Rheumatic Fever and Post-Strep Complications
- What Is Acute Rheumatic Fever?
- Jones Criteria: How ARF Is Diagnosed
- Carditis and Rheumatic Heart Disease
- Polyarthritis: The Migratory Joint Attack
- Sydenham's Chorea and PANDAS
- Post-Streptococcal Glomerulonephritis
- Preventing Acute Rheumatic Fever
- Managing Rheumatic Heart Disease
- Key Research Papers
- Connections
What Is Acute Rheumatic Fever?
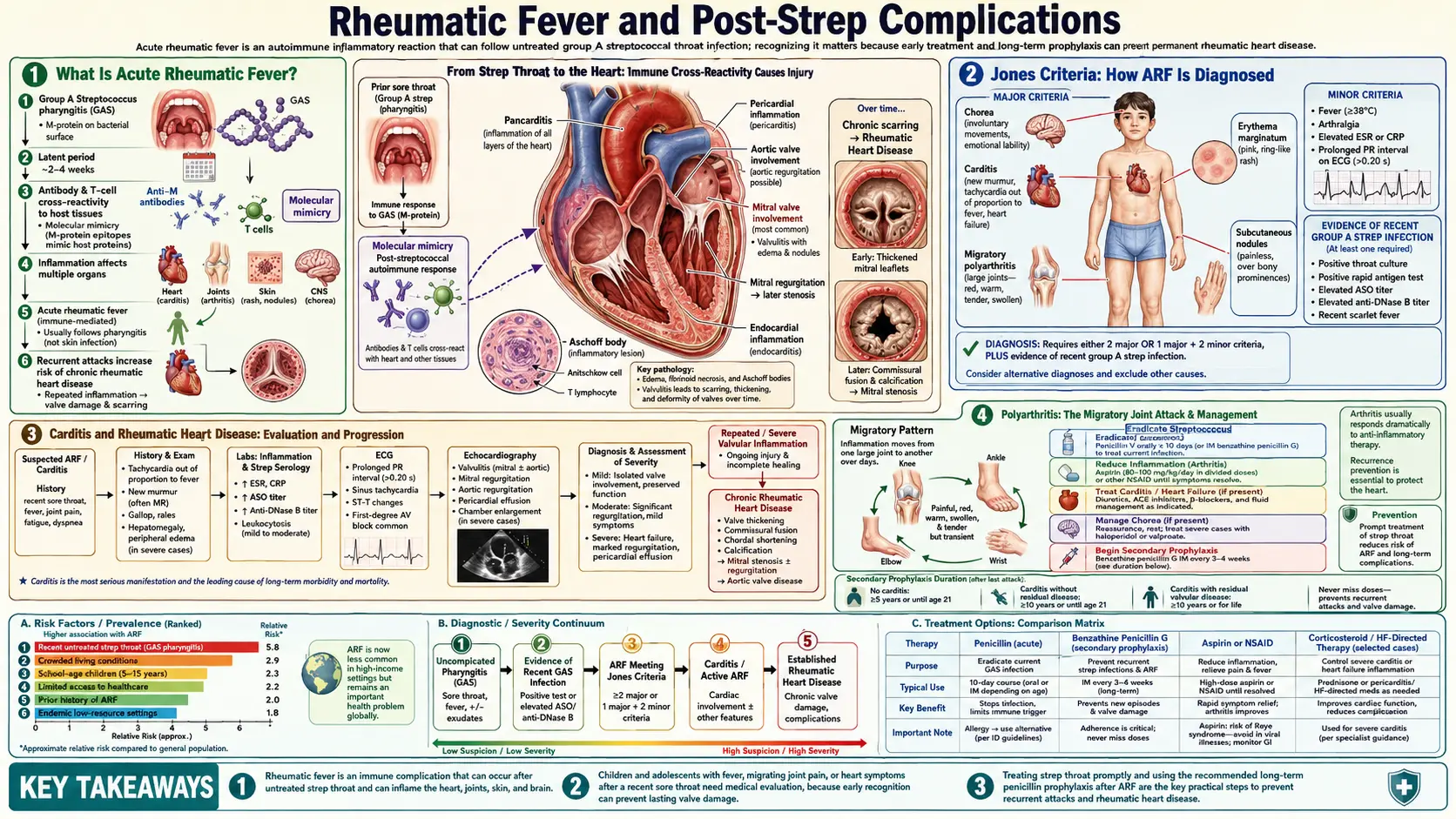
Acute rheumatic fever (ARF) is not an infection. Your doctor cannot swab your throat and find it. By the time ARF starts — typically two to four weeks after an untreated strep throat — the Streptococcus pyogenes bacteria are long gone. What remains is your own immune system, still fighting at full intensity, now attacking the wrong targets.
