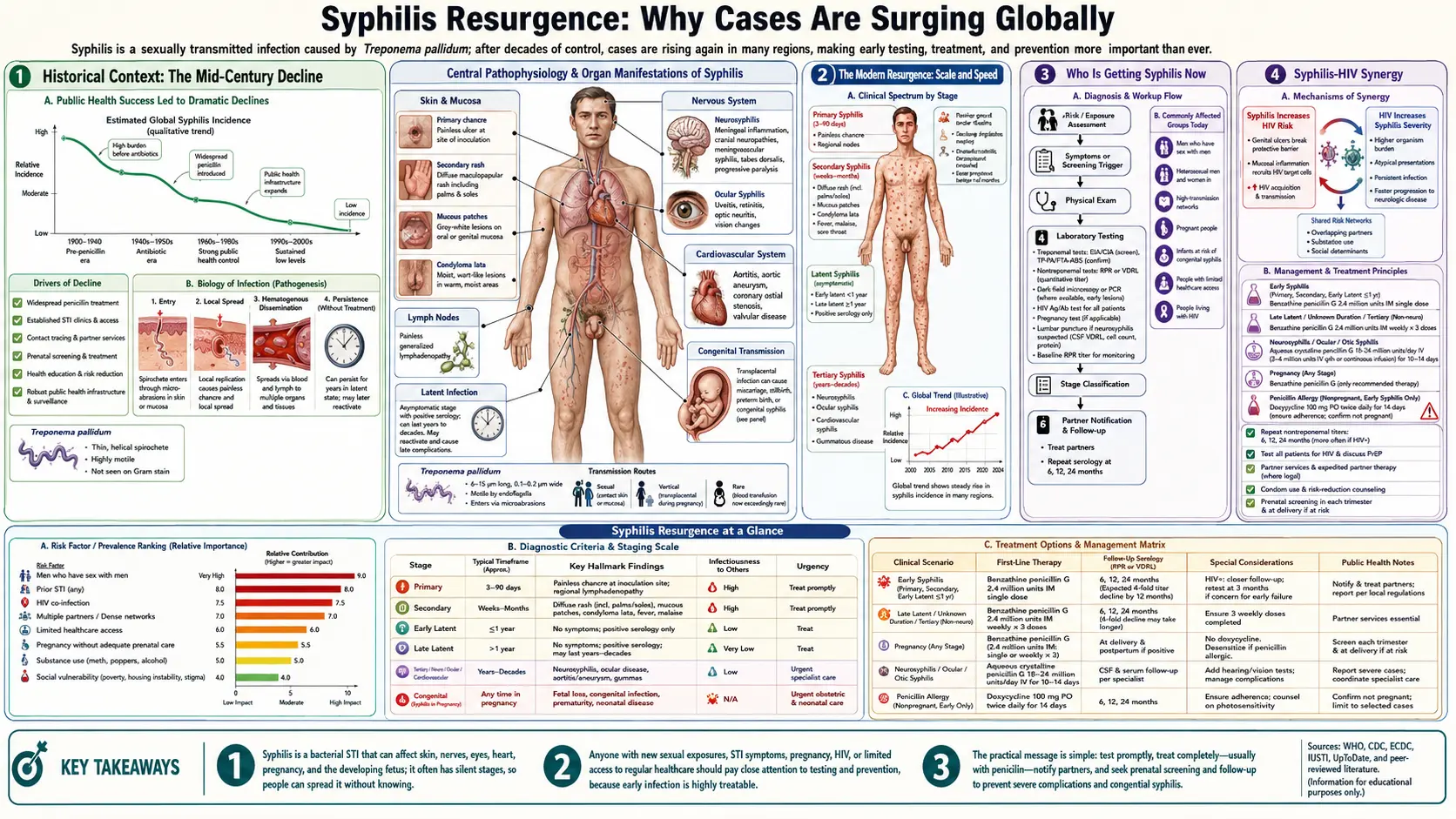
Syphilis Resurgence: Why Cases Are Surging Globally
Syphilis was on a trajectory toward elimination in the United States in the late 1990s. In 2000, the CDC launched a National Plan to Eliminate Syphilis. That plan failed. By 2022, the US recorded over 207,000 syphilis cases — the highest count since 1950 — and more than 3,700 congenital syphilis cases with 231 deaths. The resurgence is global: the same upward trajectory is seen across Europe, Australia, Canada, and parts of Asia. Understanding why matters for anyone trying to protect themselves or others from this preventable disease.
