Neurosyphilis and Tertiary Syphilis: Brain, Heart, and Gummas
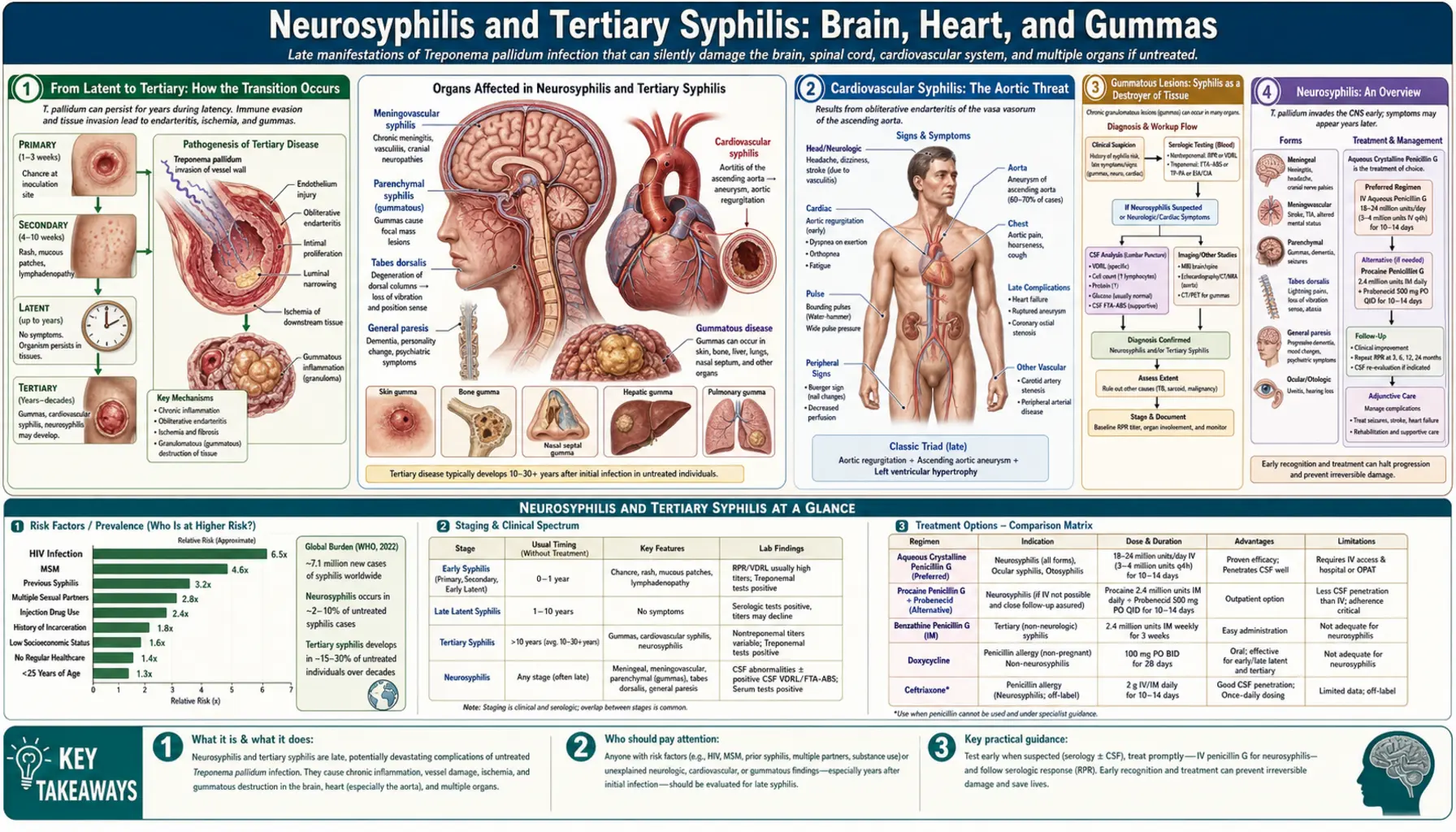
Tertiary syphilis develops years to decades after untreated infection and represents the disease's most destructive phase. The brain (neurosyphilis), heart and aorta (cardiovascular syphilis), and granulomatous lesions called gummas that can form in any organ are the major targets. Before penicillin, tertiary syphilis was one of the leading causes of dementia, blindness, aortic aneurysm, and death in the Western world. With early treatment it is entirely preventable.
