Cholesterol Management: History and Discovery
The story of cholesterol runs from a waxy crystal scraped out of a gallstone in 1769 to a class of medicines now taken by tens of millions of people every day. Along the way it gathered a Greek name, two Nobel Prizes for chemistry, a famous rabbit experiment, a sweeping mid-century hypothesis linking diet and the heart, the discovery of the receptor that controls it, and a fungus-derived drug that changed cardiology. This page separates three things that are often blurred together: the discovery of cholesterol the molecule, the lipid (diet–heart) hypothesis that connected it to heart disease, and the drugs built to lower it. Where a claim is a hypothesis or remains debated, it is labelled as such; named discoverers, dates, and “firsts” have each been checked against the historical literature.
Table of Contents
- A Crystal from a Gallstone: Isolation and Naming
- Cracking the Structure: Windaus, Wieland, and the Nobel Prizes
- Anitschkow's Rabbits and the Birth of the Lipid Hypothesis
- Ancel Keys, Framingham, and the Diet–Heart Hypothesis
- Brown, Goldstein, and the LDL Receptor
- Akira Endo and the Statin Era
- The Cholesterol Debate: Skeptics and the Mainstream Evidence
- From Molecule to Modern Management
- Research Papers and References
- Connections
- Featured Videos
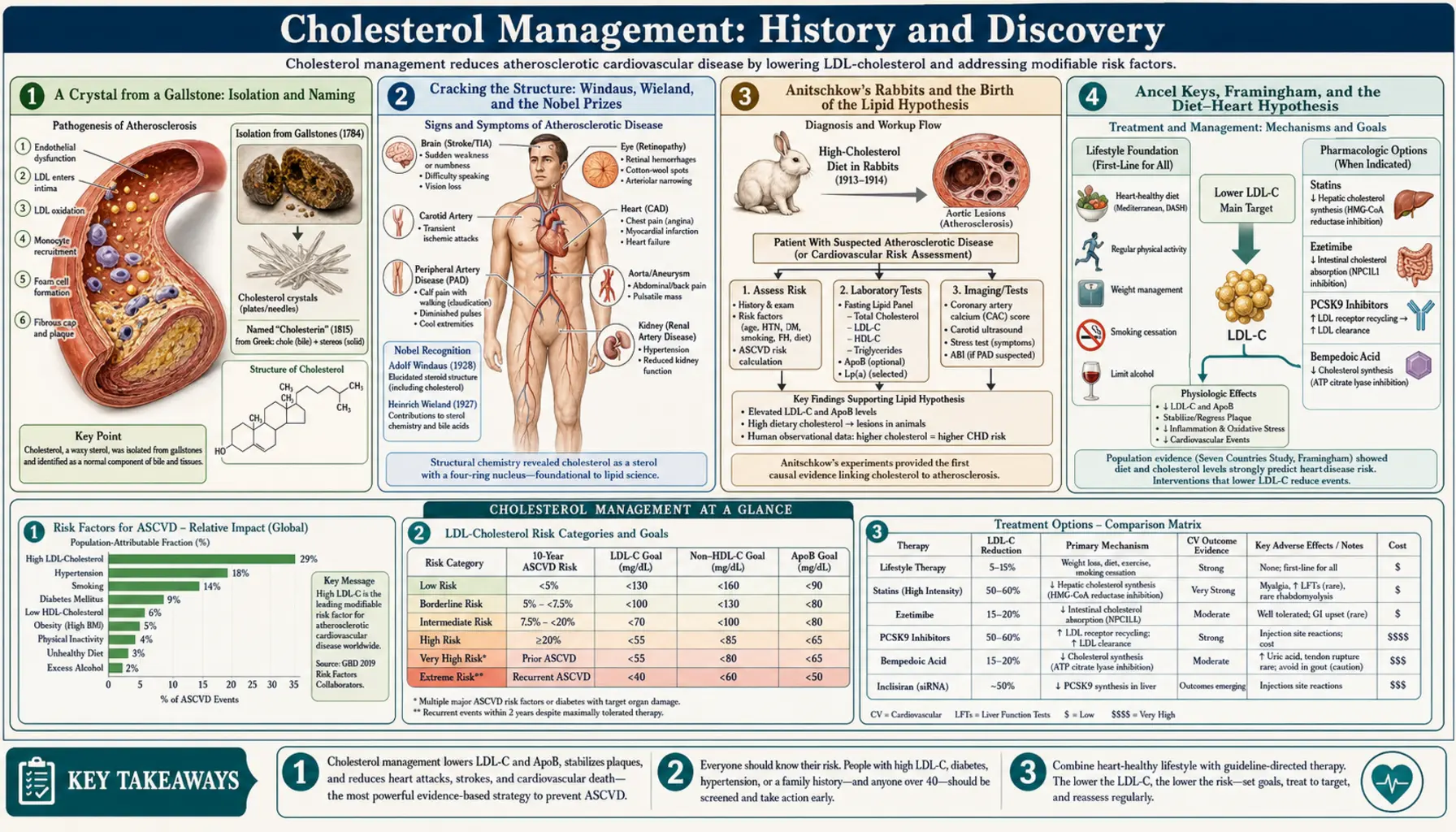
A Crystal from a Gallstone: Isolation and Naming
Cholesterol entered chemistry as something tangible and slightly odd: the pale, pearly, fatty material that makes up most gallstones. In 1769 the French physician and chemist François Poulletier de la Salle obtained it in solid, crystalline form from human gallstones — the first isolation of the substance, though his work went unpublished and was long under-credited. Two decades later the prominent chemist Antoine Fourcroy also examined the waxy component of gallstones (publishing around 1789), helping bring the material to wider scientific notice. For many years it was known simply by descriptive terms tied to its origin in bile and gallstones.
