Stevens-Johnson Syndrome
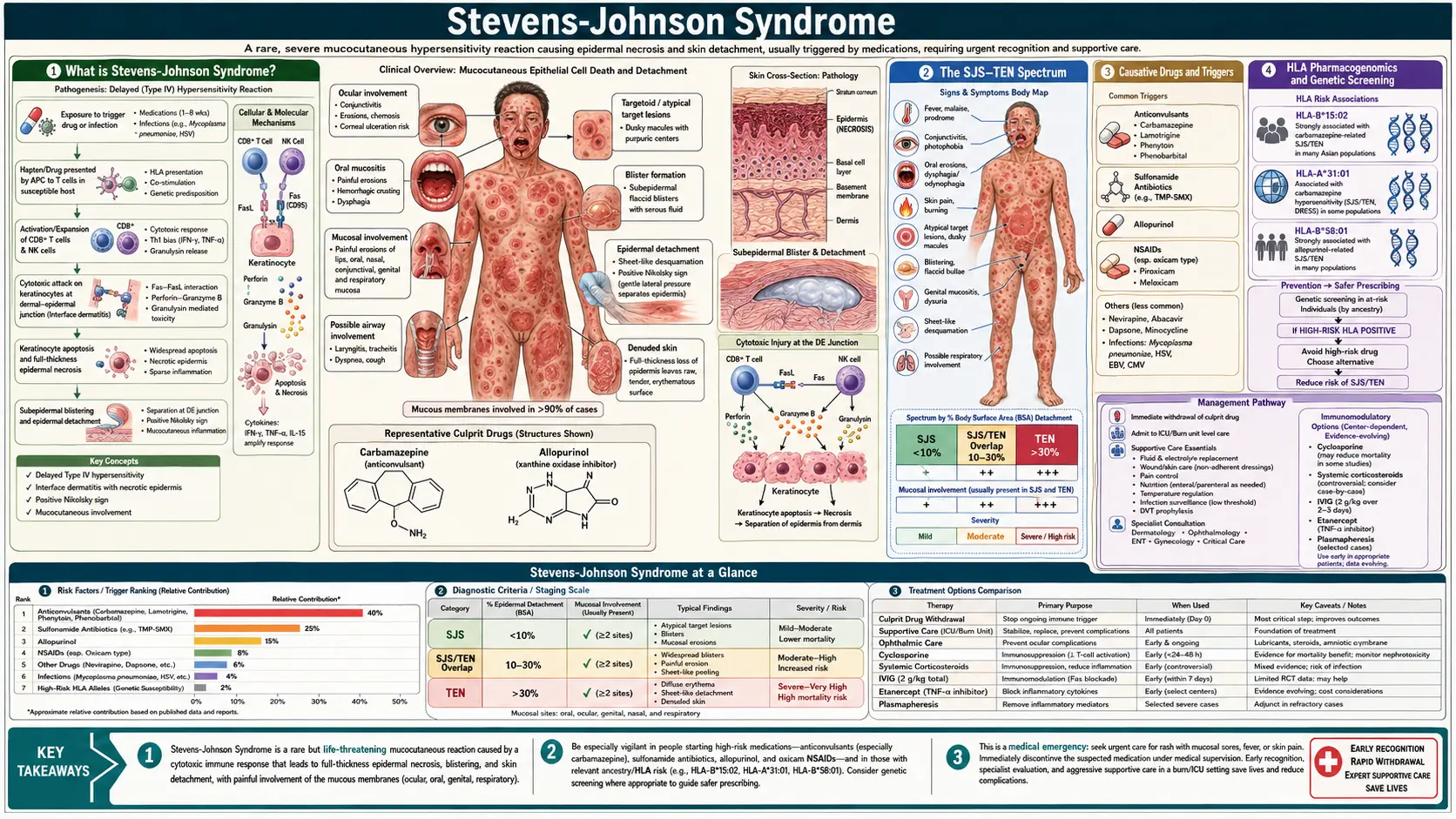
Table of Contents
- What is Stevens-Johnson Syndrome?