The mechanism is called molecular mimicry. The surface proteins on Group A Streptococcus (GAS) — particularly the M protein — are structurally similar to proteins found in human heart valve tissue, joint membranes, and certain regions of the brain. When your immune system builds antibodies to fight the strep infection, those antibodies cannot reliably tell the difference between GAS proteins and your own tissues. The antibodies and T-cells that were supposed to eliminate bacteria begin attacking your heart, joints, and nervous system instead.
This misdirected immune attack is why ARF is classified as an autoimmune disease rather than an infectious one. It is also why antibiotics do not treat an established case of ARF — the bacteria are already gone. Treatment focuses on managing the inflammation and preventing the next strep episode that would trigger another round of damage.
One critical and often misunderstood fact: only throat infections with GAS cause ARF. GAS skin infections (impetigo, wound infections) trigger a different post-streptococcal complication — kidney disease — but not rheumatic fever. The reason involves differences in which GAS strains cause throat versus skin infections, and differences in the immune response at those two sites. This distinction matters enormously for prevention strategies, because preventing ARF means specifically targeting throat infections.
The populations hit hardest by ARF are children aged 5 to 15 living in crowded, lower-income settings where strep throat circulates frequently and access to antibiotics is limited. Australia's Aboriginal and Torres Strait Islander communities, parts of sub-Saharan Africa, South Asia, and the Pacific Islands have some of the highest rates in the world. But ARF is not purely a disease of poverty — outbreaks have occurred in US military camps and schools under crowded conditions.
Jones Criteria: How ARF Is Diagnosed
There is no single test that says "this person has ARF." Instead, doctors use a diagnostic framework called the Jones Criteria, first developed in 1944 and updated most recently by the American Heart Association in 2015. The criteria divide findings into major and minor categories based on how specifically they point to ARF versus other conditions.
Major criteria:
- Carditis — inflammation of the heart, detected as a new murmur, abnormal echocardiogram, or signs of pericarditis. The 2015 update added subclinical carditis visible on echo even when no murmur is audible.
- Polyarthritis — inflammation of multiple joints simultaneously, especially large joints. The classic migratory pattern (moving from joint to joint over days) is very characteristic.
- Chorea — involuntary, purposeless jerky movements (Sydenham's chorea), which may appear weeks after the strep infection.
- Erythema marginatum — a distinctive skin rash with a spreading pink ring that has a pale center, most visible on the trunk. Rare but highly specific for ARF.
- Subcutaneous nodules — firm, painless lumps under the skin over bony prominences. Also rare but specific.
Minor criteria:
- Fever (usually above 38.5°C / 101.3°F)
- Elevated inflammatory markers: C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR)
- Prolonged PR interval on electrocardiogram (a specific change in the heart's electrical timing)
To diagnose ARF, a patient needs either 2 major criteria or 1 major + 2 minor criteria, combined with evidence of a recent GAS infection. That evidence usually comes from a positive throat culture, a rapid strep test, or elevated strep antibody levels in the blood (ASO titer or anti-DNase B), which peak about 3 to 6 weeks after the infection.
The 2015 updated Jones criteria created a two-track system: one set of thresholds for populations where ARF is rare (such as most of North America and Western Europe), and a more sensitive set for high-risk populations where the disease is common. In high-risk populations, monoarthritis (just one joint) and polyarthralgia (joint pain without visible swelling) are counted as major criteria, because missing early cases in those settings carries a steep long-term cost.
