Strep Diagnosis: Rapid Antigen Tests and Throat Culture
Getting a sore throat diagnosed accurately matters more than most people realize. Take antibiotics when you don't need them and you add to antibiotic resistance, disrupt your gut, and may still feel sick for days because the real culprit — a virus — doesn't respond to penicillin. Miss a true strep infection in a child and you risk rheumatic fever, a complication that can permanently damage the heart. This page explains exactly how doctors decide whether to test you, which test they use, what the numbers mean, and how to make sense of your result.
- When to Test vs. When to Treat Empirically
- How the Rapid Antigen Test Works
- Throat Culture: The Gold Standard
- Molecular Tests and PCR
- ASO Titer and Anti-DNase B
- Blood Cultures for Invasive Disease
- Avoiding Unnecessary Testing
- Interpreting Results with Clinical Context
- Key Research Papers
- Connections
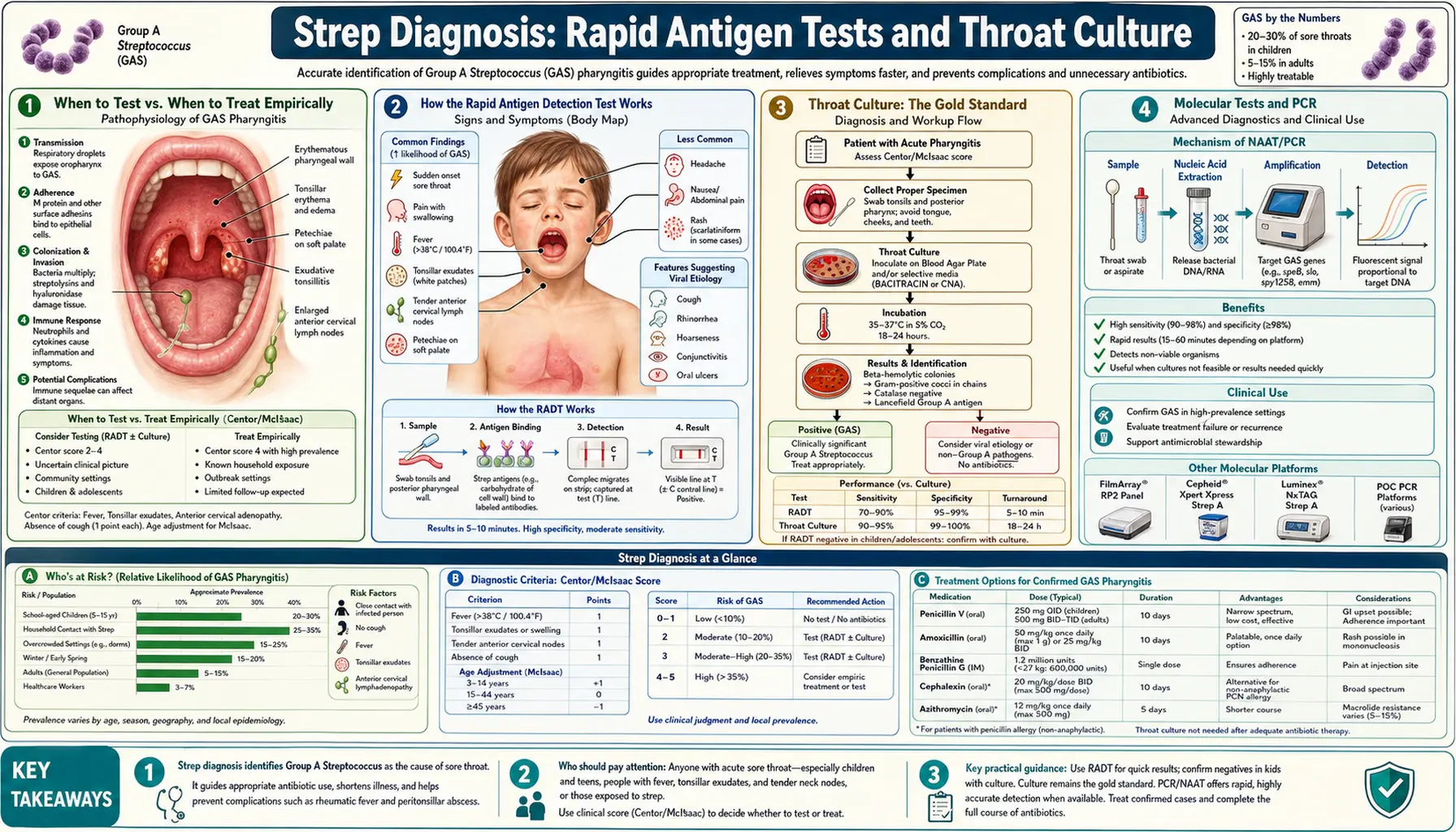
When to Test vs. When to Treat Empirically
Not everyone with a sore throat needs a strep test. Doctors use a clinical scoring system — the Centor score, later updated by McIsaac — to estimate the probability that group A Streptococcus (GAS) is actually causing the pharyngitis before deciding whether to test at all.
