Hashimoto's Thyroiditis: History and Discovery
The story of Hashimoto's thyroiditis is really two stories. The first is the careful work of a young Japanese surgeon, Hakaru Hashimoto, who in 1912 looked down a microscope at four diseased thyroid glands and described a pattern no one had named before — a goitre quietly invaded by lymphocytes, which he called struma lymphomatosa. His paper, written in German and buried in a surgical journal, was largely ignored for more than forty years. The second story begins in 1956, when researchers in Buffalo and London proved that this very disease was caused by the body attacking its own thyroid — making it one of the first human illnesses ever shown to be autoimmune, and overturning a dogma that had ruled immunology for half a century. This page traces both: how the disease was first seen, who named it, who found its cause, and why that discovery mattered far beyond the thyroid.
Interactive Visualization How Your Thyroid Is Controlled — run the feedback loop Watch TSH drive the thyroid, T4 convert to T3, and the loop feed back — then switch on Hashimoto's, Graves', or iodine deficiency. Launch →Table of Contents
- The Thyroid and Goitre Before 1912
- Hakaru Hashimoto and "Struma Lymphomatosa" (1912)
- Decades of Obscurity
- 1956 — The Birth of Autoimmune Thyroiditis
- Why It Matters for Autoimmunity as a Whole
- How Diagnosis Evolved: Antibodies and TSH
- Treatment History: From Thyroid Extract to Levothyroxine
- Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
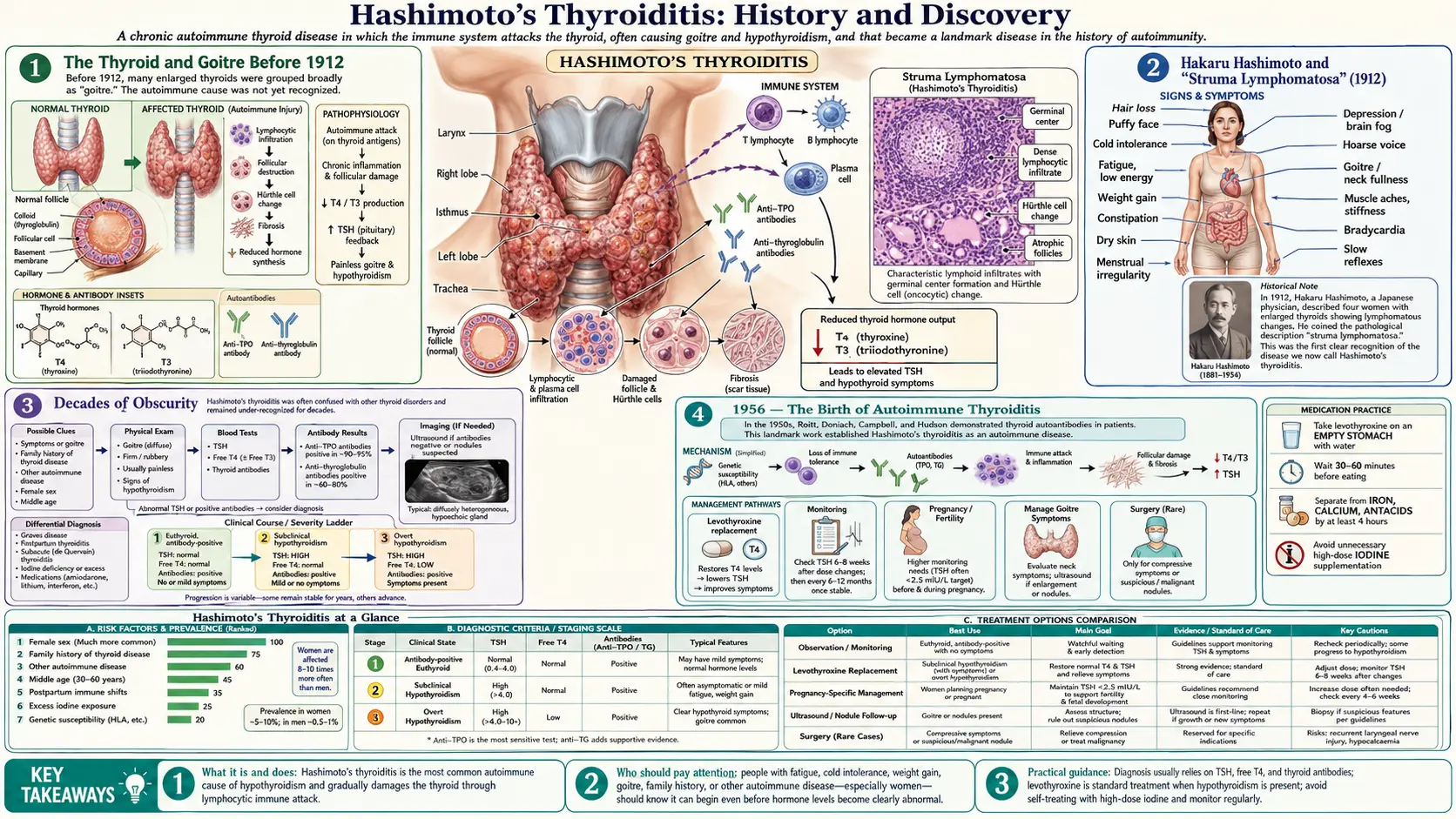
The Thyroid and Goitre Before 1912
For most of medical history, the thyroid gland was a mystery and a swollen one was simply called a goitre. Enlarged neck swellings had been recorded since antiquity and treated, often effectively if accidentally, with sea sponge and seaweed — we now know these are rich in iodine, the element the thyroid needs to make its hormones. But the gland's purpose stayed obscure until the nineteenth century. In 1835 the Irish physician Robert James Graves described the cluster of racing heart, bulging eyes, and goitre that became Graves' disease; in 1850s and 1870s reports, the English surgeon William Withey Gull and others described the opposite state — the puffy, slow, cold, mentally dulled condition of myxoedema, which the surgeon William Ord formally named in 1877.