Echocardiographic carditis — where the echo shows valve abnormalities but no murmur can be heard with a stethoscope — was added to the major criteria in 2015. Studies in endemic populations showed that many patients with what appeared to be "mild" ARF actually had significant valve changes visible on echo, meaning their disease was being systematically undercounted and undertreated.
Carditis and Rheumatic Heart Disease
Of all the complications that follow untreated strep throat, damage to the heart is the most serious. Carditis occurs in 50 to 70 percent of first ARF episodes, and it is the only part of ARF that leaves permanent damage. Everything else — the painful joints, the jerky movements, the skin findings — heals completely. The heart does not.
During acute carditis, all three layers of the heart can be inflamed: the endocardium (inner lining), myocardium (muscle), and pericardium (outer sac). But the endocardium is where the lasting damage happens. The mitral valve — between the left atrium and left ventricle — is affected most commonly, followed by the aortic valve. The right-sided valves (tricuspid, pulmonic) are rarely involved.
In the acute phase, the inflamed valve leaflets swell and may not close properly, causing blood to leak backward — a condition called mitral regurgitation. At this stage, the heart muscle can usually compensate, and many patients feel only fatigue or shortness of breath during exertion. Some have no symptoms at all, especially children whose hearts are resilient and adaptable.
The long-term problem is what happens over years and decades as scar tissue forms where inflammation once raged. Repeated ARF episodes — each one triggered by another untreated strep throat — pile more scar tissue onto valves that already have damage. The leaflets thicken and fuse, eventually narrowing the valve opening. This narrowing, called mitral stenosis, develops gradually, typically becoming clinically significant 10 to 20 years after the initial ARF episode. By then, the person may be in their 20s or 30s — a working adult, possibly pregnant — suddenly developing severe breathlessness, heart failure, or atrial fibrillation.
The global burden is staggering. More than 40 million people worldwide currently live with rheumatic heart disease (RHD), and approximately 300,000 die from it each year. RHD is the single leading cause of acquired heart disease in children and young adults globally — surpassing ischemic heart disease in that age group. The tragedy is that virtually every case of RHD is preventable by treating strep throat with a 10-day course of penicillin.
Countries where ARF and RHD remain common include many nations in sub-Saharan Africa, South and Southeast Asia, the Pacific Islands, and Oceania — particularly among Indigenous communities in Australia and New Zealand. In these settings, a child who develops ARF at age 8 may need heart valve surgery by age 25 if secondary prophylaxis is not maintained. Surgery in resource-limited settings carries its own mortality risks, and prosthetic valve replacements require lifelong anticoagulation that is difficult to manage without reliable laboratory monitoring.
Polyarthritis: The Migratory Joint Attack
Joint involvement is the most common manifestation of ARF, affecting roughly 75 percent of patients. The pattern is distinctive enough that recognizing it quickly can lead to an early diagnosis — and early treatment that prevents cardiac damage from progressing.
The arthritis of ARF is described as migratory polyarthritis. It affects multiple large joints — typically knees, ankles, elbows, and wrists — but rather than attacking all of them simultaneously, it appears to move. A knee may be exquisitely painful and swollen for one or two days, then improve as the ankle or elbow suddenly becomes inflamed. This migratory quality distinguishes ARF from rheumatoid arthritis (which tends to be symmetric and persistent) and from septic arthritis (which infects one joint at a time and does not migrate).
The pain in ARF arthritis is often described as severe and out of proportion to the swelling visible on examination. Patients may be unable to bear weight on an affected knee even when it looks only mildly swollen. Touching the joint or moving it passively can cause intense discomfort.
One of the most diagnostically useful features is how dramatically the arthritis responds to aspirin or anti-inflammatory medications. In true ARF polyarthritis, joint pain typically improves noticeably within 24 to 48 hours of starting aspirin at an adequate dose. A dramatic, rapid response is actually considered a supporting diagnostic feature. Rheumatologists sometimes call this the "aspirin test" — not an official diagnostic criterion, but practically useful when other features are ambiguous.
Critically, the arthritis of ARF does not cause permanent joint damage. Even in untreated cases, the joints eventually heal completely without erosions, deformity, or long-term disability. This stands in complete contrast to rheumatoid arthritis or gout, which progressively erode joint surfaces. The joint involvement in ARF is painful and debilitating in the short term but leaves no lasting structural harm. The heart is not so fortunate.