- The SJS–TEN Spectrum
- Causative Drugs and Triggers
- HLA Pharmacogenomics and Genetic Screening
- Pathophysiology: Granulysin and Keratinocyte Apoptosis
- Clinical Features and Prodrome
- Diagnosis: Nikolsky Sign and Skin Biopsy
- SCORTEN Prognostic Score
- Treatment: Supportive Care and Immunomodulation
- Ophthalmological Emergency
- Research Papers
- Connections
- Featured Videos
What is Stevens-Johnson Syndrome?
Stevens-Johnson Syndrome (SJS) is a rare but potentially fatal mucocutaneous hypersensitivity reaction characterized by widespread keratinocyte death, skin detachment, and severe erosions of multiple mucous membranes. It was first described by Albert Mason Stevens and Frank Chambliss Johnson in 1922 in two children with fever, stomatitis, and conjunctivitis — a clinical picture now recognized as the mucocutaneous inflammatory syndrome we understand today.
SJS belongs to a continuum of escalating severity: SJS (epidermal detachment less than 10% of body surface area), SJS/TEN overlap (10–30% detachment), and toxic epidermal necrolysis (TEN or Lyell syndrome) (greater than 30% detachment). The distinction is prognostic, not mechanistic — all represent the same immune-mediated keratinocyte destruction driven by cytotoxic lymphocytes and natural killer cells. TEN, at its most severe, resembles a full-thickness burn covering the majority of the body surface.
Incidence is low — approximately 1–6 cases per million people per year for SJS, 0.4–1.2 per million for TEN — but mortality is high: roughly 5–10% for SJS and 25–35% for TEN, reaching over 90% in patients with the highest SCORTEN prognostic scores. Drug reactions account for approximately 70–80% of adult SJS/TEN cases; infection (primarily Mycoplasma pneumoniae) accounts for most pediatric SJS cases.
The SJS–TEN Spectrum
The International Consensus Classification (Bastuji-Garin, 1993) defines the spectrum by the percentage of total body surface area (BSA) showing epidermal detachment — meaning frank denuded skin or skin that detaches with lateral pressure:
- SJS: Detachment of less than 10% BSA. Widespread dusky erythematous or purpuric macules, typically with atypical target lesions and prominent mucous membrane erosions. Mortality approximately 5–10%.
- SJS/TEN overlap: Detachment 10–30% BSA. Intermediate severity; prognosis between the two poles.
- TEN (Lyell syndrome): Detachment greater than 30% BSA. Large sheets of epidermis slough off, leaving raw, bleeding dermis resembling a severe burn. Without specialized burn-unit care, death from sepsis, fluid loss, and multi-organ failure is likely. Mortality approximately 25–35%, rising sharply with the SCORTEN score.
An important pediatric subset is SJS due to Mycoplasma pneumoniae (MP-SJS or MIRM — Mycoplasma-Induced Rash and Mucositis). Children with this form have prominent mucous membrane erosions (oral, ocular, urogenital) with minimal or absent skin detachment. Some experts propose separating MIRM from drug-induced SJS given the more benign course and different trigger.
Erythema multiforme (EM) is a related but distinct entity — typically self-limited, recurrent, predominantly caused by herpes simplex virus, with classic "true" target lesions (three zones: central dusky or necrotic core, pale edematous ring, erythematous periphery) and less severe mucous membrane involvement than SJS. The old term "EM major" for severe EM with mucosal involvement has been largely abandoned in favor of the SJS classification to avoid confusion.
Causative Drugs and Triggers
Drug reactions are the predominant cause of SJS and TEN in adults. The interval from first drug exposure to SJS onset is typically 1–3 weeks (the time needed for sensitization and immune expansion). On rechallenge or with an already-sensitized patient, onset may occur within 3–10 days. Recognizing the responsible drug and stopping it immediately is the single most important therapeutic intervention.
