Group A Strep (GAS): Symptoms, Signs, and Diagnosis
Group A Streptococcus (GAS), or Streptococcus pyogenes, is one of the most versatile human bacterial pathogens on earth. A single species causes an extraordinary range of illnesses — from the familiar sore throat a child brings home from school to rapidly fatal necrotizing fasciitis. Understanding the full symptom spectrum helps patients and caregivers know when a sore throat is "just a sore throat," when to demand a rapid strep test, and when to go straight to the emergency room. This hub page surveys the entire clinical picture; the three sub-articles below go deep on strep throat, invasive disease, and diagnostic testing.
- What Is Group A Strep?
- Strep Throat: Classic Presentation
- Scarlet Fever
- Impetigo and Ecthyma
- Erysipelas and Cellulitis
- Invasive Disease Spectrum
- Puerperal Sepsis
- Global Burden of GAS
- Key Research Papers
- Connections
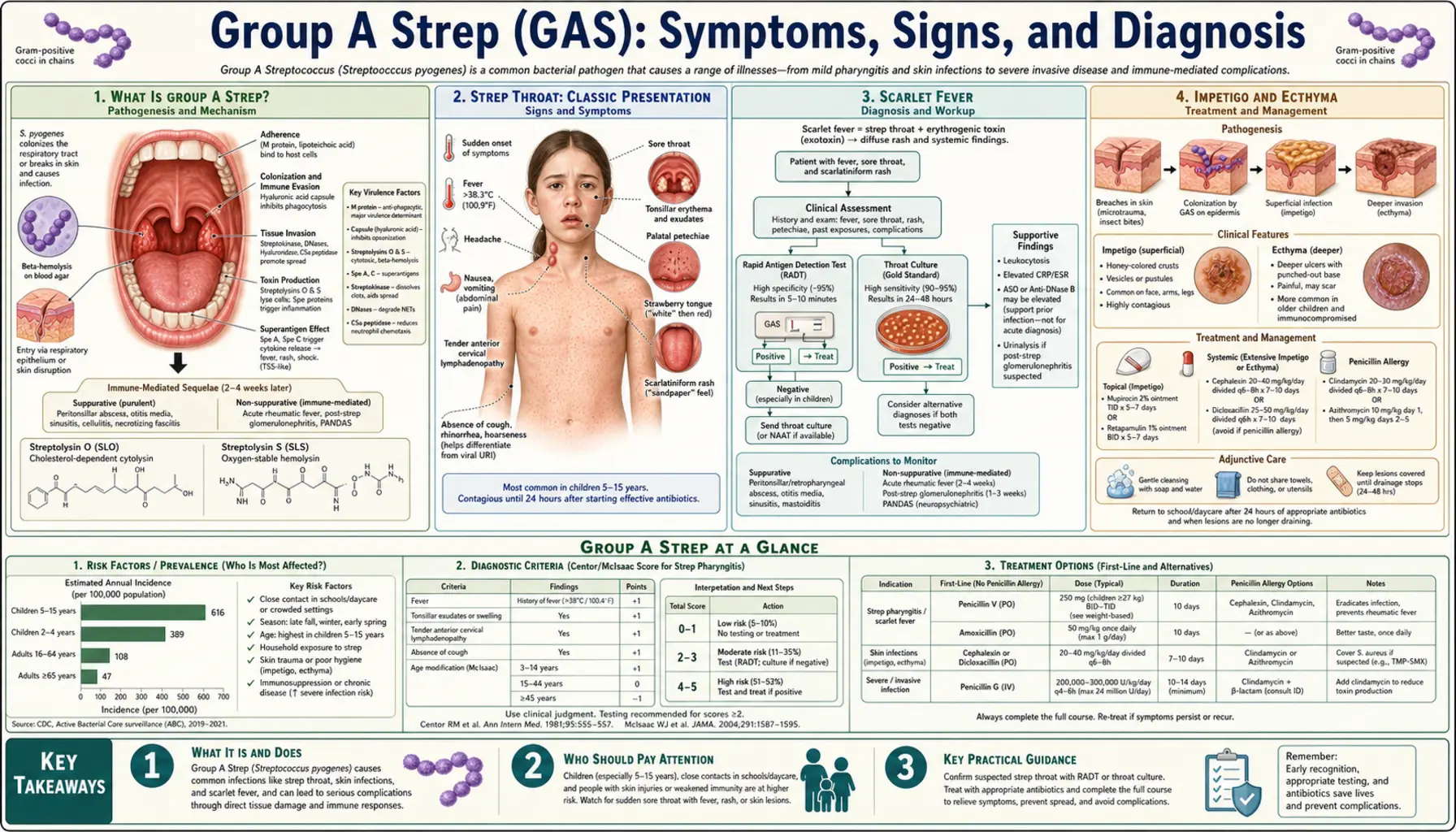
What Is Group A Strep?