Table of Contents
- Historical Context: The Mid-Century Decline
- The Modern Resurgence: Scale and Speed
- Who Is Getting Syphilis Now
- Syphilis-HIV Synergy
- The Congenital Syphilis Surge
- Behavioral Factors: Apps, Condoms, PrEP
- Structural Factors: Funding Cuts and Lost Capacity
- Why There Is No Vaccine
- Global Control Strategies: What Works
- Key Research Papers
- Featured Videos
1. Historical Context: The Mid-Century Decline
Before penicillin, syphilis was one of the leading causes of serious illness and death in the Western world. The introduction of penicillin G in 1943 and its rapid roll-out through the late 1940s produced one of the most dramatic disease control successes in medical history: primary and secondary syphilis cases in the US fell from approximately 575,000 in 1943 to just 6,000 in 1956 — a 99% drop in 13 years.
Cases crept back up in the 1960s and 1970s (primarily driven by MSM transmission) and fell again in the late 1980s and 1990s after the AIDS crisis prompted widespread behavior change and expansion of STI infrastructure. In 2000, the US rate reached its lowest point in recorded history — 2.1 cases per 100,000 population.
That was the bottom. Since 2001, primary and secondary syphilis rates have climbed every year except 2013. The post-2012 acceleration has been particularly steep.
2. The Modern Resurgence: Scale and Speed
By the numbers, the scale of the resurgence is striking:
- 2000: 5,979 primary and secondary syphilis cases in the US (rate: 2.1/100,000)
- 2012: 15,667 cases
- 2016: 27,814 cases
- 2020: 41,655 cases
- 2022: 50,781 primary and secondary cases; 207,255 total syphilis cases of all stages
The 2022 primary and secondary rate of 15.4 cases per 100,000 is the highest since 1950. Including all stages, the total burden has more than doubled in a decade. Similar trajectories are documented in the United Kingdom (where rates hit a 70-year high in 2022), Germany, France, Australia, and Canada.
The speed of the acceleration matters: this is not a slow drift upward but a compounding epidemic. Sexual networks in which syphilis is circulating grow the epidemic exponentially rather than linearly when each case generates more than one new case — a situation that current rates strongly suggest is occurring.
3. Who Is Getting Syphilis Now
The epidemiology of syphilis has shifted substantially since the early 2000s:
Gay, bisexual, and men who have sex with men (MSM) were and remain disproportionately affected, accounting for approximately 40 to 50% of primary and secondary syphilis cases in the US — a much higher rate than their share of the population. However, their share of total cases has declined as heterosexual transmission has risen sharply.
Heterosexual women and their male partners now drive an increasing proportion of total cases. The rate among women of all ages has increased more than tenfold since 2012 (from 0.9 to 9.3 cases per 100,000 in 2022). This shift in female rates directly drives the congenital syphilis epidemic.
People who use drugs, particularly methamphetamine and opioids, are now a major affected population. Methamphetamine use is strongly associated with exchange of sex for drugs, reduced impulse control and condom use, and delayed healthcare seeking. Studies in several US cities find meth use in 30 to 60% of recently diagnosed MSM syphilis cases. The opioid epidemic has created overlapping vulnerabilities in many communities.
Homeless and housing-unstable populations have substantially higher syphilis rates, reduced access to routine testing, and face barriers to completing partner notification.
Young adults (ages 20–29) have the highest reported rates in the US. However, cases have increased in all age groups.
4. Syphilis-HIV Synergy
Syphilis and HIV interact in ways that amplify both epidemics:
- Syphilis facilitates HIV transmission. Genital ulcers (primary syphilis chancres) disrupt the mucosal barrier, creating a portal of entry for HIV. Studies estimate that a syphilitic ulcer increases HIV transmission risk two- to fivefold per sexual encounter. A person with active syphilis is also more infectious for HIV: genital inflammation increases HIV shedding at mucosal surfaces.
- HIV increases neurosyphilis risk. HIV-positive individuals with syphilis are substantially more likely to develop neurosyphilis, experience more aggressive disease progression, and have atypical presentations that are harder to diagnose. Some research suggests HIV-positive individuals should be treated with IV penicillin if they have neurologic or ophthalmic symptoms, rather than the standard IM regimen.
- Both thrive in the same sexual networks. The sexual networks where HIV circulates are largely the same networks where syphilis circulates. A newly diagnosed case of either infection is a signal to screen for the other.