The name we still use was coined by the great French chemist Michel-Eugène Chevreul, a pioneer of the chemistry of fats. In 1815 he named the substance cholesterine, building it from the Ancient Greek cholé (“bile”) and stereós (“solid”) — literally “solid bile,” an apt description of a crystalline compound recovered from gallstones. The modern English form cholesterol came later, when chemists recognized that the molecule carries a hydroxyl (–OH) group and is therefore an alcohol; the “-ol” suffix marks that chemical fact. The two-hundredth anniversary of Chevreul’s naming, in 2015, was marked in the scientific literature.
It is worth pausing on how much was not known at this point. To the chemists of Chevreul’s era, cholesterol was a curious crystalline fat with no understood function and no known connection to disease. Its biological roles — as a building block of every animal cell membrane, the backbone of bile acids, steroid hormones, and vitamin D, and a normal constituent of blood — would take another century and more to uncover. The molecule had a name and a source long before anyone could draw its shape or explain why the body makes it.
Cracking the Structure: Windaus, Wieland, and the Nobel Prizes
Working out the architecture of cholesterol — the now-familiar four-ring steroid skeleton — occupied some of the finest organic chemists of the early twentieth century and earned two consecutive Nobel Prizes in Chemistry. Heinrich Otto Wieland received the 1927 prize for his investigations of bile acids and related substances, which he had pursued since 1912 and which are chemically close kin to cholesterol. The very next year, 1928, Adolf Otto Reinhold Windaus was awarded the prize for his work on the constitution of the sterols and their connection with the vitamins — research that grew directly out of his studies of cholesterol. (The two men were not only contemporaries but brothers-in-law, and they supported each other’s work for decades.)
An honest account must add an important caveat that is often lost in popular retellings. The ring structures that Windaus and Wieland originally proposed for cholesterol and the bile acids turned out to be partly wrong. In 1932, after the physicist J. D. Bernal applied X-ray analysis to sterol crystals and showed the earlier formula could not be correct, Wieland (with Elisabeth Dane) and others arrived at the corrected ring framework that chemists accept today. The complete three-dimensional structure was nailed down only later, when Harry Carlisle and Dorothy Crowfoot (Hodgkin) determined the X-ray crystal structure of cholesteryl iodide in 1945. So the accurate statement is this: the Nobel Prizes of 1927 and 1928 honored the foundational chemistry of bile acids and sterols, but the final, correct structure of cholesterol was settled around 1932 and confirmed by X-ray crystallography in the mid-1940s.
This episode is a useful reminder of how real science proceeds. Brilliant work can earn a Nobel Prize and still contain errors that later evidence corrects; the prize recognized the scope and importance of the chemistry, not a flawless final answer. By the 1930s and 1940s, however, the molecule that began as “solid bile” was fully drawn, its place among the steroids understood, and the stage set for a very different question: what does cholesterol have to do with disease of the heart and arteries?
Anitschkow's Rabbits and the Birth of the Lipid Hypothesis
The link between cholesterol and arterial disease began not in a clinic but in a rabbit hutch in St. Petersburg. In 1913, the young Russian experimental pathologist Nikolai N. Anitschkow (Anichkov), working with his student S. Chalatow, purified cholesterol from egg yolks, dissolved it in sunflower oil, and fed it to ordinary rabbits. Their blood cholesterol rose sharply, and within weeks their arteries developed raised, fatty, yellowish lesions strikingly similar to the atherosclerotic plaques seen in humans. Crucially, Anitschkow showed it was the cholesterol itself — not protein or general overfeeding, as rival groups had supposed — that produced the damage, and that the degree of arterial disease tracked the amount of cholesterol fed.