Streptococcus pyogenes is a gram-positive coccus that grows in chains and belongs to Lancefield group A — the serological classification system that Rebecca Lancefield developed at Rockefeller University in the 1920s and 1930s. Her work identified the group-specific carbohydrate antigen (the "A" in Group A) and laid the foundation for understanding strep diversity. GAS is beta-hemolytic, meaning it completely lyses red blood cells on blood agar, producing a clear halo — a property visible to any clinical lab technician and useful for presumptive identification.
The bacterium's virulence comes from an arsenal of surface proteins and secreted toxins. The M protein — anchored to the cell wall and projecting outward in a hair-like fimbriae — is the most important. More than 200 distinct M protein types (emm types) exist, and they determine both immune evasion and, in some cases, disease pattern. M1 and M3 types are most commonly associated with invasive infections in wealthy countries. M proteins interfere with complement deposition, help GAS resist phagocytosis, and are the targets of protective immunity — which is why natural infection with one emm type does not protect against others, and why developing a broadly effective vaccine is hard.
GAS also produces streptolysin O and S (which destroy red blood cells and immune cells), streptodornase (which digests DNA in pus, making biofilms less viscous), and hyaluronidase (which helps the bacterium spread through connective tissue). The pyrogenic exotoxins (SPE-A, SPE-B, SPE-C) are superantigens that can trigger the massive cytokine storm responsible for streptococcal toxic shock syndrome. Knowing these mechanisms helps explain why GAS causes so many different diseases in so many different body compartments.
Strep Throat: Classic Presentation
Acute streptococcal pharyngitis is the most common GAS illness. It causes roughly 600 to 700 million episodes of pharyngitis worldwide each year, accounting for 15–30% of all cases of sore throat in children and 5–15% in adults. The classic presentation is sudden-onset sore throat — patients often say they were fine when they went to bed and woke up unable to swallow. Fever above 38°C (100.4°F) is typical. Swollen, tender anterior cervical lymph nodes are almost always present. The tonsils and posterior pharynx are red, often with patchy white or yellow exudate. Headache and abdominal pain (especially in children) are common. Notably absent in classic GAS pharyngitis are the hallmarks of viral sore throat: cough, hoarseness, runny nose, and conjunctivitis.
The Centor score (and its pediatric modification, the McIsaac score) formalizes these observations into a clinical prediction rule. The four Centor criteria are: (1) tonsillar exudate, (2) tender anterior cervical lymphadenopathy, (3) fever by history, and (4) absence of cough. Each criterion scores 1 point; a score of 0–1 makes GAS very unlikely (2–6%), while a score of 4 suggests roughly 51–53% probability. However, because the score still misses a large proportion of true GAS infections even at the high end, most guidelines recommend confirming with a rapid antigen detection test (RADT) or throat culture before prescribing antibiotics. The 2012 IDSA guidelines state explicitly that clinical diagnosis alone is not reliable enough.