- PrEP era effects: HIV PrEP use in high-risk MSM is associated with reduced condom use in some studies, and with higher rates of gonorrhea and syphilis diagnosis — not because PrEP causes STIs but because PrEP users represent populations at highest risk, and because HIV fear was previously a major driver of condom use in MSM networks.
5. The Congenital Syphilis Surge
The congenital syphilis epidemic is the most devastating consequence of the resurgence. In 2022, the US reported 3,761 congenital syphilis cases, including 231 deaths (stillbirths and neonatal deaths) — a rate of 79.0 per 100,000 live births, eleven times the 2012 rate of 7.8.
Every case is preventable. Analysis of case records consistently identifies systemic failures:
- Approximately 40% of mothers had no prenatal care or inadequate prenatal care
- Among those who had prenatal care, some were tested but not treated (lab result not followed up, patient lost to follow-up)
- Some were treated but within 30 days of delivery (too late to fully protect the fetus)
- Some tested negative in the first trimester but acquired syphilis later and were not retested
The disparities are severe. Black, American Indian/Alaska Native, and Hispanic/Latino infants are affected at rates many times higher than non-Hispanic white infants. These disparities mirror access to prenatal care, housing stability, and drug treatment availability.
6. Behavioral Factors: Apps, Condoms, PrEP
Three behavioral trends have contributed to the resurgence, though quantifying each is difficult:
Dating and hookup apps have altered the social structure of sexual networks in ways that facilitate syphilis spread. Apps enable rapid partner matching with individuals outside one's existing social network, increasing exposure to infected partners in other communities and reducing the reach of traditional partner notification (it is much harder to notify a partner you met on an app and whose last name you do not know). Apps also enable faster partner turnover in some networks, increasing the number of exposures per unit time.
Declining condom use in key populations is documented across multiple surveillance systems. Among MSM, condom use declined as HIV fear decreased — a consequence of highly effective antiretroviral therapy and PrEP reducing HIV mortality and perceived risk. Among heterosexual populations, long-acting contraceptive methods reduce pregnancy risk without preventing STI transmission, and condom use for STI prevention may not be consistently adopted as a separate practice.
PrEP and risk compensation: Multiple studies find that MSM on PrEP have higher rates of gonorrhea, chlamydia, and syphilis than HIV-negative MSM not on PrEP. The most likely explanation is risk compensation — people protected against what they most feared (HIV) relax other protective behaviors. This is not a reason to discourage PrEP; it is a reason to integrate regular STI screening into PrEP delivery programs.
7. Structural Factors: Funding Cuts and Lost Capacity
Behavioral factors alone do not explain the magnitude of the resurgence. Structural failures in public health infrastructure are equally important:
STI clinic closures: Many local health departments closed or consolidated STI clinics following federal and state funding cuts in the 2000s and 2010s. The infrastructure that once tested hundreds of thousands of people annually in dedicated STI settings was reduced or eliminated in many cities. When syphilis rates began to climb, the capacity to respond was diminished.
Contact tracing and disease intervention specialists (DIS): Traditional syphilis control relied heavily on DIS — trained public health workers who interview newly diagnosed patients, identify and notify sexual partners, and ensure partners receive testing and treatment. DIS staffing was cut dramatically during the austerity period. When syphilis rates began to climb, there were not enough DIS to interrupt transmission chains before they spread.
COVID-19 pandemic disruptions (2020–2021): Healthcare disruptions, clinic closures, and redeployment of public health workers to pandemic response contributed to a spike in syphilis cases. Surveillance systems were also disrupted, potentially underestimating 2020–2021 case counts.
Benzathine penicillin G shortages: Periodic supply chain disruptions have reduced availability of the first-line treatment in some US and global markets, forcing use of alternative regimens with less proven efficacy, particularly for pregnant women.
8. Why There Is No Vaccine
The absence of a syphilis vaccine is one of the major reasons control is so difficult. Reinfection after treatment is common and carries the same risk as initial infection — there is no durable protective immunity from natural infection or from previous treatment.
Vaccine development against Treponema pallidum has been attempted for decades and has consistently failed to produce a clinically usable candidate. The core challenge: the bacterium that causes syphilis has never been successfully cultured in the laboratory outside a living host. Standard vaccine development requires isolating the organism, growing large quantities of it, identifying its immunogenic surface proteins, and developing formulations that elicit protective immune responses. The inability to culture T. pallidum blocks every step of this traditional pathway.