The four classic Centor criteria each earn one point:
- Tonsillar exudate (white patches or pus on the tonsils)
- Tender, swollen lymph nodes in the front of the neck
- Fever (temperature above 38°C / 100.4°F)
- Absence of cough
McIsaac added a fifth adjustment: add one point for age 3–14, subtract one point for age 45 and over. The reason for the age adjustment is that strep pharyngitis is predominantly a disease of school-age children. Adults over 45 almost never get it.
What the score means in practice:
- Score 0–1: GAS probability is under 10%. Testing is not recommended. The illness is almost certainly viral, and antibiotics will not help.
- Score 2–3: Probability 15–35%. This is the gray zone where testing makes the most sense. A rapid strep test helps separate the real cases from the viral ones.
- Score 4–5: Probability can reach 50–60%. Some guidelines support empiric treatment without a test in this range, though testing first is still prudent in most settings because even a score of 5 leaves a meaningful chance the illness is viral.
The key principle endorsed by the Infectious Diseases Society of America (IDSA) is test-and-treat: use a rapid test to confirm before prescribing, rather than giving antibiotics to everyone with a sore throat. This approach reduces unnecessary antibiotic prescriptions by roughly half in primary care settings without missing clinically important GAS infections.
How the Rapid Antigen Detection Test Works
The rapid antigen detection test (RADT), commonly called the "rapid strep test," is the workhorse of outpatient strep diagnosis. Results come back in 5 to 10 minutes, which is why it replaced the culture as the first-line test in most clinics and urgent care settings.
The science behind it: GAS bacteria have a unique carbohydrate antigen in their cell wall — the group A carbohydrate (rhamnose-N-acetylglucosamine). The RADT uses antibodies that bind specifically to this antigen. When you swab a throat with GAS present, those bacteria transfer to the swab. The swab is inserted into a solution that extracts the antigen, which then runs along a nitrocellulose strip. If GAS antigen is present, it forms a visible colored line — a lateral flow immunoassay, exactly the same technology used in home pregnancy tests and COVID rapid tests.
Accuracy numbers that matter:
- Specificity: 95–99%. This is excellent. A positive result almost always means GAS is genuinely present. False positives are rare.
- Sensitivity: 70–90%. This is the limitation. A negative result does not rule out strep with certainty. Roughly 1 in 10 to 3 in 10 true GAS infections will test negative on RADT.
Why sensitivity varies so much: swab technique. The single biggest factor in whether a RADT catches a real infection is how the throat is swabbed. The swab must firmly contact both tonsils (or the tonsillar fossae if tonsils have been removed) and the posterior pharynx. Touching only the front of the mouth, or only the tongue, consistently produces false negatives. Studies show that inadequate swabbing technique can reduce sensitivity by 15–20 percentage points. If a test comes back negative but your symptoms are textbook strep, it is worth asking whether the swab reached the back of your throat.
Self-test kits: Over-the-counter RADT kits now exist for home use. Their accuracy is similar to clinic-administered tests when used correctly. The challenge is swabbing your own posterior pharynx without gagging, which makes false negatives more likely at home.
Throat Culture: The Gold Standard
A throat culture involves swabbing the tonsils and posterior pharynx, then plating the sample on blood agar — a growth medium in which GAS produces distinctive clear zones called beta-hemolysis. After 24 to 48 hours of incubation, a positive culture confirms GAS infection with 95–99% sensitivity. That is as close to definitive as microbiology gets for this pathogen.
Why it takes 24–48 hours: Bacteria need time to grow into visible colonies. There is no shortcut; the biology sets the timeline. Some labs offer preliminary reads at 24 hours and final reads at 48 hours.
When backup culture is recommended after a negative RADT: This is one of the most practically important questions in strep management, and the answer differs by age:
- Children and adolescents: A negative RADT should be followed by a throat culture. The reason is rheumatic fever risk. Acute rheumatic fever (ARF) is a serious complication of untreated strep pharyngitis that can permanently damage heart valves. Children are the primary at-risk population. Because RADT sensitivity is not perfect, missing a real infection in a child carries meaningful consequences.
