Streptococcus pyogenes (Group A Strep): Strep Throat, Scarlet Fever, and Rheumatic Fever
Symptoms & Diagnosis
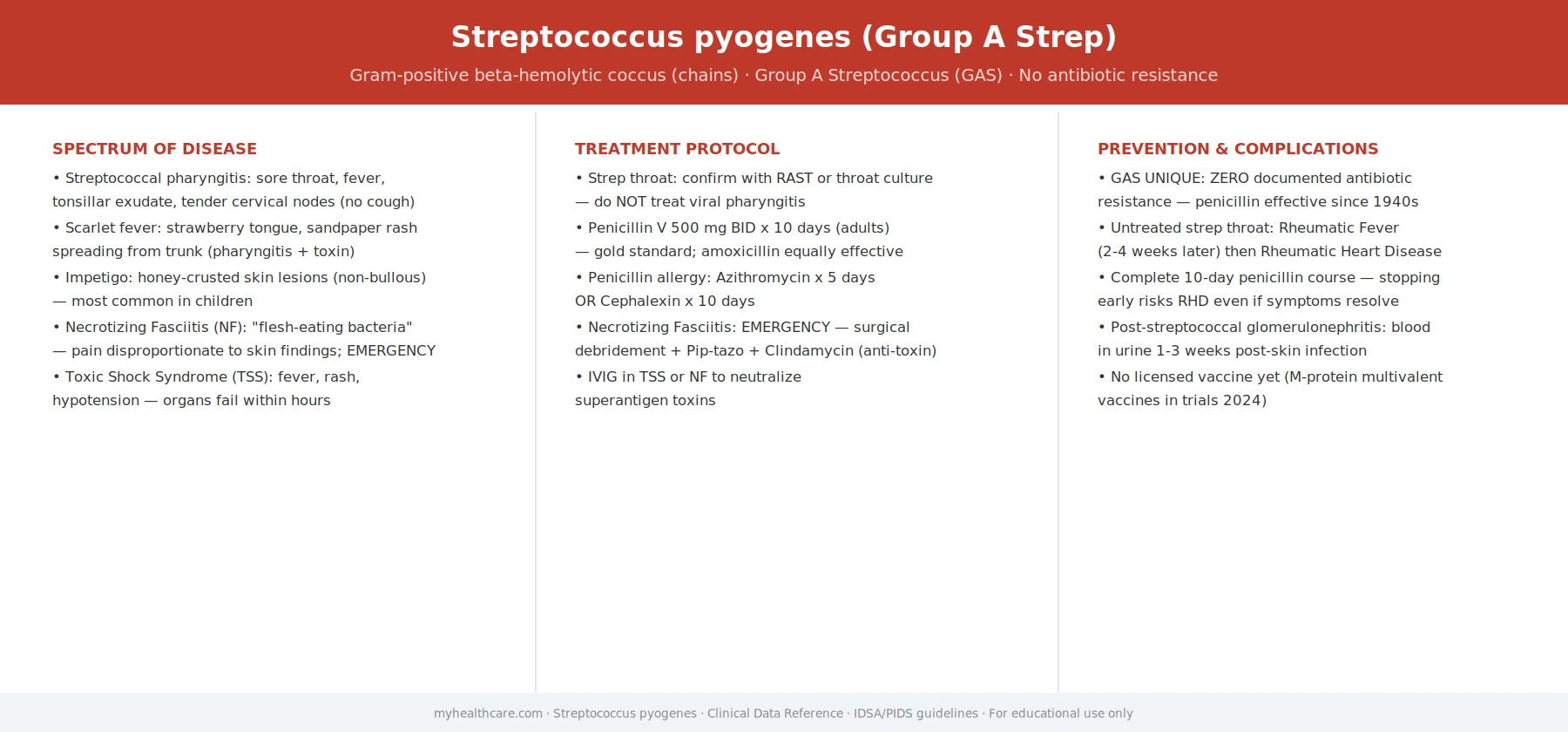
Sore throat, fever, and the full spectrum from strep throat to life-threatening invasive disease.
Strep Throat
The classic sudden sore throat, white patches, swollen lymph nodes, and no cough.
Invasive Disease
Necrotizing fasciitis, streptococcal toxic shock, and why invasive GAS kills so fast.
Diagnosis Tests
Rapid antigen tests (RADT) and throat culture — when to use each.