The crucial leap came from surgery. In the 1880s the Swiss surgeon Theodor Kocher, perfecting the removal of goitres, noticed that patients whose entire thyroid he had removed sank afterwards into exactly the myxoedematous state Gull had described — what Kocher called cachexia strumipriva. Removing the gland produced the disease; the thyroid, therefore, must do something essential. Kocher's work (which earned him the 1909 Nobel Prize) and the demonstration that feeding or injecting thyroid tissue could reverse myxoedema established, by the 1890s, that the thyroid was a vital secreting organ. This was the intellectual world Hashimoto entered: clinicians could now recognize an over-active and an under-active thyroid, but the many kinds of goitre were still being sorted out by their appearance under the microscope.
By 1912, pathologists distinguished several thyroid diseases — simple colloid goitre, Graves' (Basedow's) goitre, and the fibrous, rock-hard gland of Riedel's thyroiditis described in 1896. What no one had cleanly separated out was a distinct, chronic goitre defined by a dense infiltration of lymphocytes and the formation of lymphoid follicles within the gland itself. That gap is precisely what Hashimoto's microscope would fill.
Hakaru Hashimoto and "Struma Lymphomatosa" (1912)
Hakaru Hashimoto (1881–1934) was a Japanese surgeon, not the endocrinologist later generations often imagine. He graduated from the medical school of Kyushu Imperial University in Fukuoka in 1907 and trained in its First Department of Surgery under Professor Hayari Miyake, regarded as Japan's first neurosurgeon. Working through the surgical specimens passing through that department, Hashimoto became interested in a small group of removed goitres whose microscopic appearance did not match any established category.
In 1912 he published his findings as "Zur Kenntnis der lymphomatösen Veränderung der Schilddrüse (Struma lymphomatosa)" — "On the knowledge of lymphomatous change of the thyroid gland (lymphomatous goitre)." It appeared not in Japanese but in German, in the surgical journal Archiv für klinische Chirurgie (Langenbeck's Archiv), volume 97, pages 219–248. Like most ambitious Japanese physicians of the Meiji era, Hashimoto looked to German medicine as the international standard, and publishing in German was the way to reach the world. The paper was based on the detailed examination of thyroid glands from just four middle-aged women.
