Group A Strep Treatment and Prevention: Overview
- Why Treating Strep Throat Matters
- Antibiotic Choice: Penicillin First
- Why 10 Days Still Matters
- When Treatment Does Not Work
- Returning to School and Work
- Do Not Treat Viral Sore Throats
- Symptom Relief While You Recover
- Overview of Prevention
- Key Research Papers
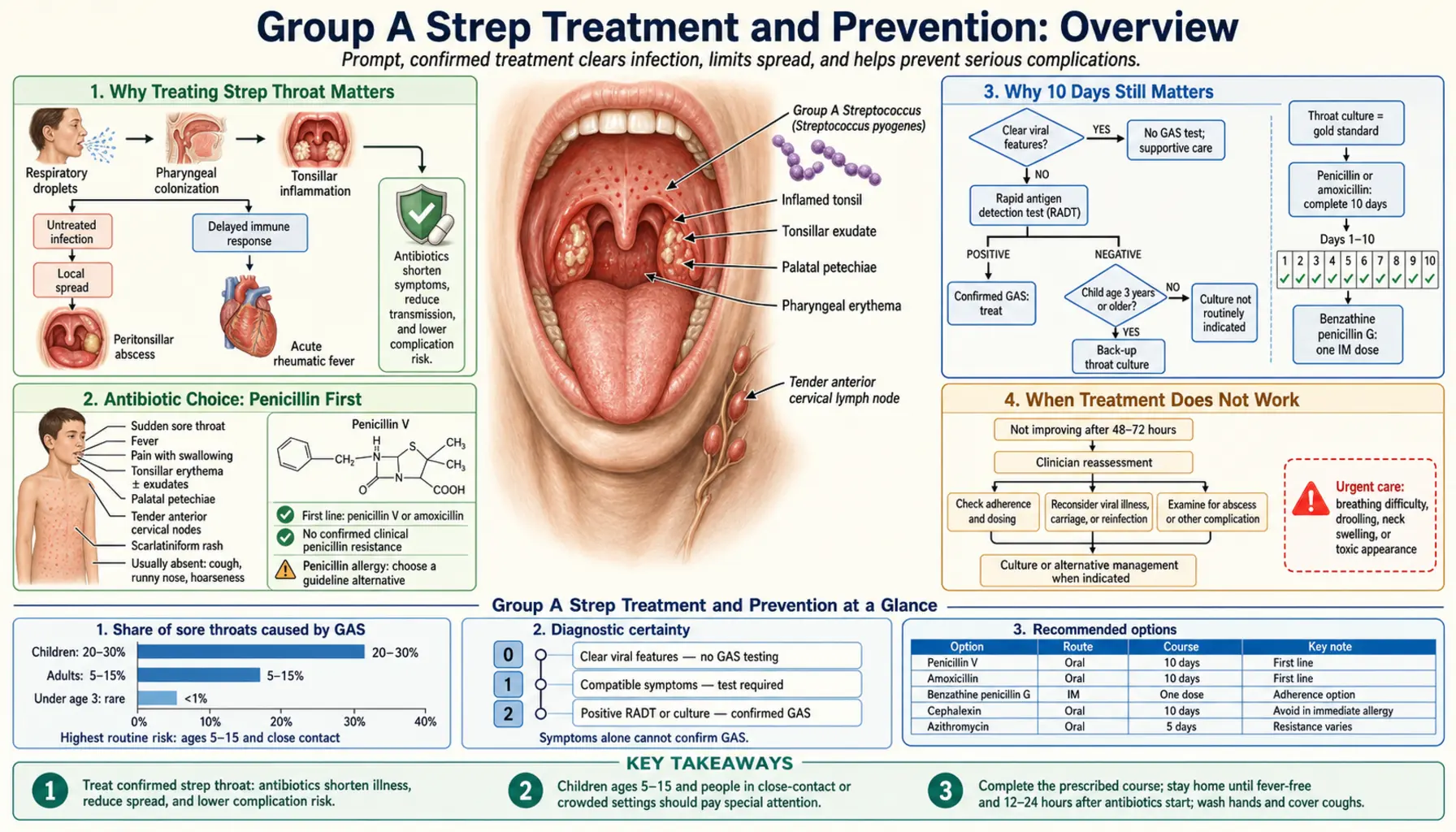
Why Treating Strep Throat Matters
Most sore throats clear up on their own whether you take antibiotics or not. So why does your doctor push for a strep test and a prescription? There are two real reasons — and they are both worth understanding.
Reason 1: Preventing rheumatic fever. Rheumatic fever (RF) is a serious inflammatory condition that can damage the heart valves permanently. It is triggered when Group A Strep pharyngitis goes untreated or is undertreated. The landmark work by Warren and Wannamaker in the 1950s, confirmed repeatedly since, showed that completing a full antibiotic course within about nine days of symptom onset essentially eliminates the risk of RF developing. Miss that window and the immune response that attacks the bacteria can also attack your heart. This is not a theoretical risk — rheumatic heart disease still kills hundreds of thousands of people per year worldwide, mostly in low-income countries, and every preventable case of rheumatic fever avoided in the United States matters.