Without treatment, strep throat resolves in most people within 3–5 days. Antibiotics shorten illness duration by about a day, reduce contagiousness within 24 hours, and — critically — prevent rheumatic fever, a complication that can cause permanent heart damage. Untreated GAS infection does not reliably trigger protective immunity, and reinfection with different emm types is common throughout childhood.
Scarlet Fever
Scarlet fever is strep throat plus a rash. It occurs when the infecting GAS strain produces pyrogenic exotoxins (SPE-A, SPE-B, or SPE-C) and the patient lacks pre-existing neutralizing antibodies to those specific toxins. The rash typically appears 1–2 days after the throat symptoms begin. It starts on the trunk and spreads outward, sparing the palms and soles. The texture is the disease's signature: fine, sandpaper-like papules that blanch with pressure, often described as feeling like goosebumps. In skin folds — the armpits, groin, and antecubital fossae — the rash concentrates into bright red lines called Pastia's lines, which are pathognomonic.
The face has a distinctive flushed appearance with circumoral pallor — a ring of pallor around the mouth that stands out against the flushed cheeks, as though the patient is wearing clown makeup without the nose. Early in illness, the tongue has a white coating with red papillae poking through (white strawberry tongue); within a few days, the white coat peels off, leaving a raw-looking red surface with enlarged papillae — the classic red or raspberry strawberry tongue. As the rash fades (usually by day 6–9), the skin undergoes desquamation, peeling in sheets from the fingertips, toes, and groin — often alarming parents who see strips of skin coming off their child's hands.
Scarlet fever was a leading killer of children in the 19th and early 20th centuries. It largely disappeared from industrialized countries by the mid-20th century — before widespread antibiotic use — likely due to shifts in circulating emm types toward strains producing less potent toxins, as well as broader population immunity. However, since approximately 2011, scarlet fever incidence has been rising sharply in the United Kingdom, Hong Kong, South Korea, and mainland China, with outbreaks involving emm1 and emm12 strains carrying new prophage elements encoding SPE-A and SPE-C. The reasons for this resurgence are not fully understood and are an active area of research.
Impetigo and Ecthyma
Impetigo is a superficial skin infection that causes the characteristic honey-colored crusted lesions seen on children's faces, especially around the nose and mouth. GAS is one of two major causes — Staphylococcus aureus is the other, and mixed infections are common. GAS impetigo is more common in tropical and subtropical climates and among children in resource-limited settings. Unlike strep throat, which is transmitted mainly by respiratory droplets, skin-strain GAS (which tend to belong to different emm types than throat strains) spreads by direct contact with infected skin or fomites.
Non-bullous impetigo, the most common form, begins as small papules that quickly become vesicles and then rupture to form the characteristic golden-yellow crusts. The lesions are usually painless or mildly itchy. They heal without scarring unless the patient picks at them. Bullous impetigo — characterized by large, fluid-filled blisters that collapse to leave a thin brown crust — is almost exclusively caused by S. aureus (specifically phage type 71 strains producing exfoliative toxins), not GAS.
Ecthyma is a deeper form of impetigo in which the infection penetrates through the epidermis into the upper dermis. It presents as a crusted ulcer with a punched-out appearance and surrounding erythema. Because it involves the dermis, it heals with scarring. Ecthyma is more common in people with diabetes, peripheral vascular disease, or immunocompromise. Importantly, GAS impetigo of any type can seed the kidney and trigger post-streptococcal glomerulonephritis — an immune-mediated complication — but skin-strain GAS does NOT cause rheumatic fever, only throat-strain GAS does. This is a critical distinction for patient counseling.
Erysipelas and Cellulitis
Erysipelas is a superficial skin infection involving the upper dermis and dermal lymphatics. It is nearly always caused by GAS. The hallmark is a sharply demarcated, raised, bright-red plaque with a clearly visible border separating infected from normal skin — you can literally trace the edge with your finger. This sharp border distinguishes erysipelas from cellulitis, in which the infection involves deeper dermis and subcutaneous tissue and has a diffuse, poorly defined border. In practice, however, the two conditions overlap and are often clinically indistinguishable; many authorities treat them as a spectrum.