What Hashimoto described, and illustrated, were four features that together defined a new entity: (1) dense infiltration of the thyroid by lymphocytes; (2) the formation of lymphoid follicles with germinal centres inside the gland; (3) destruction and shrinkage of the normal thyroid follicle cells, many transformed into the large pink-staining cells now called Hürthle or oncocytic cells; and (4) fibrosis, a scarring of the gland's connective tissue. He named the condition struma lymphomatosa — "lymphomatous goitre" — carefully choosing a descriptive term, because the lymphoid tissue made the gland resemble a lymphoma even though it was not a cancer. It was an exact, honest piece of descriptive pathology, and the four criteria he set down remain the histological signature of the disease to this day.
Hashimoto's own career then turned away from the thyroid. In 1912 he traveled to Germany to study pathology at the University of Göttingen under Eduard Kaufmann; the approach of the First World War forced his return to Japan. He eventually settled in his home town of Igamachi (Mie Prefecture) as a respected local surgeon and physician, and died of typhoid fever on 9 January 1934 — more than two decades before the disease bearing his name would be understood, and long before that name became famous.
Decades of Obscurity
For a paper now cited as a landmark, Hashimoto's 1912 report had a strikingly quiet first few decades. Several forces buried it. It was a single, short monograph by a young provincial surgeon, describing only four cases. Some prominent contemporaries doubted that he had found anything new, suspecting his struma lymphomatosa was merely a variant of Riedel's fibrous goitre or a stage of ordinary goitre rather than a disease in its own right. And the outbreak of the First World War disrupted the flow of German-language medical literature that might otherwise have carried his work outward.
Slowly, however, surgeons and pathologists elsewhere began to encounter the same picture and to confirm that it was indeed distinct. Through the 1920s and 1930s the condition was reported under a scatter of names — struma lymphomatosa, lymphadenoid goitre, chronic lymphocytic thyroiditis — and was gradually accepted as a real and recognizable form of thyroid disease, especially after surgeons noticed how often it underlay the firm goitres they removed from middle-aged women. A frequently noted turning point was a 1931 report by the American surgeons Cecil Joll and colleagues, and later writers credited Joll with helping to attach Hashimoto's name to the condition, so that "Hashimoto's disease" and "Hashimoto's struma" came into Anglophone use.
So by the 1940s the disease had a describer (Hashimoto), an eponym (his name), and a place in the textbooks — but still no explanation. No one knew why a thyroid gland should fill up with lymphocytes and slowly destroy itself. The prevailing assumptions ran toward infection or some degenerative process. The true answer would require not a new look at the thyroid, but a revolution in how scientists thought the immune system worked.
1956 — The Birth of Autoimmune Thyroiditis
To grasp why 1956 was a watershed, you have to know the dogma it broke. In the early twentieth century the great immunologist Paul Ehrlich had argued for horror autotoxicus — the principle that the body has a built-in, almost sacred reluctance to make antibodies against its own tissues, because to do so would be suicidal. For half a century this hardened into a near-law: the immune system did not, perhaps could not, attack "self." That belief is exactly why no one had seriously proposed that Hashimoto's lymphocyte-filled thyroid might be a case of the body assaulting its own gland.
In 1956, two independent lines of work shattered the dogma, both pointing at the thyroid. In Buffalo, New York, the immunologists Ernest Witebsky and Noel Rose immunized rabbits with extract of thyroid tissue (rabbits' own or other rabbits') mixed with a powerful immune stimulant, Freund's complete adjuvant. The animals developed antibodies against thyroglobulin (the thyroid's main protein) — and, decisively, their own thyroid glands became infiltrated with lymphocytes, producing a picture that looked strikingly like the human disease Hashimoto had drawn. They had created experimental autoimmune thyroiditis: deliberate, reproducible self-directed immune damage in a living animal.