In some high-incidence populations, particularly Aboriginal Australians, a monoarthritis variant has been documented — where only one joint is affected rather than multiple. This presentation can be missed under the classic Jones criteria designed for low-risk populations, which is one reason the 2015 AHA update specifically adjusted the thresholds for high-risk settings.
Sydenham's Chorea and PANDAS
Perhaps the most unusual and unsettling complication of strep infection is Sydenham's chorea — a neurological condition characterized by involuntary, purposeless jerky movements of the arms, legs, and face. A child with chorea may appear to be fidgeting constantly, grimacing, or dropping objects. They cannot control these movements and become distressed by them.
Chorea occurs because the same molecular mimicry that attacks heart valves also affects certain neurons in the basal ganglia — brain regions involved in movement control. The lag between infection and chorea is notably long: while polyarthritis appears within weeks of a strep throat, chorea may not emerge until two to three months after the initial infection. By the time the movements start, the connection to strep throat may not be obvious — particularly if the original throat infection was mild or went unrecognized.
The diagnostic picture for chorea is further complicated by emotional changes. Children with Sydenham's chorea often display lability — crying for no apparent reason, sudden mood swings, unusual anxiety. These behavioral changes sometimes precede the movement abnormalities and can lead to an initial psychiatric workup before the neurological cause is identified.
Chorea is generally self-limiting. Most cases resolve within three to six months without specific neurological treatment. For mild cases, supportive care — rest, reduced sensory stimulation, reassurance — is sufficient. Severe cases, where the movements significantly impair function or cause injury, are typically managed with valproate or carbamazepine. Corticosteroids are sometimes used when chorea occurs alongside severe carditis, but their independent benefit for chorea alone is less established.
A related but distinct and more controversial entity is PANDAS — Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections. Children with PANDAS develop obsessive-compulsive disorder (OCD) symptoms, tic disorders, or sudden-onset anxiety that appears or worsens abruptly after GAS infections. PANDAS differs from Sydenham's chorea in several important ways: the neuropsychiatric symptoms rather than movement abnormalities dominate; the course is often episodic (symptoms flare with each new strep exposure); and the postulated mechanism may involve antibodies targeting different neuronal populations.
PANDAS remains a subject of active scientific debate. The diagnostic criteria have been challenged as insufficiently specific — many children have strep exposures and behavioral changes without any causal relationship — and controlled trials of treatments such as plasma exchange and intravenous immunoglobulin (IVIG) have produced mixed results. The diagnosis should be made cautiously, by physicians familiar with the current evidence, and should not lead to long-term antibiotic prophylaxis without clear documentation of a GAS-triggered relapsing course.
Post-Streptococcal Glomerulonephritis
Post-streptococcal glomerulonephritis (PSGN) is a different kind of post-strep complication — one that damages the kidneys rather than the heart or joints. Like ARF, it is not an active infection but an immune-mediated response that unfolds after the bacteria are gone. Unlike ARF, it can follow GAS infections at either the throat or the skin.
The mechanism involves immune complexes — packages of GAS antigens bound to the antibodies produced against them — that deposit in the tiny filtering units of the kidneys (glomeruli). Once lodged there, these complexes trigger local inflammation that disrupts the glomeruli's ability to filter blood properly.
PSGN typically appears 10 to 21 days after a throat infection, or 3 to 6 weeks after a skin infection. The timing difference reflects the time it takes for immune complexes to form in sufficient quantity to cause kidney damage. Not all strains of GAS cause PSGN — only specific "nephritogenic" strains, historically M serotypes 12 and 49, carry the risk.
The classic presentation includes:
- Hematuria — blood in the urine, which turns it tea-colored, cola-colored, or smoky. This is usually the symptom that brings families to the doctor.
- Proteinuria — protein leaking into the urine, detectable on a simple dipstick test.
- Edema — fluid retention, most visible as puffiness around the eyes in the morning or swelling of the ankles.
- Hypertension — elevated blood pressure due to fluid retention and reduced kidney filtration.