- Adults in high-income countries: Most guidelines, including IDSA 2012, do not routinely recommend backup culture for adults after a negative RADT. ARF is exceedingly rare in adults in high-income settings (incidence below 1 per 100,000 per year), and the cost and delay of universal backup culture is not justified by the risk reduction.
- Exception — adults in high-risk settings: Military recruits, adults in closed communities, people with personal or family history of ARF, and travelers returning from regions with high ARF prevalence should be treated more like children, with backup culture after negative RADT.
Cost and access: Throat cultures typically cost $20–$60 before insurance. Results may arrive via patient portal or phone call the next day. If you are prescribed antibiotics pending culture results, ask your provider whether to continue treatment if the culture returns negative.
Molecular Tests and PCR
Nucleic acid amplification tests (NAATs), including PCR, detect GAS DNA rather than the bacterial protein antigen. They are newer than RADT and culture and represent a significant upgrade in sensitivity without sacrificing specificity.
Performance: NAATs achieve sensitivity of 97–99% and specificity of 97–99% — substantially better than RADT in head-to-head comparisons. They detect even very small amounts of GAS DNA, catching infections that would be missed by RADT.
Speed: Depending on the platform, results come back in 1–2 hours in the clinic, or within the same visit on some newer point-of-care molecular systems. Centralized lab-based NAATs may take longer if samples are batched.
When NAATs add value:
- Children with a negative RADT but high clinical suspicion, where a NAAT could replace the overnight wait for culture
- Immunocompromised patients in whom missing strep carries higher risk
- Outbreak investigations where maximizing sensitivity matters for public health tracking
- Settings where backup culture is logistically difficult
The carrier state problem: Like culture, NAATs detect GAS presence but cannot tell you whether the bacteria are actively causing disease or simply colonizing the throat. A person can carry GAS asymptomatically — the so-called carrier state — and test positive without having clinical strep pharyngitis. This matters most when a school-age child keeps testing positive despite repeated antibiotic courses: the positive result may reflect persistent colonization rather than recurrent infection.
Cost and availability: NAATs for GAS are not universally available in primary care and urgent care settings, though availability is expanding. They are more common in hospital emergency departments and pediatric practices. Cost is higher than RADT but similar to culture in many insurance contexts.
ASO Titer and Anti-DNase B
The anti-streptolysin O (ASO) titer is a blood test, not a throat swab. It measures antibodies your immune system made in response to streptolysin O — a toxin released by GAS bacteria during infection. Because it detects the immune response rather than the bacteria themselves, it tells you about past infection, not current active disease.
What it is used for: ASO titer is ordered when doctors suspect complications of recent strep infection that happened weeks ago and was never diagnosed — specifically:
- Acute rheumatic fever (ARF): A child presents with joint inflammation, heart murmur, or other ARF features. The throat infection that triggered this was 2–4 weeks earlier and has since resolved. An elevated ASO confirms recent GAS exposure, supporting the ARF diagnosis.
- Post-streptococcal glomerulonephritis (PSGN): A kidney complication appearing 1–3 weeks after strep infection. ASO can confirm the preceding strep episode.
Timing matters: ASO levels start rising about 1 week after GAS infection, peak at 3–5 weeks, and then gradually decline over months. Testing during the acute sore throat phase often shows a normal titer even with true GAS infection, because the immune response has not had time to develop. This is why ASO is not a useful test for diagnosing acute pharyngitis.
Important limitation for skin infections and PSGN: GAS can cause skin infections (impetigo, cellulitis) as well as throat infections, and either can trigger PSGN. However, ASO rises poorly after GAS skin infections — the skin environment suppresses the streptolysin O response. If evaluating PSGN after a skin infection, anti-DNase B antibody is the more reliable marker. Anti-DNase B rises after both throat and skin GAS infections and persists longer in the circulation, making it the preferred serological test in this context.
Normal ranges: Normal ASO titers vary by laboratory and age. Children typically have higher background titers because they are exposed to strep more frequently. A result above 200 IU/mL in adults or 333 IU/mL in children is generally considered elevated, but confirm with your lab's specific reference range.
Blood Cultures for Invasive Disease
When GAS escapes the throat or skin and enters the bloodstream — invasive group A streptococcal disease — the diagnostic approach shifts entirely. You are no longer looking for bacteria in the throat; you are looking for bacteria in places they should never be.