That same year, in London, Ivan Roitt and Deborah Doniach, working with colleagues, examined the blood of actual patients with Hashimoto's disease. In a paper published in The Lancet on 20 October 1956 — "Auto-antibodies in Hashimoto's disease (lymphadenoid goitre)" — they showed that these patients' serum contained autoantibodies against thyroglobulin. The two findings locked together perfectly: the rabbit experiment proved self-attack on the thyroid was possible and could cause the lesion, and the patient study proved it was actually happening in people with Hashimoto's. Together, Rose and Witebsky in the laboratory and Roitt and Doniach at the bedside established that Hashimoto's thyroiditis is an autoimmune disease — the body's immune system mistaking its own thyroid for a threat.
This is why the year matters so much. Hashimoto had described what the disease looked like in 1912; 1956 finally explained why it happened — and in doing so dethroned horror autotoxicus and made Hashimoto's thyroiditis the founding model of human autoimmunity.
Why It Matters for Autoimmunity as a Whole
The 1956 discovery reached far beyond the neck. Before it, "autoimmune disease" was barely a usable idea; afterward, it became one of the central organizing concepts of modern medicine. Hashimoto's thyroiditis was among the very first human conditions to be proven autoimmune, and because the thyroid is an accessible organ that makes a single, easily studied main protein, it became the laboratory model in which the rules of organ-specific autoimmunity were first worked out. Conditions from type 1 diabetes and pernicious anaemia to rheumatoid arthritis and lupus were subsequently re-understood through the lens that thyroiditis helped create.
The work also forced immunology to confront a hard question Ehrlich's dogma had let it dodge: if the body can attack itself, what normally stops it? Witebsky, mindful of the burden of proof, even helped frame a set of criteria (echoing Koch's postulates for infection) for deciding when a disease may legitimately be called autoimmune — demonstrate the autoantibody or self-reactive cells, identify the target antigen, and reproduce the disease in an animal by immunizing against that antigen. Hashimoto's thyroiditis satisfied all of them, and so became the template against which other candidate autoimmune diseases were judged. The modern fields of self-tolerance, regulatory T cells, and autoimmunity all trace part of their lineage to that 1956 moment at the thyroid.
There is a human dimension here too. Recognizing Hashimoto's as autoimmune reframed it from a baffling local oddity of the gland into one instance of a body-wide tendency — which is why people with Hashimoto's are now known to carry a higher risk of other autoimmune conditions, and why the disease is studied as a window onto immune tolerance generally.
How Diagnosis Evolved: Antibodies and TSH
Before the 1950s, Hashimoto's could be diagnosed with certainty only by surgery — a pathologist confirming the lymphocytic infiltrate in a gland that had been removed or biopsied. The 1956 discovery of thyroglobulin autoantibodies changed that overnight: for the first time, a simple blood test could point to the disease in a living, intact patient. Early laboratories detected anti-thyroglobulin antibodies (anti-Tg, the original Roitt–Doniach finding) and a second target soon called the thyroid microsomal antigen, against which most patients also had antibodies.
The "microsomal" antibody turned out to be even more important once its true target was identified. In the 1980s, researchers (notably Czarnocka and colleagues in 1985) showed that the mysterious thyroid microsomal antigen was in fact the enzyme thyroid peroxidase (TPO) — the very enzyme the gland uses to build thyroid hormone. What had been called the anti-microsomal antibody was renamed the anti-thyroid-peroxidase (anti-TPO) antibody, and it became the single most useful blood marker of Hashimoto's: today the great majority of people with the disease test positive for anti-TPO, often alongside anti-thyroglobulin antibodies. The deeper meaning and interpretation of these markers is covered in the companion TPO and TgAb Antibodies Explained article.
The other half of modern diagnosis is the measurement of thyroid function, and here the key tool is thyroid-stimulating hormone (TSH). The pituitary gland raises TSH when the thyroid is failing, so a high TSH is an early, sensitive signal of an underactive gland — the usual fate of a thyroid steadily destroyed by Hashimoto's. Reliable TSH radioimmunoassays arrived in the 1960s and 1970s and were refined into the ultrasensitive assays used now, allowing clinicians to catch hypothyroidism long before a patient feels its full weight. The combination is what defines the disease today: positive thyroid antibodies (anti-TPO and/or anti-Tg) plus a rising TSH, often supported by ultrasound showing the characteristic patchy, hypoechoic gland. Optimal ranges for these tests are discussed in TSH, T4 and T3 Optimal Ranges.