Treatment & Prevention
Penicillin remains fully effective — why GAS has never developed resistance.
Antibiotic Treatment
Penicillin V, amoxicillin, and alternatives for penicillin allergy.
Prevention & Vaccines
Hygiene, preventing spread, and the long quest for a strep vaccine.
Complications
Rheumatic fever, rheumatic heart disease, and post-streptococcal glomerulonephritis.
Streptococcus pyogenes — commonly called Group A Strep (GAS) — is a bacterium that causes strep throat in tens of millions of children every year. For most people, it is a sore throat that clears up quickly with antibiotics. But Group A Strep is also behind scarlet fever, the skin infection impetigo, and the rare but life-threatening flesh-eating disease (necrotizing fasciitis). Most importantly, when a strep throat goes untreated, the immune system's reaction to the bacteria can trigger rheumatic fever — a condition that can permanently scar the heart valves and leave lasting heart damage. Understanding Group A Strep means knowing not just how to treat a sore throat quickly, but why treating it promptly matters so much.
Table of Contents
- What Group A Strep Is
- Strep Throat — Symptoms and Diagnosis
- Scarlet Fever
- Impetigo and Skin Infections
- Invasive Disease — Necrotizing Fasciitis and Toxic Shock
- Rheumatic Fever and Heart Damage
- Treatment
- Research Papers
- Connections
- Featured Videos
What Group A Strep Is
Streptococcus pyogenes is a gram-positive bacterium that lives only in humans — it does not survive in the environment or animals. The name gives hints to its character: streptococcus means "chain of spheres" (the bacteria grow in linked chains), and pyogenes is Latin for "pus-forming." Its designation as Group A comes from a laboratory classification by the polysaccharide molecules on its surface, developed by Rebecca Lancefield in the 1930s to sort streptococcal species.
GAS spreads almost exclusively by respiratory droplets and direct contact with infected secretions. An infected person spreads it by coughing, sneezing, or sharing drinks and eating utensils. Crowded environments — school classrooms, military barracks, households with young children — are the classic settings for outbreaks. The incubation period is typically 2 to 5 days.
The bacterium carries an arsenal of virulence factors: surface proteins (especially the M protein) that help it evade the immune system, and toxins (streptolysins, pyrogenic exotoxins) that damage tissues and, in some infections, trigger a severe whole-body inflammatory response. The great majority of GAS infections are superficial, but the same organism that causes a routine sore throat can occasionally — usually through a break in the skin or by producing especially potent toxins — cause devastating invasive disease.
Strep Throat — Symptoms and Diagnosis
Strep throat (streptococcal pharyngitis) is the most common GAS illness. It is estimated to account for 20–30% of sore throats in children and about 5–15% in adults. Classic features include:
- Sudden onset of a severe sore throat, typically peaking within a day.
- Fever (often above 38.3°C / 101°F) and chills.
- Swollen, tender lymph nodes in the front of the neck.
- Red, inflamed tonsils, often with white patches or pus (tonsillar exudate).
- Absence of cough, runny nose, or hoarseness — these symptoms strongly suggest a viral cause instead.
- Headache, stomach ache, and nausea, especially in children.
No combination of symptoms alone can reliably diagnose strep throat, because many viruses cause identical symptoms. Testing is essential. The standard approach combines a clinical scoring tool (such as the Centor or McIsaac criteria) with laboratory testing:
- Rapid antigen detection test (RADT): A throat swab result in 5–10 minutes. Specificity is high, so a positive test confirms GAS; sensitivity is about 70–90%, so a negative result in a child with high clinical suspicion should be followed by a culture.
- Throat culture: The gold standard — virtually 100% sensitive, but takes 24–48 hours. Still recommended for children with a negative RADT when clinical suspicion is high, because missed strep in children carries rheumatic fever risk.
Adults with a negative RADT generally do not need a culture, because rheumatic fever after GAS is very rare in adults in high-income countries.
Scarlet Fever
Scarlet fever is a form of strep throat (or, less commonly, a strep skin infection) complicated by a distinctive rash. It occurs when the infecting GAS strain produces pyrogenic exotoxins (also called erythrogenic toxins) — protein toxins that cause the characteristic skin rash and contribute to the fever. The rash itself is not dangerous, but it signals that the GAS infection is more toxin-producing and underscores the importance of antibiotic treatment.