Erysipelas most commonly affects the lower extremities (after GAS enters through a skin break — a crack between the toes, a small wound, an ulcer) and the face (classically a butterfly pattern across the nose and cheeks, mimicking lupus). Systemic signs — fever, chills, rigors — typically precede or accompany the skin findings. The affected area is warm, tender, and edematous; blistering is common in severe cases. Lymphangitis (red streaks tracking proximally along lymphatic channels) and regional lymphadenopathy may be present.
Recurrence is a major problem. Once the lymphatic channels of a limb are damaged by a first episode of erysipelas, residual lymphedema creates a perpetual reservoir for bacterial growth, and recurrence rates exceed 30% within three years. Long-term low-dose prophylactic penicillin (phenoxymethylpenicillin 250 mg twice daily for 6–12 months) is recommended after a second episode. Weight reduction, compression stockings, and meticulous foot hygiene to eliminate tinea pedis entry points are equally important non-antibiotic strategies.
Invasive Disease Spectrum
Invasive GAS disease occurs when bacteria breach the epithelial barrier and enter sterile body compartments — blood, muscle, fascia, pleural space, or cerebrospinal fluid. The CDC defines invasive GAS as GAS isolated from a normally sterile site or from a skin wound in a patient with necrotizing fasciitis (NF) or streptococcal toxic shock syndrome (STSS). Annual incidence in the United States is approximately 3–4 cases per 100,000 population, with roughly 15,000–20,000 cases and 1,500–2,000 deaths each year. Case fatality rates for NF exceed 25% even in well-resourced intensive care units; STSS kills 30–70% of those affected.
Three invasive syndromes deserve special attention. Necrotizing fasciitis (NF) — often called "flesh-eating disease" in media reports — destroys the fascial planes between the skin and underlying muscle at devastating speed. Early signs are deceptively mild: pain disproportionate to the skin findings, often described as the worst pain of the patient's life. Within hours, the overlying skin develops a dusky, bronze, then frankly necrotic appearance, bullae fill with bloody fluid, and crepitus (gas under the skin, palpable as crackling) may be felt. NF demands surgical debridement within hours of diagnosis; delays measured in hours increase mortality measurably. The sub-article on invasive GAS covers NF and STSS in depth.
Streptococcal toxic shock syndrome (STSS) is defined by hypotension plus two or more of: renal impairment, coagulopathy, hepatic involvement, ARDS, soft-tissue necrosis, or an erythematous rash. It is caused by superantigen pyrogenic exotoxins that activate up to 20% of all T cells simultaneously, unleashing a cytokine storm that causes multiorgan failure. Unlike staphylococcal TSS, STSS is often not associated with a foreign body (tampon) or an obvious skin wound — it can arise from an inapparent pharyngitis or varicella lesion. Bacteremia without a focal source accounts for a significant proportion of invasive cases, particularly in the elderly and immunocompromised.
Puerperal Sepsis
Puerperal (childbed) fever — postpartum uterine infection leading to sepsis — was the leading cause of maternal death in European and American hospitals through the mid-19th century. Ignaz Semmelweis, a Hungarian physician working in Vienna's maternity wards in 1847, made the crucial observation that mortality was far higher in the ward staffed by medical students (who came directly from performing autopsies) than in the midwife ward. He instituted mandatory handwashing with chlorinated lime solution before deliveries and cut mortality from 10–18% to below 2%. He was ridiculed and dismissed; Louis Pasteur and Joseph Lister later provided the germ-theory foundation that vindicated him. Semmelweis died in an asylum in 1865, likely of the very infection he spent his life fighting — S. pyogenes sepsis.