Treatment History: From Thyroid Extract to Levothyroxine
The treatment of Hashimoto's is, at its core, the treatment of the underactive thyroid it causes — and that history begins, remarkably, just before Hashimoto's own paper. In 1891 the English physician George Redmayne Murray treated a woman dying of myxoedema with an injected extract of sheep thyroid, and watched her recover. It was one of the first triumphs of what we would now call hormone replacement: a missing glandular secretion supplied from outside. Murray's patient went on to live for decades on the treatment, and the principle — give the body the thyroid substance it can no longer make — has never changed.
Murray's injections quickly gave way to the simpler practice of feeding dried, powdered animal thyroid by mouth. Desiccated thyroid extract, prepared from pig or cattle glands, became the standard treatment for hypothyroidism for the first half of the twentieth century. It worked, and cheaply, but it had a real drawback: each batch's hormone content varied, so dosing was imprecise. Patients with Hashimoto's-driven hypothyroidism in the 1920s through the 1950s were treated, by and large, with this natural extract.
The path to a standardized drug ran through chemistry. In 1914 Edward Kendall at the Mayo Clinic isolated the pure thyroid hormone he named thyroxine from animal glands; in 1927 the British chemists Charles Robert Harington and George Barger worked out its structure and synthesized it in the laboratory. That achievement made it possible, in time, to manufacture the pure hormone in precise, identical doses rather than relying on ground-up glands. The synthetic form — levothyroxine (synthetic T4) — came into wide clinical use from the mid-twentieth century and, because the body converts T4 into the more active T3 as needed, it became the dominant treatment: a single daily tablet, consistent in strength, that restores thyroid hormone to normal. It remains the standard of care for the hypothyroidism of Hashimoto's today, though some patients and clinicians still discuss desiccated extract and added T3, a debate explored in Levothyroxine vs NDT vs T3. It is worth stressing what treatment does and does not do: replacing the hormone corrects the deficiency superbly, but it does not switch off the underlying autoimmune process — which is why interest in the nutritional and immune dimensions of the disease, such as selenium and other micronutrients, continues.
Modern Understanding
A century after Hashimoto, the disease he sketched in four cases is understood as the most common cause of an underactive thyroid in iodine-sufficient parts of the world, and one of the most common autoimmune diseases of all. We now know it is driven by a self-directed immune attack — T lymphocytes infiltrating and gradually destroying the thyroid, with anti-TPO and anti-thyroglobulin antibodies as the hallmark of the process — arising in genetically susceptible people, far more often women than men, under the influence of triggers that are still being mapped (among them iodine excess, certain infections, smoking, pregnancy, and selenium status). The end result is the slow loss of hormone-producing tissue and, in most patients, hypothyroidism.
The arc of this history is unusually clean. Hashimoto supplied the picture in 1912; Rose, Witebsky, Roitt and Doniach supplied the cause in 1956; the antibody tests and TSH assays of the following decades supplied the diagnosis; and replacement therapy, from Murray's 1891 extract to modern levothyroxine, supplied the treatment. Each step built on the last. Research now reaches past these foundations toward the genetics and immunology of why tolerance to the thyroid breaks down, in the hope of one day modifying the autoimmune process itself rather than only replacing its lost product.
It is fitting that the disease still carries the name of the surgeon who first saw it clearly. Hashimoto never knew his struma lymphomatosa would become a cornerstone of immunology, nor that his name would be spoken in clinics worldwide every day. His 1912 paper is a quiet reminder that careful, honest observation — even of only four patients, even when ignored for forty years — can open a door that an entire field eventually walks through. For the present-day clinical picture, diagnosis, and management, see the main Hashimoto's Thyroiditis page.