In children, PSGN is almost always self-limiting. The immune complexes are eventually cleared, inflammation subsides, and kidney function returns to normal within weeks to months. Most children recover completely with no lasting kidney damage. Supportive care — managing blood pressure with antihypertensive medications, restricting salt and fluid intake, monitoring kidney function — is the main treatment.
Adults and older patients have a more guarded prognosis. A significant minority of adults with PSGN develop persistent proteinuria or hypertension that continues for years, and some progress toward chronic kidney disease. Elderly patients and those with underlying kidney conditions are particularly vulnerable.
A critical point that patients and families often find surprising: treating the strep infection with antibiotics does not prevent PSGN. Once a nephritogenic strain has triggered the immune response, the glomerulonephritis will follow whether or not the bacteria are eliminated. This is the opposite of ARF, where prompt antibiotic treatment of the throat infection reliably prevents rheumatic fever. The distinction is not well understood outside of medical settings and causes significant confusion.
Preventing Acute Rheumatic Fever
The prevention of ARF is one of medicine's most powerful and underutilized success stories. A series of studies in the late 1940s and 1950s — most notably the landmark trials by Lewis Wannamaker and colleagues — demonstrated that treating strep throat with penicillin within nine days of symptom onset prevents the subsequent development of ARF. Not reduces the risk modestly — prevents it, effectively completely, in compliant patients.
This finding transformed ARF from an almost inevitable complication of recurrent strep throat into a largely preventable disease. In high-income countries where strep throat is routinely treated with antibiotics, ARF has become rare. The United States went from tens of thousands of ARF cases per year in the mid-20th century to a few hundred annually today. The decline tracks almost exactly with the widespread adoption of penicillin therapy for strep throat.
The window is generous — nine full days — because the immune cascade that produces ARF takes several weeks to develop. Antibiotics given within this period can interrupt the immune sensitization process before it reaches the point of attacking host tissues. However, this window should not be taken as license for delay. Earlier treatment means shorter illness, reduced transmission to household contacts, and a larger margin against the ARF clock.
For patients who have already had one episode of ARF, the picture changes significantly. A second strep throat infection will trigger a second ARF episode with high probability, and each successive episode adds cumulative valve damage. These patients require secondary prophylaxis: long-term, ongoing antibiotic therapy to prevent future strep infections before they can cause another round of inflammation.
The standard secondary prophylaxis regimen is benzathine penicillin G given by intramuscular injection every 28 days. Monthly injections are more effective than daily oral penicillin because they eliminate the risk of missed doses — and a single missed dose leaves a window during which a strep throat could go undetected and untreated. For patients who genuinely cannot tolerate injections and are at lower risk, daily oral penicillin V or amoxicillin is an alternative.
How long secondary prophylaxis continues depends on the severity of cardiac involvement during ARF:
- No carditis during ARF: 5 years of prophylaxis, or until age 21, whichever is longer.
- Carditis with no residual valve disease: 10 years, or until age 21, whichever is longer.
- Persistent rheumatic heart disease: At least 10 years, or until age 40, whichever is longer — and sometimes lifelong, particularly for patients undergoing valve surgery or with severe disease.
Adherence to secondary prophylaxis is the single greatest challenge in ARF management worldwide. Monthly injections are painful, require clinic visits, and must continue for years in patients who often feel completely well between episodes. In high-burden settings where clinics are distant and staff are stretched, maintaining prophylaxis programs for thousands of at-risk patients is an enormous logistical undertaking — but the payoff, measured in hearts saved and surgeries avoided, is profound.
Managing Rheumatic Heart Disease
For the 40-plus million people already living with rheumatic heart disease, the goal shifts from prevention to management — slowing the progression of valve damage, treating complications, and in appropriate cases, repairing or replacing damaged valves.
Echocardiographic screening plays a central role in endemic areas. Standard clinical examination (listening with a stethoscope) misses a significant proportion of mild-to-moderate valve disease, particularly mitral regurgitation that the heart is compensating for without producing symptoms. Population-level echo screening programs in high-burden areas have repeatedly demonstrated that the true prevalence of RHD is 5 to 10 times higher than what clinical examination alone detects. Early identification through screening allows secondary prophylaxis to be started or intensified before valve damage advances to the point of requiring surgery.