This experiment is widely regarded as the origin of what became known as the lipid hypothesis of atherosclerosis — the idea that cholesterol and other lipids drive the formation of arterial plaque. Its centenary was celebrated in the medical literature in 2013. At the same time, the rabbit model has well-known limitations: rabbits are herbivores that handle dietary cholesterol very differently from humans, and Anitschkow’s findings were not immediately accepted. For decades many investigators doubted that a result in cholesterol-fed rabbits had any bearing on human heart disease, and the hypothesis remained contested.
What turned a disputed animal finding into a central idea of cardiology was the slow accumulation of human evidence over the following half-century: pathology linking plaque to cholesterol-rich deposits, the discovery that people with inherited very high cholesterol suffer early heart attacks, and large population studies. Anitschkow’s rabbits did not prove the case in humans — but they framed the question that the rest of the twentieth century set out to answer.
Ancel Keys, Framingham, and the Diet–Heart Hypothesis
By the mid-twentieth century, heart attacks had become a leading cause of death in the industrialized world, and the search for causes turned to diet and blood cholesterol. The American physiologist Ancel Keys became the most prominent champion of the diet–heart hypothesis: the proposal that the type and amount of fat in the diet raises serum cholesterol, which in turn raises the risk of coronary heart disease. Keys presented an early version of this hypothesis at a World Health Organization meeting in 1955 and went on to lead the landmark Seven Countries Study, launched in 1958, which followed roughly 13,000 middle-aged men across Finland, Greece, Italy, Japan, the Netherlands, the United States, and Yugoslavia. The study reported that populations with higher saturated-fat intake and higher serum cholesterol tended to have more coronary disease, and it helped popularize the Mediterranean dietary pattern.
Running in parallel, the Framingham Heart Study — a long-term observational study of residents of Framingham, Massachusetts, begun in 1948 — was quietly transforming medicine. Framingham is the study that gave us the very term “risk factor.” By following the same people for decades, it established that high blood cholesterol, along with high blood pressure and smoking, predicted who would later develop coronary heart disease. Together, the Seven Countries Study and Framingham moved blood cholesterol from a laboratory curiosity to a measurable, modifiable predictor of heart disease, and shaped dietary guidelines for a generation.
Honesty requires noting that this body of work has been genuinely controversial. Critics have argued that Keys selected countries that fit his hypothesis and downplayed those that did not, that the early diet–heart story under-weighted the roles of sugar, trans fats, and refined carbohydrate, and that population correlations cannot by themselves prove causation. Some of these criticisms have merit and have reshaped modern nutrition science. What survived the debate is narrower but robust: blood cholesterol — especially LDL cholesterol — is a causal risk factor for atherosclerotic heart disease, even though the precise dietary route to a healthy heart is more complex than “avoid all fat” and remains an active area of research. The diet–heart hypothesis, in short, was partly right, partly oversimplified, and is best understood as one chapter in a longer scientific argument.
Brown, Goldstein, and the LDL Receptor
If the population studies established that blood cholesterol matters, the molecular biologists explained how the body controls it — and in doing so closed much of the causal argument. At the University of Texas Southwestern Medical Center in Dallas, where they were reunited as junior faculty in 1972, Michael S. Brown and Joseph L. Goldstein set out to understand familial hypercholesterolemia, a hereditary condition in which cholesterol is dramatically elevated from birth and heart attacks can strike in childhood or early adulthood.
Their work, beginning with a key paper in 1974, revealed that cells carry a specific surface protein — the low-density lipoprotein (LDL) receptor — that grabs LDL particles from the blood, pulls them into the cell, and signals the cell to dial down its own cholesterol production. People with familial hypercholesterolemia, they showed, inherit faulty or missing LDL receptors, so LDL is not cleared efficiently and piles up in the bloodstream, accelerating atherosclerosis. This was a profound insight: it explained how the body normally regulates cholesterol through a feedback loop, why some people have lethally high levels, and — importantly — it pointed directly at a therapeutic strategy. Anything that increases the number of active LDL receptors on liver cells would pull more LDL out of the blood. Brown and Goldstein were awarded the Nobel Prize in Physiology or Medicine in 1985 for these discoveries concerning the regulation of cholesterol metabolism.