High-Risk Drug Classes
- Allopurinol: The most common cause of SJS/TEN in Asia and increasingly in Western countries. Risk is highest in the first 2 months of use. Strong HLA-B*58:01 association (see below).
- Sulfonamide antibiotics: Sulfamethoxazole (in co-trimoxazole/TMP-SMX), sulfadiazine, sulfasalazine. Among the originally identified SJS triggers and remain high-risk.
- Aromatic anticonvulsants: Carbamazepine (highest risk, especially with HLA-B*15:02 in Han Chinese and Southeast Asian populations), lamotrigine, phenytoin, phenobarbital. Carbamazepine-induced SJS risk rises dramatically if HLA-B*15:02 is present — approximately 25-fold increase in risk.
- Oxicam NSAIDs: Piroxicam, meloxicam. Implicated in disproportionate SJS/TEN cases relative to their use prevalence.
- Nevirapine: Non-nucleoside reverse transcriptase inhibitor (antiretroviral). High rates of SJS especially in women and patients with higher CD4 counts at initiation.
- Other anticonvulsants: Oxcarbazepine, zonisamide, levetiracetam (lower risk than aromatic anticonvulsants).
- Other antibiotics: Aminopenicillins (ampicillin, amoxicillin), cephalosporins, fluoroquinolones, tetracyclines.
Infectious Triggers
Mycoplasma pneumoniae is the dominant infectious trigger, predominantly in children and young adults. SJS following Mycoplasma tends to have less skin detachment with more severe mucosal involvement. Herpes simplex virus (HSV) triggers erythema multiforme more commonly than SJS. Histoplasma, cytomegalovirus (CMV), and HIV infection have also been associated with SJS/TEN.
HLA Pharmacogenomics and Genetic Screening
One of the most striking advances in understanding SJS/TEN has been the discovery of specific HLA (human leukocyte antigen) alleles that confer extremely high risk for drug-specific reactions. These associations reflect the fact that the drug or its reactive metabolite must be presented by a specific MHC molecule to activate cytotoxic T cells.
Key HLA–Drug Associations
- HLA-B*15:02 — Carbamazepine (Han Chinese, Thai, Vietnamese, Filipino, South Asian populations): Odds ratio for SJS/TEN approximately 80–1000× in Han Chinese carriers. The US FDA issued a Black Box Warning and mandates HLA-B*15:02 screening before initiating carbamazepine in patients with ancestry from at-risk populations. The allele frequency is approximately 8% in Han Chinese and 6–8% in Thai populations, but less than 1% in Europeans. Oxcarbazepine carries partial cross-reactivity.
- HLA-B*57:01 — Abacavir: This HIV antiretroviral causes a severe hypersensitivity reaction (including skin manifestations) almost exclusively in HLA-B*57:01 carriers. Prospective screening and exclusion of HLA-B*57:01-positive patients has essentially eliminated abacavir hypersensitivity reactions. This was the first pharmacogenomic screening to be routinely implemented in clinical practice and represents a proof-of-concept for the field.
- HLA-B*58:01 — Allopurinol: Strongly associated with allopurinol-induced SJS/TEN in Han Chinese, Thai, Korean, and other Asian populations. Allele frequency approximately 6–8% in these populations versus 0.1% in Europeans. Some guidelines recommend screening in at-risk Asian populations before allopurinol initiation.
- HLA-A*31:01 — Carbamazepine (European and Japanese populations): Associated with multiple carbamazepine hypersensitivity syndromes (SJS, DRESS, maculopapular exanthema) in Europeans and Japanese — a population with low HLA-B*15:02 prevalence. Some European guidelines recommend this screen before carbamazepine initiation.
The mechanistic basis is direct: the drug (or a reactive metabolite) binds non-covalently to the peptide-binding groove of the specific HLA molecule, forming a pharmacological interaction (the "p-i concept") that mimics antigen presentation and activates cytotoxic T cells bearing specific T-cell receptors. This is distinct from classical drug haptenation.