Blood cultures: Two sets of blood cultures (from two separate venipuncture sites) should be drawn before antibiotics are started in any patient who appears severely ill with suspected invasive GAS. GAS is a good bacteremic pathogen — blood cultures are positive in a meaningful proportion of invasive cases. Starting antibiotics first dramatically reduces culture yield, which can delay pathogen identification and targeted therapy.
Wound and tissue cultures: In necrotizing fasciitis (NF) or myositis, tissue cultures obtained at the time of surgical debridement are essential. These often grow GAS in pure culture. Superficial wound swabs are unreliable and not recommended for diagnosis of deep tissue infections.
Supporting labs that guide severity assessment:
- C-reactive protein (CRP): Markedly elevated in invasive GAS (often >200 mg/L). Helps distinguish serious bacterial infection from viral illness.
- White blood cell count (WBC): Elevated with left shift (immature neutrophils) suggests serious bacterial infection. Very high counts (>20,000) or paradoxically low counts may indicate overwhelming sepsis.
- Lactate: Elevated serum lactate (>2 mmol/L) is a marker of tissue hypoperfusion and signals streptococcal toxic shock syndrome (STSS) or septic shock requiring ICU-level care.
- Creatinine and LFTs: Organ function markers to assess multi-organ involvement in STSS.
- Imaging: CT of the affected limb or body area for NF — the classic finding is gas tracking along fascial planes. MRI is more sensitive but may not be available urgently. Neither replaces surgical exploration when NF is clinically suspected.
Invasive GAS disease is a medical emergency. Diagnostic workup runs in parallel with resuscitation and empiric antibiotic therapy — you do not delay antibiotics waiting for culture results, but you draw cultures before the first antibiotic dose whenever possible.
Avoiding Unnecessary Testing
About 80–90% of sore throats are caused by viruses. Testing everyone with a sore throat for strep would generate enormous numbers of unnecessary positives from the carrier state, lead to inappropriate antibiotic prescribing, and consume healthcare resources without improving outcomes. Understanding when not to test is as important as knowing when to test.
Symptoms that strongly suggest a viral cause:
- Runny nose (rhinorrhea)
- Cough
- Conjunctivitis (red, watery eyes)
- Hoarseness
- Mouth sores or ulcers
- Diarrhea
When these features are present, the Centor/McIsaac score will typically be 0–1. Testing in this context has a high rate of positive results that represent colonization rather than infection, leading to unnecessary antibiotic courses.
The carrier state problem in detail: Between 10–15% of school-age children carry GAS in their throats at any given time without having active infection. A child who is a carrier will test positive on RADT every time they swab positive — but they are not ill from GAS, they do not need antibiotics, and treating them will not clear the carriage. The distinguishing feature is that carriers do not have the acute inflammation, fever, and swollen lymph nodes of true strep pharyngitis. Positive RADT in a child with cough, runny nose, and mild sore throat does not always mean treatment is needed.
The antibiotic resistance argument: Unnecessary antibiotic prescriptions for viral sore throats are a recognized driver of antibiotic resistance. Streptococcus pyogenes itself has shown increasing macrolide resistance in many countries (up to 30–40% resistance to erythromycin and azithromycin in some regions), driven in part by overuse of these antibiotics. Penicillin resistance in GAS remains essentially zero worldwide — but only because we use it judiciously.
What happens if you don't treat true strep: Most adults with untreated GAS pharyngitis recover fully without complications. The acute illness is self-limiting in 3–7 days. The real reason to treat is to prevent ARF in susceptible individuals (mainly children), shorten symptom duration by about 1–2 days, and reduce transmission. Antibiotics do not prevent post-streptococcal glomerulonephritis.
Interpreting Results with Clinical Context
Test results are not self-interpreting. A positive RADT is not the same as a treatment mandate, and a negative RADT does not guarantee no strep. Clinical context determines what the result actually means for you.
Scenario 1: Child, age 8, fever 39°C, tonsillar exudate, no cough — RADT positive. This is straightforward. Classic presentation plus positive RADT. GAS pharyngitis is confirmed. Start a 10-day course of penicillin V or amoxicillin.
Scenario 2: Adult, age 32, sore throat, cough, runny nose — RADT positive. This requires more thought. The presence of cough and runny nose strongly suggests a viral URI, with perhaps coincidental GAS colonization. The positive RADT may reflect the carrier state. Most guidelines would support watchful waiting in this adult rather than immediate antibiotic treatment, particularly if fever is low-grade or absent. A shared decision-making conversation with your provider is appropriate here.