The LDL-receptor story matters for the broader debate because it supplied a mechanism, not just a correlation: it showed a clear, dose-dependent biological pathway by which LDL cholesterol causes disease, and it predicted that lowering LDL by boosting receptor activity should reduce harm. That prediction would soon be tested by a drug discovered, almost simultaneously, on the other side of the world.
Akira Endo and the Statin Era
The most consequential cholesterol drug in history came from a Japanese biochemist’s study of molds. Akira Endo, inspired partly by Alexander Fleming’s work with Penicillium, reasoned that some fungi might produce compounds to block the cholesterol-making machinery of competing microbes. The body builds cholesterol through a long pathway whose rate-limiting step is controlled by the enzyme HMG-CoA reductase; a natural inhibitor of that enzyme, Endo predicted, might lower cholesterol. After screening roughly 6,000 fungal broths, in August 1973 he isolated compactin (also called ML-236B or mevastatin) from the mold Penicillium citrinum — the first statin, and the first HMG-CoA reductase inhibitor.
Compactin itself was not marketed, but it proved the concept and opened the field. A closely related compound, lovastatin (mevinolin), was isolated around 1978–1979 — identified independently from fungi by Endo and by researchers at Merck — and after roughly a decade of testing it became the first statin approved for sale, receiving U.S. FDA approval in 1987. Its arrival launched the “statin era.” Statins lower LDL precisely as the LDL-receptor biology predicted: by partly blocking the liver’s own cholesterol synthesis, they prompt liver cells to make more LDL receptors, which then clear more LDL from the blood. Large randomized trials in the 1990s and beyond went on to show that statins reduce heart attacks, strokes, and deaths in people at elevated risk.
Endo, often called “the father of statins,” reportedly never grew wealthy from a discovery that has benefited tens of millions of people; he received major scientific honors and died in 2024. The statin story also tied the whole history together — the molecule isolated from gallstones, the structure drawn by Nobel chemists, the lipid hypothesis from Anitschkow’s rabbits and Keys’s populations, and the receptor mechanism of Brown and Goldstein — into a single therapeutic chain: identify cholesterol, understand how it is regulated, and design a drug to lower it.
The Cholesterol Debate: Skeptics and the Mainstream Evidence
No honest history of cholesterol can ignore the long-running “cholesterol controversy.” A vocal minority of researchers and clinicians — sometimes called cholesterol skeptics — have argued over the years that the role of cholesterol, and especially of dietary cholesterol and saturated fat, has been overstated; that some early diet studies were selectively reported; that statins are over-prescribed or their benefits exaggerated; and that other factors (inflammation, insulin resistance, sugar and refined carbohydrate, particle size, and overall metabolic health) deserve more attention. Several of these criticisms have substance and have genuinely improved the science: modern guidance, for example, no longer treats dietary cholesterol in food as the prime villain it was once thought to be, and the importance of triglycerides, metabolic syndrome, and diet quality is now widely recognized.
It is also important to distinguish the strong claims from the weak ones. The evidence that blood LDL cholesterol is causally involved in atherosclerotic cardiovascular disease is, in the mainstream scientific view, very strong — and it rests on multiple independent lines of evidence that converge: Anitschkow’s and later animal work; the natural experiment of familial hypercholesterolemia and the LDL-receptor mechanism; large prospective cohorts like Framingham; human genetic studies (Mendelian randomization) showing that people born with lifelong lower LDL have less heart disease; and randomized controlled trials in which lowering LDL — by statins and by other, non-statin drugs — reduces cardiovascular events. Major cardiology and lipid societies regard LDL’s causal role as well established.
The fair summary, then, is twofold. First, healthy skepticism has been valuable: it corrected real oversimplifications in the old “all fat is bad / dietary cholesterol is the enemy” message and broadened the picture to include sugar, inflammation, and metabolic health. Second, the core of the lipid hypothesis — that lowering elevated LDL cholesterol reduces cardiovascular risk — has held up under the most rigorous tests we have. This page presents both sides plainly, but readers deserve to know where the weight of evidence currently lies, and to make decisions about their own cholesterol with a qualified clinician rather than from any single study or headline.
From Molecule to Modern Management
Modern cholesterol management is the inheritance of this entire two-and-a-half-century arc. The simple lipid panel — total cholesterol, LDL, HDL, and triglycerides — descends directly from the chemistry of isolating and measuring the molecule and from the risk-factor framework of Framingham. The drugs descend from Endo’s molds and the Brown–Goldstein receptor: statins remain first-line, now joined by ezetimibe, by PCSK9 inhibitors (which work by sparing LDL receptors from destruction, a strategy made possible by molecular discoveries that built on the LDL-receptor story), and by newer agents such as bempedoic acid and inclisiran. The dietary advice, too, has matured beyond the early diet–heart message into a more nuanced emphasis on overall dietary pattern and metabolic health.