Pathophysiology: Granulysin and Keratinocyte Apoptosis
The cellular mechanism of keratinocyte death in SJS/TEN has been substantially elucidated over the past two decades. Activated drug-specific cytotoxic CD8+ T lymphocytes (CTLs) and natural killer (NK) cells accumulate in the skin in response to the drug-HLA interaction. These effector cells kill keratinocytes through multiple pathways:
Granulysin — The Key Mediator
The landmark 2008 study by Chung and colleagues identified granulysin as the dominant soluble cytotoxin responsible for widespread keratinocyte death in SJS/TEN. Granulysin is a cationic cytolytic protein stored in secretory lysosomes of CTLs and NK cells. It is released upon target cell recognition and penetrates the keratinocyte membrane, triggering caspase-independent apoptosis via mitochondrial pathway disruption. Critically, granulysin was found in blister fluid at concentrations 4–10 times higher than perforin or granzyme B, and its concentration correlates directly with disease severity. In mouse models, injection of recombinant granulysin alone reproduced the skin detachment of SJS/TEN.
Additional Apoptotic Pathways
- Fas–FasL pathway: Keratinocytes in SJS/TEN upregulate Fas (CD95); blister-fluid lymphocytes express FasL. Fas–FasL interaction triggers keratinocyte apoptosis. This pathway was initially thought to be primary but is now understood as contributory alongside granulysin.
- Perforin and granzyme B: CTLs release perforin pores in the keratinocyte membrane through which granzyme B (a serine protease) enters and cleaves caspases, triggering apoptosis.
- TNF-α: Elevated in blister fluid; activates NF-κB and JNK pathways leading to keratinocyte apoptosis and dermal inflammation.
- Annexin A1: Recently identified as the key ligand on keratinocytes that triggers CTL and NK cell recognition via the FPR1 receptor, initiating targeted cytotoxic attack.
The end result — massive synchronous keratinocyte apoptosis across large areas of skin — is histologically visible as full-thickness epidermal necrosis with a clean dermal-epidermal separation, seen on skin biopsy as necrotic epidermis separating above an otherwise relatively normal dermis (in contrast to burns, where the dermis is also damaged).
Clinical Features and Prodrome
Prodromal Phase (Days 1–3)
SJS/TEN characteristically begins with a nonspecific flu-like prodrome that may be mistaken for a viral illness or drug side effect: fever (often greater than 39°C), malaise, sore throat, photophobia, burning eyes, and skin tenderness or dysesthesia. This prodrome precedes the skin eruption by 1–3 days. The early mucosal burning and photophobia are important warning signs — mucous membrane involvement in SJS/TEN nearly always precedes or accompanies the rash, unlike most other drug eruptions.
Cutaneous Eruption
The rash typically begins on the trunk and face, then spreads to involve the extremities. Initial lesions are dusky erythematous macules or atypical target lesions — flat, lacking the raised edematous ring of true erythema multiforme targets. These macules coalesce rapidly, and the centers of the lesions become purpuric or necrotic. Within 1–3 days, the epidermis begins to detach, starting with blister formation within the macules. The skin may feel painful and tender before visible blistering — patients often describe it as a "burning" or "raw" sensation under the skin. The Nikolsky sign is positive: lateral pressure on erythematous skin causes the epidermis to shear and separate laterally.
Mucous Membrane Involvement — Mandatory for SJS Diagnosis
Mucous membrane erosions are a defining feature of SJS and must be present. Involvement includes:
- Oral mucosa: Hemorrhagic crusting of the lips (pathognomonic when paired with skin lesions), erosions of the buccal mucosa, tongue, and palate. Severe pain limits eating and drinking — nutritional support is essential.
- Ocular mucosa: Conjunctival hyperemia, chemosis, pseudomembrane formation, eyelid edema. This is the most feared mucosal site — see Ophthalmological Emergency section.
- Urogenital mucosa: Erosions of the glans penis or vaginal mucosa, dysuria, urinary retention. Urethral stricture is a long-term complication.
- Respiratory mucosa: Tracheobronchial involvement with hemorrhagic mucositis in severe TEN can cause respiratory failure.