Table of Contents
- From Latent to Tertiary: How the Transition Occurs
- Cardiovascular Syphilis: The Aortic Threat
- Gummatous Lesions: Syphilis as a Destroyer of Tissue
- Neurosyphilis: An Overview
- Syphilitic Meningitis and Cranial Nerve Palsies
- Tabes Dorsalis and General Paresis
- Syphilis-HIV Co-infection: Accelerated Neurologic Disease
- CSF Testing for Neurosyphilis
- Prognosis and Modern Outcomes
- Historical Impact: The Great Imitator
- Key Research Papers
- Featured Videos
1. From Latent to Tertiary: How the Transition Occurs
After the secondary stage resolves, syphilis enters a latent phase characterized by a complete absence of symptoms. The bacteria do not disappear — they persist in tissues throughout the body, particularly in lymph nodes, the aortic wall, the meninges, and the central nervous system. The immune system contains but does not eliminate them.
Without treatment, approximately 25 to 40% of people with latent syphilis will eventually develop tertiary disease. The transition typically takes 10 to 30 years, though it can occur earlier. The specific form of tertiary disease that develops (cardiovascular, neurosyphilitic, or gummatous) appears to depend on the individual's immune response, but this is not predictable in advance. The remaining 60 to 75% of untreated people never develop symptomatic tertiary disease — they die of unrelated causes with spirochetes still present in their tissues.
The pre-penicillin Oslo study, which followed 1,147 untreated syphilis patients for decades beginning in 1891, provided much of what we know about the natural history: approximately 9.4% developed cardiovascular syphilis, 6.5% developed neurosyphilis, and 15% developed gummas in some form. These percentages underestimate the true burden because many patients died before reaching the tertiary stage.
2. Cardiovascular Syphilis: The Aortic Threat
Cardiovascular syphilis targets the aorta and is one of the most dramatic manifestations of the tertiary stage. It develops in 10 to 15% of untreated patients, typically 10 to 30 years after initial infection.
The pathological process begins when spirochetes infect the vasa vasorum — the network of tiny blood vessels that nourish the wall of the aorta itself. This triggers a granulomatous inflammation (obliterative endarteritis) that progressively destroys the media (the muscular middle layer) of the aortic wall. The loss of elastic and muscular tissue weakens the wall and leads to dilatation. The result is:
- Syphilitic aortitis: The foundational lesion — chronic inflammation of the aortic wall. Often asymptomatic until complications develop.
- Aortic aneurysm: The weakened wall bulges outward. Syphilitic aneurysms preferentially affect the ascending aorta and aortic arch, in contrast to the atherosclerotic aneurysms that classically affect the abdominal aorta. The bulging aneurysm can compress adjacent structures — the trachea, bronchi, esophagus, or superior vena cava — causing symptoms long before rupture.
- Aortic regurgitation: As the aortic root dilates, the aortic valve leaflets are pulled apart, causing aortic valve incompetence and backward flow of blood into the left ventricle. The resulting volume overload causes progressive heart failure.
- Coronary ostial stenosis: The inflammatory process can narrow the openings of the coronary arteries as they emerge from the aortic root, causing angina and myocardial infarction.
Modern treatment with penicillin halts the progression of active aortitis but cannot reverse established structural damage. A dilated aorta remains dilated; a regurgitant valve requires surgical repair or replacement.
3. Gummatous Lesions: Syphilis as a Destroyer of Tissue
Gummas are the least dramatic but most widely distributed form of tertiary syphilis. They are soft, rubbery, granulomatous nodules — collections of inflammatory cells surrounding a central area of necrosis — that can form anywhere in the body. Common sites include:
- Skin: Nodular or ulcerating lesions, often with a serpiginous (winding, snake-like) edge as central areas heal and the edge progresses.
