of bedside tests — it was a measurable physiological state. The radioimmunoassay transformed insulin resistance from an idea into a phenomenon that could be quantified, studied, and eventually targeted, and it opened the door to the next question: exactly how much resistance does a given person have?
The Gold Standard: DeFronzo and the Euglycemic Clamp (1979)
Being able to measure insulin in a single blood sample was a giant step, but it did not, by itself, tell researchers precisely how sensitive or resistant a particular person's tissues were. A static reading could be muddied by how much insulin the pancreas happened to be secreting at that moment. What was needed was a controlled, dynamic test that could pin down insulin action directly. That tool arrived in 1979.
The endocrinologist Ralph A. DeFronzo, with Jordan D. Tobin and Reubin Andres, described the hyperinsulinemic–euglycemic glucose clamp in the American Journal of Physiology (1979; volume 237, issue 3, pages E214–E223), in a paper titled "Glucose clamp technique: a method for quantifying insulin secretion and resistance." The idea is elegant. Insulin is infused into the bloodstream at a fixed, steady rate to raise it to a chosen level, while glucose is simultaneously dripped in and continuously adjusted to keep blood sugar "clamped" at a normal (euglycemic) value. Once a steady state is reached, the amount of glucose being infused exactly equals the amount the body's tissues are taking up in response to that insulin.
That glucose-infusion rate becomes a direct, quantitative readout of whole-body insulin sensitivity: a person whose tissues respond well needs a lot of glucose to keep from going low, while an insulin-resistant person needs much less. Because it measures insulin action so directly and reproducibly, the euglycemic clamp became — and remains — the recognized gold standard for quantifying insulin resistance in research. It is labor-intensive and not practical for everyday clinical use, which is precisely why a simpler index was soon needed.
A Practical Index: HOMA-IR (1985)
The clamp is rigorous but demanding: it requires intravenous lines, hours of careful monitoring, frequent blood draws, and trained staff. It is wonderful for a research study of a few dozen volunteers and impossible for a busy clinic or a large population study. Researchers therefore wanted a way to estimate insulin resistance from something as simple as a single fasting blood sample. That practical index appeared in 1985.
David R. Matthews and colleagues at Oxford published the Homeostasis Model Assessment (HOMA) in Diabetologia (1985; volume 28, pages 412–419). They built a mathematical model of the feedback loop between the pancreas and the liver and showed that the product of fasting glucose and fasting insulin — both measurable from one ordinary blood draw — could be used to estimate both insulin resistance (HOMA-IR) and beta-cell function (HOMA-%B). The familiar simplified formula expresses HOMA-IR as fasting insulin times fasting glucose divided by a constant.
HOMA-IR is an estimate, not a direct measurement, and it is less precise than a clamp — an honest distinction worth keeping. But its convenience made it enormously influential: it requires nothing more than a fasting blood test, and it can be applied to thousands of people at once. That 1985 paper became the most-cited article in the history of Diabetologia, and HOMA-IR remains, four decades later, the workhorse index of insulin resistance in clinical research and increasingly in patient care. The practical fasting-insulin and HOMA-IR testing that grew out of this work is covered in the companion Fasting Insulin and HOMA-IR Testing article.
Reaven's Syndrome X: Insulin Resistance and the Heart (1988)
By the late 1980s, insulin resistance was a well-established and measurable phenomenon — but it was still thought of mainly as a feature of diabetes. The Stanford endocrinologist Gerald M. Reaven (1928–2018) changed that framing in one of the most influential lectures in the history of the field. Each year the American Diabetes Association invites a senior scientist to deliver the Banting Lecture, named for insulin's co-discoverer. In 1988, Reaven used his Banting Lecture to argue that insulin resistance was far more than a diabetes problem.
His lecture, published as "Role of insulin resistance in human disease" in Diabetes (1988; volume 37, pages 1595–1607), proposed that insulin resistance sat at the center of a cluster of common conditions — high blood pressure, abnormal blood fats (high triglycerides and low HDL cholesterol), and a tendency toward high blood sugar — and that this cluster substantially raised the risk of cardiovascular disease. Reaven gave the cluster the deliberately neutral name "Syndrome X," using X to signal that the unifying thread had only just been identified.
The significance of Reaven's contribution was to recast insulin resistance from a narrow metabolic curiosity into a central driver of the chronic diseases that kill most people in the developed world. His "Syndrome X" is the direct ancestor of what is now called the metabolic syndrome — the same constellation of central obesity, hypertension, dyslipidemia, and dysglycemia, now formalized into diagnostic criteria. It is fair to note that the exact boundaries and clinical utility of the syndrome have been debated ever since; what is not debated is that Reaven's lecture put insulin resistance at the heart of cardiometabolic medicine.