Diagnosis: Nikolsky Sign and Skin Biopsy
Clinical Assessment
SJS/TEN is primarily a clinical diagnosis. The key diagnostic features are:
- Recent (within 1–3 weeks) drug exposure (or Mycoplasma infection in children)
- Prodromal fever and mucosal burning
- Dusky/purpuric flat macules or atypical targets — not raised urticarial targets
- Mandatory mucous membrane erosions (at least two sites)
- Positive Nikolsky sign in erythematous skin
- Measured or estimated BSA detachment to classify SJS vs. overlap vs. TEN
The RegiSCAR (Registry of Severe Cutaneous Adverse Reactions) group developed validated scoring criteria using the above features to confirm SJS/TEN diagnosis and exclude mimics (e.g., staphylococcal scalded skin syndrome, which also shows Nikolsky positivity but is caused by exfoliatin toxin rather than immune-mediated keratinocyte death, and which spares mucous membranes).
Skin Biopsy
Biopsy of an early lesion (ideally within 24–48 hours) shows full-thickness epidermal necrosis with keratinocyte apoptosis at all levels of the epidermis, a sparse lymphocytic infiltrate at the dermal-epidermal junction, and subepidermal blister formation with little dermal inflammation. The necrotic epidermis rests on an otherwise relatively intact dermis — this contrasts with staphylococcal scalded skin syndrome, where the split is superficial (subcorneal) and epidermal necrosis is absent. Frozen sections of the detached "roof" can rapidly confirm full-thickness vs. superficial split.
Laboratory Evaluation
No blood test is diagnostic of SJS/TEN, but laboratory evaluation guides severity assessment and management:
- Complete blood count (lymphopenia is common; eosinophilia may suggest DRESS rather than SJS/TEN)
- Comprehensive metabolic panel (electrolytes, renal function — fluid losses cause electrolyte disturbances)
- Liver function tests (hepatitis in some drug reactions; drugs eliminated hepatically)
- Blood cultures (fever may reflect secondary sepsis)
- Mycoplasma pneumoniae serology and PCR (especially in children)
SCORTEN Prognostic Score
SCORTEN (SCORe of Toxic Epidermal Necrolysis) is a validated prognostic scoring system developed by Bastuji-Garin and colleagues (2000) to predict in-hospital mortality for SJS/TEN. It is calculated from seven binary variables assessed within the first 24 hours of hospital admission:
- Age >40 years (1 point)
- Presence of malignancy (1 point)
- Heart rate >120 bpm (1 point)
- Initial BSA epidermal detachment >10% (1 point)
- Serum BUN >28 mg/dL (urea >10 mmol/L) (1 point)
- Serum bicarbonate <20 mEq/L (1 point)
- Serum glucose >252 mg/dL (14 mmol/L) (1 point)
SCORTEN score and associated predicted mortality:
- 0–1 points: ~3.2% mortality
- 2 points: ~12.1%
- 3 points: ~35.3%
- 4 points: ~58.3%
- 5+ points: >90% mortality
SCORTEN should be recalculated on days 3 and 5 of admission, as BSA detachment typically peaks during this period and the metabolic variables evolve. It is used to guide triage decisions (transfer to burn unit), inform family communication, and stratify patients in clinical trials.
Treatment: Supportive Care and Immunomodulation
Step 1 — Immediate Drug Withdrawal
The single most impactful intervention is immediate identification and discontinuation of the causative drug. Each day of continued drug exposure is associated with increased BSA detachment and higher mortality. Where multiple drugs are implicated, all non-essential drugs should be stopped; the drug started most recently or most strongly associated with SJS/TEN (using tools like the ALDEN algorithm — Algorithm of Drug Causality in Epidermal Necrolysis) should be prioritized for discontinuation. The half-life of the offending drug also predicts how quickly the reaction will plateau after withdrawal.