- Bone: Particularly the tibia, skull, and palate. Gummas destroy bone locally, causing painful periostitis and bony defects. Palatal gummas can perforate the hard palate, connecting the mouth to the nasal cavity.
- Liver: Gummatous hepatitis causing lobular scarring and hepatic dysfunction.
- Brain: Rare cerebral gummas that behave like space-occupying lesions on imaging, mimicking brain tumors.
- Testis: Painless testicular enlargement from gumma formation, historically a recognized clinical entity.
The good news about gummas: they respond extremely well to penicillin, even at this late stage. Unlike the structural damage of cardiovascular syphilis or the neuronal loss of neurosyphilis, gummas are inflammatory lesions that can largely resolve with treatment.
4. Neurosyphilis: An Overview
Neurosyphilis refers to infection of the nervous system by T. pallidum. Technically, spirochetes can invade the cerebrospinal fluid (CSF) very early in infection — within weeks of primary syphilis — making "early neurosyphilis" a recognized entity. Late neurosyphilis, which causes the devastating clinical syndromes described below, typically develops years to decades after untreated infection.
The modern landscape of neurosyphilis has shifted. The classic late forms (tabes dorsalis, general paresis) are rare in countries with working healthcare systems. What clinicians now encounter most often are:
- Ocular syphilis: Uveitis, retinitis, and optic neuritis. These can occur at any stage of syphilis. Syphilis is now a significant cause of infectious uveitis in STI-endemic cities.
- Otosyphilis: Sudden sensorineural hearing loss, tinnitus, and vertigo. Can be rapidly progressive and is treatable if diagnosed early.
- Meningeal and meningovascular neurosyphilis: Meningitis-like presentations and strokes in young people (discussed below).
- Classic late forms: Still seen, but less commonly, especially in HIV-positive populations where progression can be accelerated.
5. Syphilitic Meningitis and Cranial Nerve Palsies
Syphilitic meningitis is a form of early neurosyphilis occurring within the first two years of infection. Patients present with headache, neck stiffness, photophobia, nausea, and vomiting — the classic syndrome of meningitis. Unlike bacterial meningitis, the onset is usually subacute over days to weeks rather than explosive over hours, and it is rarely fatal without treatment.
The cranial nerves are vulnerable to syphilitic meningitis, because they travel through the meningeal spaces that become inflamed. Cranial nerve palsies can cause:
- Facial nerve palsy (CN VII) — one-sided facial weakness, resembling Bell's palsy
- Hearing loss and vertigo (CN VIII) — the basis of otosyphilis
- Eye movement abnormalities (CN III, IV, VI) — double vision, drooping eyelid
- Optic neuritis (CN II) — visual loss
Meningovascular neurosyphilis is a more severe form in which spirochetal inflammation targets the blood vessels supplying the brain (endarteritis obliterans). The narrowed vessels can occlude, causing ischemic strokes. A stroke in a person aged 25 to 45 without typical cardiovascular risk factors should always prompt syphilis testing. The onset may be preceded by weeks of prodromal symptoms — headache, dizziness, insomnia, personality change — that distinguish it from embolic strokes.
6. Tabes Dorsalis and General Paresis
The two classic late forms of neurosyphilis represent the endpoints of different pathological processes within the nervous system:
Tabes dorsalis results from degeneration of the posterior columns and posterior nerve roots of the spinal cord. The posterior columns carry proprioception (sense of limb position) and vibration sense upward to the brain. When they degenerate:
- The patient loses the ability to feel where their feet are without looking — leading to the characteristic high-stepping, stamping gait (they slap their feet down hard to get sensory feedback they can no longer receive from the spinal cord)
- Romberg sign is positive: the patient can stand with feet together when eyes open, but sways dramatically when eyes are closed, because vision is compensating for lost proprioception
- Lancinating pains — sudden, severe, shooting pains in the legs, lasting seconds, described by patients as "lightning" or "electric shock" pains
- Bladder dysfunction from loss of sacral nerve root function — urinary retention and overflow incontinence
- Argyll Robertson pupils — bilaterally small, irregular, asymmetric pupils that accommodate (constrict when focusing on a near object) but do not react to light (the light reflex arc is interrupted, but the accommodation arc is not). This finding is highly specific for neurosyphilis.