What is striking, looking back, is how each era handed the next a sharper question. The eighteenth-century chemists asked what is this waxy crystal? The Nobel chemists asked what is its structure? Anitschkow and Keys asked does it cause heart disease? Brown and Goldstein asked how does the body control it? And Endo asked can we safely lower it? The answers did not always come cleanly — structures were corrected, hypotheses were oversimplified and revised, and debate continues at the edges — but the cumulative result is one of the best-understood and most treatable risk factors in all of medicine.
For the practical side of this story — what the numbers on a lipid panel mean, lifestyle and dietary strategies, and the medications used today — see the main Cholesterol Management page. The history here is offered for context and understanding; it is not medical advice, and decisions about testing, diet, or cholesterol-lowering medication should be made with a qualified healthcare professional.
Research Papers and References
The references below combine peer-reviewed historical reviews with curated PubMed topic-search links into the primary literature on cholesterol’s discovery, the lipid hypothesis, the LDL receptor, and the statins. Where a stable DOI or PubMed identifier is available it is given; otherwise a PubMed topic search is provided. Each link opens in a new tab.
- Olson RE. Discovery of the lipoproteins, their role in fat transport and their significance as risk factors. Journal of Nutrition. 1998;128(2 Suppl):439S–443S. — PubMed: PMID 9478044
- Chaudhuri A, Anand D. Cholesterol: Revisiting its fluorescent journey on the 200th anniversary of Chevreul’s “cholesterine.” Biomedical Spectroscopy and Imaging. 2017;6(1–2):1–5. — doi:10.3233/BSI-170166
- Vance DE. Cholesterol — naming, isolation, and early chemistry (historical overview). — PubMed: cholesterol history isolation Chevreul Poulletier
- The Nobel Prize in Chemistry 1927 (Heinrich Wieland, bile acids) and 1928 (Adolf Windaus, sterols). — NobelPrize.org: Windaus 1928
- Cholesterol and bile-acid structure determination; correction of the steroid ring system (Bernal, Wieland, Dane; X-ray confirmation by Carlisle and Hodgkin). — PubMed: cholesterol structure steroid ring X-ray
- Steinberg D. In celebration of the 100th anniversary of the lipid hypothesis of atherosclerosis. Journal of Lipid Research. 2013;54(11):2946–2949. — doi:10.1194/jlr.R043414
- Konstantinov IE, et al. Nikolai N. Anitschkow and his theory of atherosclerosis. Texas Heart Institute Journal. 2006;33(4):417–423. — PubMed: PMID 17215962
- Anitschkow NN, Chalatow S. Cholesterol-fed rabbit as a model of experimental atherosclerosis (historical and modern commentary). — PubMed: PMID 9395267
- Keys A. Coronary heart disease in seven countries (Seven Countries Study). Circulation. 1970;41(Suppl 1):I1–I211. — PubMed: Keys Seven Countries Study
- Kannel WB, et al. Factors of risk in the development of coronary heart disease — the Framingham Study. Annals of Internal Medicine. 1961;55:33–50. — PubMed: PMID 13751193
- Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis (Nobel Lecture / review of LDL-receptor biology). Science. 1986;232(4746):34–47. — PubMed: PMID 3513311
- Goldstein JL, Brown MS. History of discovery: the LDL receptor. Arteriosclerosis, Thrombosis, and Vascular Biology. 2009;29(4):431–438. — doi:10.1161/ATVBAHA.108.179564
- Endo A. A historical perspective on the discovery of statins. Proceedings of the Japan Academy, Series B. 2010;86(5):484–493. — doi:10.2183/pjab.86.484
- Ference BA, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease — evidence from genetic, epidemiologic, and clinical studies (EAS Consensus). European Heart Journal. 2017;38(32):2459–2472. — doi:10.1093/eurheartj/ehx144
External Authoritative Resources
- NobelPrize.org — Brown & Goldstein, Physiology or Medicine 1985
- NHLBI (NIH) — Blood Cholesterol
- PubMed — cholesterol history, lipid hypothesis, and statins
Connections
- Cardiology
- Cholesterol Management
- All Conditions
- Atherosclerosis
- Coronary Artery Disease
- Cardiovascular Disease
- Hypertension
- Lipid Panel (Lab Test)
- CoQ10