Scenario 3: Child, age 10, Centor score 3 — RADT negative. Do not stop here. RADT sensitivity is 70–90%. A backup throat culture is recommended. In a child with moderate-to-high clinical suspicion and a negative rapid test, the culture catches the cases rapid testing misses.
Scenario 4: Adult, age 50, mild sore throat, score 0-1 — no test ordered. Correct clinical decision. No testing is warranted. Supportive care (salt water gargle, lozenges, ibuprofen or acetaminophen for pain, rest, fluids) is the right approach. Antibiotics will not help.
Scenario 5: Repeated positive tests despite multiple antibiotic courses. Consider the carrier state. If a child tests positive for strep repeatedly but lacks acute illness markers each time, they may be a colonized carrier who keeps getting exposed to viral pharyngitis in the school environment. Management of chronic carriers is complex and rarely requires eradication therapy in the absence of ARF risk factors.
Practical takeaways for patients:
- Ask your provider why they are or are not testing — knowing the reasoning helps you participate in the decision.
- If you have a positive RADT, ask whether your symptoms are consistent with active infection or possible carrier state.
- If your child has a negative RADT but still has classic strep symptoms, ask about a backup culture.
- Finish the full antibiotic course even if you feel better in 2–3 days. Stopping early is one reason strep can linger or recur.
- A negative test with a viral illness is good news, not bad news — it means antibiotics were never going to help.
Key Research Papers
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):e86–e102 — Search PubMed — The definitive IDSA guideline establishing test-and-treat strategy, RADT role, and backup culture recommendations by age.
- Bisno AL, Gerber MA, Gwaltney JM, Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2002;35(2):113–125 — Search PubMed — Earlier IDSA guideline establishing the foundational framework for GAS pharyngitis management.
- McIsaac WJ, White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158(1):75–83 — Search PubMed — Original paper describing the McIsaac modification to the Centor score, adding age adjustment and validating its use to guide testing decisions.
- Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1(3):239–246 — Search PubMed — The seminal 1981 paper establishing the four original Centor criteria that underpin all subsequent clinical decision rules for strep pharyngitis.
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172(11):847–852 — Search PubMed — Large population validation confirming the predictive accuracy of both scoring systems across age groups in a real-world clinical setting.
- Pelucchi C, Grigoryan L, Galeone C, et al. Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18(Suppl 1):1–27 — Search PubMed — European guideline synthesizing evidence on sore throat management, including RADT accuracy and antibiotic stewardship in European settings.
- Lean WL, Arnup S, Danchin M, Steer AC. Rapid diagnostic tests for group A streptococcal pharyngitis: a meta-analysis. Pediatrics. 2014;134(4):771–781 — Search PubMed — Systematic review and meta-analysis of RADT accuracy across studies, confirming pooled sensitivity ~86% and specificity ~96% in pediatric populations.
- Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev. 2004;17(3):571–580 — Search PubMed — Review addressing throat swab technique, RADT mechanics, and the clinical implications of sensitivity gaps between rapid tests and culture.
- Choby BA. Diagnosis and treatment of streptococcal pharyngitis. Am Fam Physician. 2009;79(5):383–390 — Search PubMed — Practical primary care review covering Centor scoring, RADT use, culture indications, and treatment selection for family physicians.
- Oppegaard O, Skrede S, Mylvaganam H, Kittang BR. Emerging threat of antimicrobial resistance in beta-hemolytic streptococci. Front Microbiol. 2017;8:1997 — Search PubMed — Covers serological markers (ASO, anti-DNase B) for post-streptococcal syndromes alongside emerging antibiotic resistance patterns in GAS.
- Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229–241 — Search PubMed — Documents the contribution of unnecessary sore throat antibiotic prescriptions to macrolide resistance in GAS and proposes diagnostic stewardship as the primary intervention.
Additional PubMed searches relevant to this topic:
- Rapid antigen detection test group A streptococcus
- Throat culture streptococcal pharyngitis sensitivity
- Centor McIsaac score pharyngitis validation
- ASO titer anti-streptolysin rheumatic fever
- GAS carrier state pharyngitis overtreatment
Connections
- All Bacteria
- Streptococcus Pyogenes Overview
- Strep Symptoms & Diagnosis Hub
- Strep Throat and Pharyngitis
- Penicillin and Antibiotic Treatment
- Lab Tests