- Charcot joints (neuropathic arthropathy) from loss of joint position sense and pain sensation, leading to painless destruction of large joints
General paresis of the insane (GPI) results from direct invasion and destruction of cerebral cortex neurons by spirochetes. It develops 15 to 25 years after initial infection. Early features include personality change, irritability, poor concentration, forgetfulness, and grandiose delusions. Over months to years it progresses to:
- Frank dementia with severe memory loss
- Psychosis, including delusions of grandeur ("I am the Emperor Napoleon") that were historically so characteristic they led to the name "general paresis of the insane"
- Seizures
- Progressive motor dysfunction, tremor, and dysarthria (slurred speech)
- Death within two to five years if untreated
GPI was responsible for filling substantial portions of 19th- and early 20th-century psychiatric hospitals. Julius Wagner-Jauregg won the Nobel Prize in 1927 for treating GPI with deliberate malaria infection (pyrotherapy), the only Nobel Prize awarded for a psychiatric treatment, before penicillin superseded this approach.
7. Syphilis-HIV Co-infection: Accelerated Neurologic Disease
HIV immunosuppression significantly alters the course of syphilis, particularly its neurologic complications. Several patterns have been observed:
- Earlier and more frequent neurosyphilis: People with HIV progress to neurologic involvement faster and at higher rates than HIV-negative people with syphilis. Neurosyphilis has been reported in HIV-positive patients with early-stage syphilis who would not normally be expected to develop it.
- More aggressive presentations: Ocular syphilis (uveitis, retinitis) and rapidly progressive neurologic deficits occur more commonly in HIV co-infection.
- Altered serologic responses: HIV-related immune dysregulation can cause atypically high RPR titers (prozone phenomenon) or, in severely immunocompromised patients, falsely negative non-treponemal tests. CSF analysis is therefore required in more scenarios when HIV is present.
- Lower threshold for lumbar puncture: Current guidelines recommend CSF examination in any HIV-positive patient with syphilis of more than one year's duration, unknown duration, or any neurologic/ophthalmologic symptoms — a broader indication than for HIV-negative patients.
8. CSF Testing for Neurosyphilis
Lumbar puncture and cerebrospinal fluid analysis is essential for diagnosing neurosyphilis. The procedure involves inserting a needle between the lumbar vertebrae to collect a small sample of the fluid that surrounds the brain and spinal cord. Key CSF findings in neurosyphilis include:
- CSF-VDRL (Venereal Disease Research Laboratory): When positive, this is highly specific for neurosyphilis — almost diagnostic. However, it is relatively insensitive: it is negative in up to 70% of neurosyphilis cases. A negative CSF-VDRL does not rule out neurosyphilis.
- CSF pleocytosis: Elevated white blood cell count (>5 white blood cells per microliter) indicates inflammation of the meninges. Present in most symptomatic neurosyphilis.
- Elevated CSF protein: Protein levels above 45 mg/dL suggest meningeal inflammation.
- CSF-FTA-ABS: A treponemal test on CSF. Highly sensitive but not specific — can be positive from passively transferred antibody. A negative result may be useful for ruling out neurosyphilis.
When to consider lumbar puncture: neurologic symptoms (including hearing loss, vision changes, headache, psychiatric symptoms), treatment failure, HIV co-infection with late latent or unknown-duration syphilis, or tertiary syphilis of any type.
9. Prognosis and Modern Outcomes
The prognosis of tertiary syphilis depends heavily on how much organ damage has already occurred when treatment begins. The key principle: antibiotic therapy kills the spirochetes and halts the destructive process, but it cannot reverse established structural damage.