Step 2 — Specialized Wound Care (Burn Unit)
Patients with SJS/TEN detachment greater than 10% should be transferred to a burn center or specialized dermatology intensive care unit. Management parallels burn care:
- Fluid resuscitation: Significant fluid, protein, and electrolyte losses through denuded skin — aggressive IV fluid replacement, typically with Ringer's lactate, tailored to urine output.
- Temperature regulation: Environmental temperature set to 30–32°C to minimize the thermogenic cost of evaporative water loss through denuded skin.
- Wound management: Gentle non-adhesive dressings (petrolatum gauze, biologic membranes, or biosynthetic dressings). Do NOT forcibly debride intact necrotic epidermis — it provides a temporary biologic barrier. Early ophthalmology consultation.
- Pain management: Intravenous opioid analgesia for wound care procedures; anxiolytics for dressing changes.
- Nutritional support: Early nasogastric or nasojejunal tube feeding (oral intake is impaired by mucosal erosions).
- Infection surveillance: Surveillance cultures (wounds, blood, urine); systemic antibiotics only for documented infection (prophylactic antibiotics are not recommended and may select resistant organisms).
Immunomodulatory Therapies
Evidence for specific immunosuppressive therapies in SJS/TEN is limited by the rarity of the disease and absence of randomized controlled trials. The most studied options:
- Cyclosporine: Currently the immunomodulatory agent with the best evidence base in SJS/TEN. Mechanistically, cyclosporine inhibits calcineurin → blocks T-cell activation and IL-2 production → suppresses CTL-mediated keratinocyte killing. Multiple retrospective series and a meta-analysis suggest cyclosporine reduces mortality and may halt disease progression. Typical dosing: 3–5 mg/kg/day for 10–14 days with rapid taper. Renal function monitoring is essential. Cyclosporine also decreases TNF-α and Fas-FasL-mediated apoptosis.
- IV immunoglobulin (IVIg): Proposed mechanisms include Fas pathway blockade and granulysin neutralization. Early retrospective reports suggested benefit; however, a systematic review and the prospective SWIFT (SJS World Initiative For Treatment) data did not demonstrate a survival advantage over supportive care alone at standard doses. High-dose IVIg (2–3 g/kg) combined with cyclosporine is used in some centers.
- Etanercept: TNF-α inhibitor (soluble receptor). Several prospective series from Taiwan suggest etanercept 50 mg subcutaneous ×2 doses significantly reduces mortality compared to historical controls (SCORTEN-predicted vs. actual mortality). Phase II randomized controlled trial data are emerging. Etanercept has an excellent safety profile in the short term (no immunosuppression-related infections in short courses).
- Corticosteroids: Controversial and not recommended as primary therapy. Early retrospective data suggested harm (increased infection, delayed wound healing); however, very early (pre-detachment) short-course systemic corticosteroids may abort the reaction in selected cases. Current guidelines do not support routine use.
- Thalidomide: Formally studied and found to be harmful — a randomized trial showed increased mortality in the thalidomide arm. Thalidomide must not be used in SJS/TEN.
Ophthalmological Emergency
Ocular involvement in SJS/TEN is an ophthalmological emergency — the most feared long-term complication is permanent blindness from progressive conjunctival cicatrization (scarring), and the window for intervention to preserve vision is narrow.
Acute Ocular Manifestations
- Conjunctival hyperemia, chemosis (edema), photophobia, purulent discharge
- Pseudomembrane formation on the palpebral conjunctiva (fibrinous membranes that, if not removed, cause severe symblepharon)
- Eyelid margin erosions and trichiasis (lashes turning inward, abrading the cornea)
- Corneal epithelial defects and ulceration — risk of corneal perforation in severe cases
Symblepharon Formation
The most catastrophic acute complication is symblepharon — adhesion of the bulbar conjunctiva (over the eyeball) to the palpebral conjunctiva (lining the eyelids). Symblephara form rapidly as the inflamed conjunctival surfaces make contact and scar. Once established, symblephara restrict eye movement, distort lid anatomy, cause chronic dry eye, and expose the cornea to persistent abrasion. Aggressive early intervention is required to prevent their formation.