From Syndrome X to the Modern Era
The arc from Himsworth to Reaven gave medicine a coherent picture: a concept (1936), a measurement (1959–1960), a gold-standard quantification (1979), a practical index (1985), and a disease framework (1988). Everything since has been an elaboration and deepening of that foundation. The discovery and cloning of the insulin receptor and the unraveling of the intracellular signaling cascade that carries insulin's message inside the cell turned "the tissues don't respond" into a detailed molecular story involving receptor binding, signaling proteins, and glucose transporters.
Modern research has connected insulin resistance to a remarkable range of conditions well beyond diabetes — including polycystic ovary syndrome, non-alcoholic (now metabolic-associated) fatty liver disease, and cardiovascular risk — and has explored how excess fat tissue, inflammation, and lifestyle factors drive it. Tools have multiplied too, from continuous glucose monitoring to refined surrogate indices, even as the clamp and HOMA-IR remain the reference points. Importantly, the field has also shown that insulin resistance is often modifiable: weight loss, exercise, dietary change, and medications can meaningfully improve insulin sensitivity, which is why so much of today's practical advice traces back to understanding this single phenomenon.
What stands out across the whole history is the discipline of distinguishing idea from proof. The early thinkers hypothesized resistance; Himsworth demonstrated it clinically; Yalow and Berson proved it chemically; DeFronzo measured it precisely; Matthews made it practical; and Reaven gave it consequence. Each step rested on the one before, and none claimed more than the evidence allowed. That is exactly how a vague clinical hunch became one of the central organizing ideas of modern metabolic medicine. The clinical picture, causes, and management that grew out of this history are covered on the main Insulin Resistance page and its deep-dive articles.
Research Papers and References
The references below combine landmark primary papers — given with real DOIs or PMIDs where firmly identified — with curated PubMed topic-search links into the historical and review literature. Where a precise citation could not be confidently matched to a stable identifier, a PubMed search link is provided instead, so that no DOI or PMID here is fabricated. Each external link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Himsworth HP. Diabetes mellitus: its differentiation into insulin-sensitive and insulin-insensitive types. The Lancet. 1936;227(5864):127-130. (Reprinted; see PubMed) — PubMed: PMID 24415598
- Krentz AJ, et al. Sir Harold Himsworth and insulin insensitivity 75 years on. Diabetic Medicine. 2011. — doi:10.1111/j.1464-5491.2011.03488.x
- Reaven GM. Banting Lecture 1988: Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595-1607. — doi:10.2337/diab.37.12.1595
- DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. American Journal of Physiology. 1979;237(3):E214-E223. — doi:10.1152/ajpendo.1979.237.3.E214
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412-419. — doi:10.1007/BF00280883
- Yalow RS, Berson SA. Immunoassay of endogenous plasma insulin in man. Journal of Clinical Investigation. 1960;39(7):1157-1175. — doi:10.1172/JCI104130
- The Nobel Prize in Physiology or Medicine 1977 — Rosalyn Yalow (radioimmunoassay) — NobelPrize.org: 1977 facts
- Reaven GM (subject). Why Syndrome X? From Harold Himsworth to the insulin resistance syndrome. Cell Metabolism. 2004. — PubMed: PMID 16054040
- Wilhelm Falta and the early concept of insulin insensitivity (history) — PubMed: Falta and the history of insulin resistance
- History of insulin resistance: concept, discovery, and evolution — PubMed: insulin resistance history and concept
- Radioimmunoassay of insulin and the discovery of hyperinsulinemia in type 2 diabetes — PubMed: radioimmunoassay of insulin (Yalow & Berson)
- Euglycemic clamp as the gold standard for insulin sensitivity — PubMed: euglycemic clamp and insulin sensitivity
- HOMA-IR: derivation, use, and limitations — PubMed: HOMA-IR and the homeostasis model
- From Syndrome X to metabolic syndrome and cardiometabolic risk — PubMed: Syndrome X to metabolic syndrome
External Authoritative Resources
- NIDDK (NIH) — Insulin Resistance and Prediabetes
- NobelPrize.org — 1977 Physiology or Medicine (radioimmunoassay)
- PubMed — All research on the history of insulin resistance
Connections
- Endocrinology
- Blood Sugar & Insulin — interactive animation
- Insulin Resistance (main page)
- Fasting Insulin and HOMA-IR Testing
- Diabetes
- Metabolic Syndrome
- PCOS (Polycystic Ovary Syndrome)
- Obesity
- Insulin Resistance — the modern diet, exercise, and supplement strategies for reversing the condition this history traces.
- All Conditions