- Gummas: Excellent response to penicillin. Lesions resolve within weeks to months. Skin and bone gummas leave some scarring.
- Cardiovascular syphilis: Penicillin halts progression. An existing aortic aneurysm remains at risk of enlargement and rupture. Aortic regurgitation from root dilatation requires surgical assessment. Coronary ostial stenosis may require angioplasty or bypass. Overall prognosis has improved dramatically since the antibiotic era.
- Early neurosyphilis (meningitis, meningovascular): Good response to high-dose IV penicillin. Neurologic deficits from stroke may partially or fully recover; hearing loss from otosyphilis has variable recovery but benefits from early treatment.
- Ocular syphilis: Responds to IV penicillin; visual prognosis depends on promptness of treatment and extent of retinal or optic nerve damage.
- Late neurosyphilis (tabes dorsalis, GPI): Penicillin halts or slows progression but cannot restore lost neurons. Established dementia in GPI does not fully reverse. Neuropathic pain of tabes may improve partially.
10. Historical Impact: The Great Imitator
Syphilis was called "the great imitator" because its many manifestations mimic so many other conditions — a sobriquet that remains entirely apt. But to appreciate its historical significance, consider what syphilis did before penicillin was discovered in 1928 and introduced into clinical use in the 1940s:
- It was one of the most common serious diseases in the Western world, with infection rates far exceeding current levels.
- It was a major cause of psychiatric institutionalization — general paresis of the insane filled hospital wards.
- It was a leading cause of blindness, deafness, aortic aneurysm, stroke in young adults, and death.
- It ended or derailed the lives of historical figures including Franz Schubert, Friedrich Nietzsche, Édouard Manet, Al Capone, and Henry VIII (disputed).
- The Tuskegee syphilis study (1932–1972), in which the US Public Health Service deliberately withheld penicillin from 399 Black men with syphilis, remains one of the most notorious ethical violations in medical history and continues to shape justified distrust of medical institutions in Black communities.
Understanding this history matters today: the tools to prevent every case of tertiary syphilis exist and have existed for 80 years. The current resurgence is not a failure of medicine — it is a failure of public health infrastructure, equitable access to care, and political will to fund STI prevention.
Key Research Papers
- Marra CM, Maxwell CL, Smith SL, et al. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory features. J Infect Dis. 2004;189(3):369–376. PMID 14745693
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187. PMID 34292926
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382(9):845–854. PMID 32101666
- Peeling RW, Mabey D, Kamb ML, et al. Syphilis. Nat Rev Dis Primers. 2017;3:17073. — Search PubMed
- de Voux A, Kidd S, Torrone EA. Reported cases of neurosyphilis among early syphilis cases — United States, 2009 to 2015. Sex Transm Dis. 2018;45(1):39–41. — Search PubMed
- Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007;44(9):1222–1228. PMID 17407043
- Johns DR, Tierney M, Felsenstein D. Alteration in the natural history of neurosyphilis by concurrent infection with the human immunodeficiency virus. N Engl J Med. 1987;316(25):1569–1572. — Search PubMed
- Lukehart SA. Scientific monogamy: thirty years dancing with the same bug: 2007 Thomas Parran Award Lecture. Sex Transm Dis. 2008;35(1):2–7. — Search PubMed
- Merritt HH, Adams RD, Solomon HC. Neurosyphilis. Oxford University Press; 1946. — The foundational clinical monograph on neurosyphilis presentations, still referenced in modern teaching.
- French P. Syphilis. BMJ. 2007;334(7585):143–147. PMID 17235095
Connections
- All Bacteria
- Treponema pallidum (Syphilis) Hub
- Syphilis Symptoms & Stages Overview
- Primary & Secondary Syphilis
- Syphilis Diagnosis: Serologic Tests
- Penicillin G Treatment
- Meningitis
- Dementia
- Aortic Aneurysm
- All Conditions
- Syphilis — disease overview covering every stage from chancre to tertiary.