Ophthalmological Management
- Daily ophthalmology assessment from day 1 of hospitalization, regardless of symptom severity at presentation (ocular involvement may evolve rapidly)
- Pseudomembrane removal by the ophthalmologist daily or twice daily using a glass rod or moist cotton-tipped applicator — prevents the symblepharon adhesions from forming
- Amniotic membrane transplantation (AMT): Fresh or cryopreserved amniotic membrane can be placed as an ocular surface overlay within the first 72–96 hours in patients with severe conjunctival involvement. AMT provides an anti-inflammatory, anti-fibrotic substrate that dramatically reduces the risk of symblepharon and long-term visual impairment
- Preservative-free lubricating eye drops every 1–2 hours; topical antibiotic drops for corneal defects; topical cyclosporine A for chronic ocular surface disease
- Long-term: Scleral contact lenses for dry eye and irregular astigmatism; surgical management of established symblephara; mucous membrane grafting in severe cases
Even with optimal acute management, approximately 35% of SJS/TEN survivors have significant long-term ocular sequelae, and 3–10% are legally blind. Patients who survived SJS/TEN should be followed by an ophthalmologist long-term, as dry eye disease and conjunctival fibrosis can progress for years after the acute episode.
Research Papers
Key peer-reviewed studies on SJS/TEN pathogenesis, pharmacogenomics, and treatment. Each PMID link opens the study on PubMed.
- Chung WH, et al. Medical genetics: a marker for Stevens-Johnson syndrome. Nature. 2004;428(6982):486. PMID 15057820
- Chung WH, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 2008;14(12):1343-1350. PMID 19029983
- Bastuji-Garin S, et al. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 2000;115(2):149-153. PMID 10951229
- Mockenhaupt M, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study. J Invest Dermatol. 2008;128(1):35-44. PMID 17805350
- Halevy S, et al. Allopurinol is the most common cause of Stevens-Johnson syndrome and toxic epidermal necrolysis in Europe and Israel. J Am Acad Dermatol. 2008;58(1):25-32. PMID 17919772
- Nassif A, et al. Evaluation of T-cell-mediated blister formation in patients with toxic epidermal necrolysis: involvement of FasL and perforin pathways. J Invest Dermatol. 2004;123(5):964-971. — Search PubMed
- Schneck J, et al. Effects of treatments on the mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis: a retrospective study on patients included in the prospective EuroSCAR Study. J Am Acad Dermatol. 2008;58(1):33-40. — Search PubMed
- Kirchhof MG, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71(5):941-947. — Search PubMed
- Chen P, et al. Carbamazepine-induced toxic effects and HLA-B*1502 screening in Taiwan. N Engl J Med. 2011;364(12):1126-1133. PMID 21428768
- Dodiuk-Gad RP, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: an update. Am J Clin Dermatol. 2015;16(6):475-493. PMID 26481651
- Shanbhag SS, et al. Acute ocular manifestations of Stevens-Johnson syndrome and toxic epidermal necrolysis — the foundation for chronic disease. Am J Ophthalmol. 2019;206:172-190. — Search PubMed
- Choo KJL, Leow YH, Bigby M. Allopurinol hypersensitivity syndrome: a systematic review. Br J Dermatol. 2015;173(6):1560. — Search PubMed
Curated PubMed topic searches:
- PubMed: SJS/TEN treatment
- PubMed: HLA-B*15:02 carbamazepine
- PubMed: Granulysin mechanism
- PubMed: SCORTEN prognosis
- PubMed: Cyclosporine SJS
- PubMed: Ocular AMT in SJS
- PubMed: Mycoplasma SJS children
- PubMed: Allopurinol HLA-B*58:01
Connections
- Dermatology
- Bullous Pemphigoid
- Pemphigus Vulgaris
- Lichen Planus
- Psoriasis
- Eczema
- Contact Dermatitis
- Rosacea
- Lupus
- Vitiligo
- Epilepsy
- Gout