Mitral regurgitation — the acute, inflammatory valve leak — may improve partially during the months following an ARF episode, especially in children who receive good anti-inflammatory treatment. Mild residual regurgitation often remains stable for years. However, severe or worsening regurgitation eventually requires intervention. The optimal timing of surgery is before the left ventricle, which has been under excessive strain, begins to permanently dilate and weaken.
Mitral stenosis — the chronic, fibrotic narrowing that develops over a decade or more — can sometimes be treated with a catheter-based procedure called percutaneous mitral balloon valvotomy (PMBV), which cracks the fused valve leaflets open without open-heart surgery. When the valve is too heavily calcified or the anatomy is too distorted for PMBV, surgical repair or mechanical valve replacement is necessary.
Atrial fibrillation is a common complication of rheumatic mitral stenosis. The enlarged, pressure-overloaded left atrium develops irregular electrical activity, and the resulting arrhythmia dramatically increases stroke risk. Anticoagulation with warfarin (or newer direct oral anticoagulants in appropriate cases) is essential once atrial fibrillation develops. Managing anticoagulation safely requires regular INR monitoring — a significant practical challenge in resource-limited settings.
Pregnancy poses special risks for women with RHD. The cardiovascular demands of pregnancy — increased blood volume, increased cardiac output, changes in heart rate — can decompensate valvular disease that was previously stable. Mitral stenosis is particularly dangerous in pregnancy. Women with known RHD who are planning pregnancy should be evaluated by a cardiologist before conception, and many require close monitoring or intervention before they can safely carry a pregnancy.
The global equity dimension of RHD management is stark. In high-income countries, patients with RHD can access echocardiography, specialized cardiology care, and cardiac surgery as routine medical services. In the countries where RHD is most prevalent — where monthly penicillin prophylaxis is often unavailable, where echo machines are rare, where cardiac surgical centers may not exist within hundreds of miles — the same patient faces a progression to heart failure and premature death that is entirely foreseeable and entirely preventable. Closing that gap is one of the central challenges in global cardiovascular health.
Key Research Papers
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med. 2017;377(8):713-722 — Search PubMed
- Cunningham MW. Streptococcus and rheumatic fever. Curr Opin Rheumatol. 2007;19(5):408-415 — Search PubMed
- Ralph AP, Carapetis JR. Group A streptococcal diseases and their global burden. Curr Top Microbiol Immunol. 2013;368:1-27 — Search PubMed
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):e86-102 — Search PubMed
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685-694 — Search PubMed
- Gewitz MH, Baltimore RS, Tani LY, et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015;131(20):1806-1818 — Search PubMed
- Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers. 2016;2:15084 — Search PubMed
- Barnett TC, Bowen AC, Carapetis JR. The fall and rise of group A streptococcus diseases. Epidemiol Infect. 2019;147:e4 — Search PubMed
- Walker MJ, Barnett TC, McArthur JD, et al. Disease manifestations and pathogenic mechanisms of group A streptococcus. Clin Microbiol Rev. 2014;27(2):264-301 — Search PubMed
- Oppegaard O, Skrede S, Mylvaganam H, Kittang BR. Emerging threat of antimicrobial resistance in beta-hemolytic streptococci. Front Microbiol. 2017;8:1989 — Search PubMed
- Swedo SE, Leckman JF, Rose NR. From research subgroup to clinical syndrome: modifying the PANDAS criteria to describe PANS (Pediatric Acute-onset Neuropsychiatric Syndrome). Pediatr Therapeut. 2012;2(2):113 — Search PubMed
Search PubMed for more:
- Acute rheumatic fever prevention
- Rheumatic heart disease global burden
- Sydenham's chorea streptococcal
- Post-streptococcal glomerulonephritis treatment
- Benzathine penicillin secondary prophylaxis rheumatic fever
Connections
- Streptococcus Pyogenes Overview
- Strep Throat and Pharyngitis
- Strep Throat (Infectious Disease)
- Prevention and Vaccine Research
- Penicillin and Antibiotic Treatment
- Cardiology Diseases
- Rheumatology Diseases
- All Bacteria