Research Papers and References
The references below combine the landmark historical papers in the discovery of Hashimoto's thyroiditis and human autoimmunity with curated PubMed topic-search links and authoritative reviews. Hashimoto's original 1912 monograph (Zur Kenntnis der lymphomatösen Veränderung der Schilddrüse [Struma lymphomatosa], Archiv für klinische Chirurgie, 1912;97:219–248) is named in the article as a historical primary source. Each link opens in a new tab.
- Roitt IM, Doniach D, Campbell PN, Hudson RV. Auto-antibodies in Hashimoto's disease (lymphadenoid goitre). The Lancet. 1956;268(6947):820–821. (20 October 1956) — PubMed: Auto-antibodies in Hashimoto's disease
- Witebsky E, Rose NR, Terplan K, Paine JR, Egan RW. Chronic thyroiditis and autoimmunization. JAMA. 1957;164(13):1439–1447. — PubMed: Witebsky & Rose, chronic thyroiditis and autoimmunization
- Rose NR, Witebsky E. Studies on organ specificity. V. Changes in the thyroid glands of rabbits following active immunization with rabbit thyroid extracts. Journal of Immunology. 1956;76(6):417–427. — PubMed: Rose & Witebsky, experimental autoimmune thyroiditis in rabbits
- Pearce EN, Farwell AP, Braverman LE. Thyroiditis. New England Journal of Medicine. 2003;348(26):2646–2655. — doi:10.1056/NEJMra021194
- Caturegli P, De Remigis A, Rose NR. Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmunity Reviews. 2014;13(4–5):391–397. — doi:10.1016/j.autrev.2014.01.007
- Ralli M, Angeletti D, Fiore M, et al. Hashimoto's thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmunity Reviews. 2020;19(10):102649. — doi:10.1016/j.autrev.2020.102649
- Weetman AP. The immunopathogenesis of chronic autoimmune thyroiditis one century after Hashimoto. European Thyroid Journal. 2013;1(4):243–250. — doi:10.1159/000343834
- Czarnocka B, Ruf J, Ferrand M, Carayon P, Lissitzky S. Purification of the human thyroid peroxidase and its identification as the microsomal antigen involved in autoimmune thyroid diseases. FEBS Letters. 1985;190(1):147–152. — PubMed: thyroid peroxidase identified as the microsomal antigen (1985)
- Sawin CT. The heritage of Dr. Hakaru Hashimoto (1881–1934). Endocrine Journal. 2002;49(4):399–403. — PubMed: the heritage of Dr. Hakaru Hashimoto
- Hiromatsu Y, Satoh H, Amino N. Hashimoto's thyroiditis: history and future outlook. Hormones (Athens). 2013;12(1):12–18. — PubMed: Hashimoto's thyroiditis — history and future outlook
- Murray GR. Note on the treatment of myxoedema by hypodermic injections of an extract of the thyroid gland of a sheep. British Medical Journal. 1891;2(1606):796–797. — PubMed: Murray, treatment of myxoedema by thyroid extract (1891)
- Harington CR, Barger G. Chemistry of thyroxine. III. Constitution and synthesis of thyroxine. Biochemical Journal. 1927;21(1):169–183. — PubMed: Harington & Barger, synthesis of thyroxine (1927)
- History and concept of autoimmunity — horror autotoxicus and the 1956 origins of human autoimmune disease — PubMed: history of autoimmunity and horror autotoxicus
- All research on Hashimoto's (chronic lymphocytic / autoimmune) thyroiditis — PubMed: Hashimoto's thyroiditis
External Authoritative Resources
- NIDDK (National Institutes of Health) — Hashimoto's Disease
- American Thyroid Association — Hashimoto's Thyroiditis
- PubMed — All research on Hashimoto's thyroiditis
Connections
- Endocrinology
- How Your Thyroid Is Controlled — interactive animation
- Hashimoto's Thyroiditis (Main Page)
- TPO and TgAb Antibodies Explained
- Levothyroxine vs NDT vs T3
- Graves' Disease
- Thyroid Disorders
- Selenium
- All Conditions