The rash typically appears 1–2 days after the sore throat begins as a fine, red, sandpaper-like eruption on the neck and chest, spreading to the body and limbs but sparing the face (though the face becomes flushed, with a pale area around the mouth — the classic circumoral pallor). The tongue initially has a white coating but then sheds it to become the distinctive "strawberry tongue" — bright red and bumpy. The rash fades over about a week, and the skin may peel in the following weeks, particularly on the hands and feet.
Scarlet fever is treated identically to strep throat: a full course of penicillin or amoxicillin. Once common and feared, it remains prevalent worldwide, and there have been cycles of resurgence — including a notable rise in several countries in the 2010s whose cause is still being studied.
Impetigo and Skin Infections
GAS causes several skin infections in addition to the throat. Impetigo is the most common — a superficial, highly contagious skin infection seen mainly in children, typically on the face, arms, and legs. There are two forms:
- Non-bullous (crusted) impetigo: Red sores that quickly break open, ooze fluid, and then dry to form a distinctive honey-colored crust. GAS is a primary cause, sometimes together with Staphylococcus aureus.
- Bullous impetigo: Larger, fluid-filled blisters; almost always caused by Staphylococcus aureus rather than GAS.
Impetigo spreads by direct contact with the sores or by touching surfaces contaminated by the fluid. Good handwashing and not sharing towels or sports equipment limit spread. Treatment is with topical antibiotics (mupirocin) for mild cases, or oral antibiotics for widespread disease.
GAS also causes cellulitis (a deeper skin and soft-tissue infection causing redness, warmth, swelling, and pain) and erysipelas (a distinct form of skin infection with a sharply defined, raised, bright-red border, commonly on the face or lower leg). Both are treated with penicillin-class antibiotics.
Invasive Disease — Necrotizing Fasciitis and Toxic Shock
A small fraction of GAS infections become invasive, meaning the bacteria breach normal tissue barriers and spread into deeper tissues or the bloodstream. These are medical emergencies with high mortality even with aggressive treatment. The two most feared forms are:
- Necrotizing fasciitis: Popularly known as "flesh-eating disease," this is a rapidly spreading infection that destroys the soft tissue beneath the skin, traveling along the fascial planes that separate muscle groups. It can follow a seemingly minor wound, insect bite, or even a chickenpox sore. The hallmarks are pain dramatically out of proportion to the visible injury, skin that may initially look deceptively normal, followed by rapidly spreading swelling and discoloration. Immediate surgical removal of infected tissue (often extensive) combined with high-dose intravenous antibiotics is the only treatment. Delays measured in hours worsen survival.
- Streptococcal toxic shock syndrome (STSS): Caused by GAS strains that produce superantigen pyrogenic exotoxins, which flood the immune system with an uncontrolled T-cell and cytokine response. This causes a sudden drop in blood pressure (shock), organ failure, and high fever. STSS can occur alongside necrotizing fasciitis or even without obvious skin involvement. It is treated with intensive care, high-dose penicillin and clindamycin (clindamycin suppresses toxin production), and intravenous immunoglobulin in severe cases.
Risk factors for invasive GAS include skin breaks (surgical wounds, burns, chickenpox), immunosuppression, intravenous drug use, and — rarely — no identifiable portal of entry. The incidence of invasive GAS has fluctuated and rose notably in some countries after 2022, a pattern being actively studied.
Rheumatic Fever and Heart Damage
Acute rheumatic fever (ARF) is not an infection — it is the immune system's misdirected response to an untreated GAS throat infection. Roughly 2–3 weeks after a strep throat, the immune system, which has been producing antibodies against the M protein on GAS's surface, begins attacking its own tissues. This is called molecular mimicry: the GAS M protein shares structural similarities with proteins in human heart valves, brain, joints, and skin, and the antibodies cannot tell the difference.
The result is widespread inflammation that can affect:
- Joints (arthritis): migratory polyarthritis — painful swelling that moves from joint to joint — is the most common feature of ARF, seen in about 75% of patients.
- Heart (carditis): Inflammation of the heart, including the valves (endocarditis), heart muscle (myocarditis), and the sac around the heart (pericarditis). This is the most dangerous aspect of ARF — repeated or severe episodes can cause permanent scarring and thickening of the mitral and aortic valves, a condition called rheumatic heart disease (RHD).