Modern genomic approaches have identified candidate surface antigens (particularly members of the TP0965 and Tp17 families of outer membrane proteins), and these are under investigation in animal models. Whole-genome sequencing of T. pallidum in 1998 provided the complete list of targets. Animal model studies in rabbits have shown partial protection with some antigen formulations. However, rabbit immunity does not always predict human immunity, and the path from rabbit protection studies to human clinical trials remains long.
The challenge is compounded by the organism's remarkable ability to evade the immune system: natural syphilis infection does not produce solid immunity, so even if a vaccine elicited the same immune response as natural infection, it might provide only partial protection. Vaccine candidates need to do better than natural infection at eliciting neutralizing antibodies against surface antigens that vary between strains.
9. Global Control Strategies: What Works
Despite the resurgence, there are demonstrated approaches to syphilis control that work when consistently implemented:
- Universal prenatal screening and treatment: Countries and regions that achieve high antenatal screening coverage and rapid treatment eliminate congenital syphilis. Cuba became the first country certified by the WHO as having eliminated mother-to-child transmission of syphilis in 2015. Thailand achieved the same in 2017. The difference between success and the US situation is not the medicine — it is political commitment to universal prenatal care.
- Rapid testing and same-day treatment: Deployment of rapid point-of-care syphilis tests in settings where people actually seek care (emergency departments, drug treatment programs, homeless shelters, jails, antenatal clinics) and immediate same-day treatment when a positive result is found dramatically shortens the time from infection to treatment.
- Rebuilding DIS capacity: Contact tracing works. Countries and jurisdictions that maintained robust disease intervention specialist programs have better controlled their epidemics. The cost is much less than treating the consequences of uncontrolled spread.
- Doxycycline post-exposure prophylaxis (doxy-PEP): Clinical trial evidence (IPERGAY, DOXYVAC, DoxyPEP) shows that taking doxycycline 200 mg within 72 hours of condomless sex reduces syphilis (and chlamydia) acquisition in high-risk MSM by 70 to 80%. CDC guidelines now include doxy-PEP as an option for this population. Implementation requires prescribers comfortable discussing this intervention and patients who can access doxycycline.
- Integration of STI and HIV care: When STI screening and treatment are integrated into HIV care settings (PrEP clinics, HIV primary care), high-risk populations are reached at regular intervals with both services simultaneously.
Key Research Papers
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382(9):845–854. PMID 32101666
- Peeling RW, Mabey D, Kamb ML, et al. Syphilis. Nat Rev Dis Primers. 2017;3:17073. — Search PubMed
- Luetkemeyer AF, Donnell D, Dombrowski JC, et al. Postexposure doxycycline to prevent bacterial sexually transmitted infections. N Engl J Med. 2023;388(14):1296–1306. — Search PubMed
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187. PMID 34292926
- French P, Gomberg M, Janier M, et al. Resurgent syphilis across the globe: a public health perspective on bridging surveillance and strategic interventions. Pathogens. 2025;14(11):1148. doi:10.3390/pathogens14111148
- Pathela P, Braunstein SL, Schillinger JA, Shepard CW, Blank S. Men who have sex with men have a 140-fold higher risk for newly diagnosed HIV and syphilis compared with heterosexual men in New York City. J Acquir Immune Defic Syndr. 2011;58(4):408–416. — Search PubMed
- Stamm LV. Syphilis: antibiotic treatment and resistance. Epidemiol Infect. 2015;143(8):1567–1574. — Search PubMed
- Lukehart SA, Godornes C, Molini BJ, et al. Macrolide resistance in Treponema pallidum in the United States and Ireland. N Engl J Med. 2004;351(2):154–158. PMID 15247355
- Hicks CB, Benson PM, Lupton GP, Tramont EC. Seronegative secondary syphilis in a patient infected with the human immunodeficiency virus (HIV) with Kaposi sarcoma. Ann Intern Med. 1987;107(4):492–495. — Search PubMed
- Bowen V, Su J, Torrone E, Kidd S, Weinstock H. Increase in incidence of congenital syphilis — United States, 2012–2014. MMWR Morb Mortal Wkly Rep. 2015;64(44):1241–1245. — Search PubMed
Connections
- Treponema pallidum (Syphilis) Hub
- Syphilis Treatment & Prevention
- Congenital Syphilis
- Penicillin G Treatment
- Syphilis Symptoms & Stages
- Neurosyphilis & Tertiary Syphilis
- All Bacteria
- Infectious Disease
- All Conditions
- Syphilis — background on the infection whose case counts are now climbing again.