GAS remains a cause of postpartum and post-abortion uterine infection today, though it is now less common than polymicrobial infections. When GAS does cause puerperal sepsis, it tends to be severe and rapid. The bacterium can be introduced from the birth attendant's throat or nasal passages (asymptomatic GAS carriage rates are 5–15% in the general population), from the patient's own skin or vaginal flora, or from the neonate's skin. Outbreaks in obstetric units remain documented in the medical literature and are reportable events. The combination of labor trauma to the uterine endometrium, an immunologically tolerant postpartum state, and the highly invasive M1/M3 strains creates conditions for explosive infection. Fever within 24 hours of delivery, lower abdominal tenderness, and uterine subinvolution should trigger immediate GAS workup including blood cultures.
Global Burden of GAS
GAS is a disease of global reach but profoundly unequal impact. In high-income countries, strep throat is an inconvenience managed with a rapid test and a course of amoxicillin. In low- and middle-income countries (LMICs), the same infection, left untreated, can trigger rheumatic fever — and repeated episodes of rheumatic fever cause rheumatic heart disease (RHD), in which the heart valves are scarred and deformed by the immune response. RHD affects approximately 40 million people worldwide and kills around 300,000–500,000 annually, almost entirely in LMICs where access to penicillin for primary and secondary prevention is limited.
The numbers are staggering. GAS causes an estimated 616 million cases of pharyngitis per year globally. It is responsible for over 111 million cases of skin infection (impetigo, ecthyma) in children in developing regions. Invasive GAS disease claims approximately 500,000 lives annually. RHD is the leading cause of cardiovascular disease in children and young adults in sub-Saharan Africa and South Asia. In some remote Aboriginal Australian communities, the prevalence of RHD reaches 20–30 per 1,000 population — rates comparable to those in Europe before penicillin. The burden of GAS-related illness — pharyngitis, skin infections, invasive disease, rheumatic fever, RHD, post-streptococcal glomerulonephritis, and PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections) — makes GAS one of the most important pathogens worldwide measured by disability-adjusted life years (DALYs).
This inequity has driven renewed interest in GAS vaccine development. Multiple candidate vaccines targeting conserved M protein epitopes, C5a peptidase, and other antigens are in clinical trials. A safe, broadly protective GAS vaccine could prevent millions of cases of RHD and invasive disease annually, particularly in the populations bearing the greatest burden.
Key Research Papers
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):1279–1282. — Search PubMed
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685–694. — Search PubMed
- Walker MJ, Barnett TC, McArthur JD, et al. Disease manifestations and pathogenic mechanisms of group A Streptococcus. Clin Microbiol Rev. 2014;27(2):264–301. — Search PubMed
- Ralph AP, Carapetis JR. Group A streptococcal diseases and their global burden. Curr Top Microbiol Immunol. 2013;368:1–27. — Search PubMed
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med. 2017;377(8):713–722. — Search PubMed
- Barnett TC, Bowen AC, Carapetis JR. The fall and rise of group A Streptococcus diseases. Epidemiol Infect. 2019;147:e4. — Search PubMed
- Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344(3):205–211. — Search PubMed
- Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2002;35(2):113–125. PMID: 12087516
- Stevens DL, Bryant AE. Necrotizing soft-tissue infections. N Engl J Med. 2017;377(23):2253–2265. — Search PubMed
- Cunningham MW. Streptococcus and rheumatic fever. Curr Opin Rheumatol. 2012;24(4):408–416. — Search PubMed
- Oppegaard O, Skrede S, Mylvaganam H, Kittang BR. Emerging streptococcal aetiology of cellulitis in western Norway. Eur J Clin Microbiol Infect Dis. 2018;37(1):89–96. — Search PubMed
Connections
- Group A Strep Overview
- Strep Throat and Pharyngitis
- Invasive GAS and Necrotizing Fasciitis
- Diagnosis: Rapid Strep Tests
- GAS Treatment and Prevention
- ENT Diseases
- Infectious Disease
- Rheumatology
- All Bacteria