- Brain (Sydenham's chorea): Involuntary, jerky movements of the arms, legs, or face, and emotional lability. It is unusual but can be the presenting sign weeks after the initial infection.
- Skin: Subcutaneous nodules and a distinctive rash called erythema marginatum (a lacy, migrating red rash on the trunk).
The key insight is that ARF follows strep throat infections, not skin infections. GAS skin infections do not trigger rheumatic fever. This distinction matters: it means that prompt antibiotic treatment of strep throat — within 9 days of symptom onset — reliably prevents the first episode of ARF. And because the risk of ARF rises dramatically with each new strep infection, people who have already had ARF receive ongoing low-dose penicillin (secondary prophylaxis) for years to prevent recurrence and further valve damage.
Rheumatic heart disease remains a major global health problem, particularly in sub-Saharan Africa, South and Southeast Asia, and Indigenous communities in Australia and New Zealand. It is estimated to affect more than 40 million people worldwide and is a leading cause of heart surgery in young people in endemic regions.
Treatment
Streptococcus pyogenes has never developed resistance to penicillin — one of the few bacteria for which that remains true, more than 80 years after penicillin was introduced. First-line treatment for strep throat, scarlet fever, and uncomplicated skin infections remains penicillin or amoxicillin for 10 days. The full 10-day course matters: shorter courses have higher rates of treatment failure and increase the risk of rheumatic fever.
- Penicillin V (oral, twice or three times daily for 10 days) or a single injection of benzathine penicillin G are the standard first-line regimens. The injection is especially useful when adherence to a 10-day oral course is uncertain.
- Amoxicillin once or twice daily for 10 days is equally effective and often preferred for children (it tastes better and has a convenient once-daily dosing option).
- For patients who are allergic to penicillin: a narrow-spectrum cephalosporin (if the allergy is not anaphylactic), azithromycin, or clindamycin are acceptable alternatives. Azithromycin resistance in GAS has been rising in some regions.
For invasive infections (necrotizing fasciitis, STSS), high-dose intravenous penicillin G combined with clindamycin is the standard regimen. Clindamycin is added because it suppresses toxin production at the ribosomal level, even in large bacterial loads where penicillin (a cell-wall agent) is less effective against stationary-phase bacteria. Intravenous immunoglobulin (IVIG) is used as an adjunct in STSS. Surgical debridement is central to managing necrotizing fasciitis and cannot be replaced by antibiotics alone.
Do not use antibiotics for viral sore throats. Because viruses cause the majority of sore throats, testing before prescribing matters both for individual care and for protecting the community from antibiotic resistance.
Research Papers
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):e86–e102. doi:10.1093/cid/cis629 — The authoritative IDSA clinical guideline covering who to test, how to test, and how to treat GAS pharyngitis, including antibiotic choice and duration.
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685–694. doi:10.1016/S1473-3099(05)70267-X — Estimated more than 517,000 deaths annually from severe GAS diseases, highlighting rheumatic heart disease as the dominant source of GAS-attributable mortality worldwide.
- Walker MJ, Barnett TC, McArthur JD, et al. Disease Manifestations and Pathogenic Mechanisms of Group A Streptococcus. Clin Microbiol Rev. 2014;27(2):264–301. doi:10.1128/CMR.00101-13 — A comprehensive review of GAS virulence factors (M protein, exotoxins, streptolysin, hyaluronidase) and how they produce the full spectrum of GAS diseases from pharyngitis to necrotizing fasciitis.
- Ralph AP, Carapetis JR. Group A streptococcal diseases and their global burden. Curr Top Microbiol Immunol. 2013;368:1–27. doi:10.1007/82_2012_280 — Detailed epidemiology of all major GAS disease categories, including the disproportionate impact on children and populations in low- and middle-income countries.
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990–2015. N Engl J Med. 2017;377(8):713–722. doi:10.1056/NEJMoa1603693 — Global burden analysis estimating 33.4 million prevalent cases of rheumatic heart disease in 2015, with 319,000 deaths, underscoring the ongoing scale of untreated strep throat's consequences.
Connections
- Infectious Disease
- ENT Conditions
- Rheumatology Conditions
- Cardiology Conditions
- Dermatology Conditions
- All Conditions
- Strep Throat — the clinical illness this bacterium causes, with testing and treatment.