Reason 2: Cutting contagiousness. Within 24 to 36 hours of starting an antibiotic, GAS bacteria in the throat drop dramatically. A child who was contagious at school in the morning becomes much less of a risk to classmates by the next morning — assuming they are also fever-free. This is why pediatricians give a "24 hours on antibiotics plus no fever" rule for returning to school, not "wait until you feel completely better."
Bonus: Faster recovery. Antibiotics typically shorten illness by about one to two days and reduce pain sooner. That is real, but it is the least important of the three reasons. The big wins are the ones that prevent downstream harm.
Antibiotic Choice: Penicillin First
Penicillin and amoxicillin have been the first-line treatments for Group A Strep pharyngitis for over 80 years — and that has not changed, because GAS has never developed resistance to them. This is genuinely unusual in the world of bacteria. Nearly every other common bacterial pathogen has found ways around at least some antibiotics. GAS has not, at least not against penicillin. No documented clinical resistance has been reported since penicillin entered widespread use in the 1940s.
The Infectious Diseases Society of America (IDSA) 2012 guidelines — the primary reference clinicians use — continue to recommend penicillin V or amoxicillin as first-line choices. Amoxicillin is often preferred for children because it can be given once daily and is available in palatable liquid formulations. Adults who can swallow tablets often receive penicillin V twice or three times daily.
For people with a penicillin allergy, the options depend on the type of allergy:
- Non-severe penicillin allergy (rash only, no hives, no anaphylaxis): a first-generation cephalosporin such as cephalexin is appropriate. Cross-reactivity rates are very low — around 1 to 2 percent — for people with only a minor historical rash.
- Severe penicillin allergy (anaphylaxis, angioedema, urticaria): clindamycin or azithromycin (a macrolide) are used. Note that macrolide resistance in GAS is rising — up to 5 to 10 percent in some regions — so a throat culture with sensitivity testing is helpful when using azithromycin.
Fluoroquinolones (ciprofloxacin, levofloxacin) are not recommended for strep pharyngitis. They are effective against GAS in a test tube but overkill for a self-limited infection, and using them unnecessarily accelerates resistance in other bacteria you may encounter later.
Why 10 Days Still Matters
Ten days of oral penicillin is the standard regimen that has proven to reliably prevent rheumatic fever. This seems long for what often feels like a three-day illness, and adherence is a known challenge — most people start feeling better after four or five days and stop taking the medication.
Several studies have tested shorter courses. Six-day regimens show higher bacteriological failure rates and higher rates of residual GAS in the throat at follow-up. When the goal is just symptom relief, shorter courses work. When the goal is eradicating GAS and protecting against rheumatic fever, the evidence still supports completing ten days.
Amoxicillin once daily as an adherence strategy. A well-designed trial by Gerber and colleagues (2002) showed that once-daily amoxicillin (at a higher single dose) was as effective as the standard twice-daily ten-day penicillin course for pharyngitis, with similar bacteriological eradication rates. This is clinically important: if a child is struggling with the twice-daily schedule, once-daily amoxicillin is a legitimate and evidence-based simplification. Finishing the course becomes easier when there are fewer doses to remember.
Benzathine penicillin G by injection. A single intramuscular injection of benzathine penicillin G is as effective as ten days of oral penicillin and eliminates the adherence problem entirely. It is particularly useful for patients who cannot reliably take oral medication, families with chaotic schedules, or in populations at high risk for rheumatic fever. The main downside is that the injection is painful — the formulation is thick and slow-absorbing by design. It is commonly used in public health programs in developing countries where rheumatic fever rates are high.
When Treatment Does Not Work
Most people with strep throat feel clearly better within 48 to 72 hours of starting antibiotics. If symptoms are not improving by that point, there are a few possibilities to consider.
True treatment failure. This is uncommon with penicillin since GAS resistance does not exist, but it does happen. The most likely explanation is that beta-lactamase-producing bacteria in the throat (other species, not GAS) are inactivating the penicillin before it reaches the GAS. In these cases, switching to amoxicillin-clavulanate or a first-generation cephalosporin is reasonable.
Re-exposure, not treatment failure. A child who returns to a classroom full of untreated strep carriers may simply be getting re-infected. This is especially common in school-age children during winter. If symptoms resolve and then return within a few weeks, test everyone in the household.
Strep carrier state with concurrent viral illness. Some people carry GAS in their throat without it causing symptoms. If they get a viral sore throat at the same time, a rapid strep test will come back positive — but they don't actually have strep pharyngitis. Treating the carrier state is not recommended as a routine matter; it is difficult to eradicate and rarely causes disease.
Recurrent strep throat and tonsillectomy. If a child (or adult) is getting confirmed GAS infections repeatedly — the IDSA threshold often cited is seven episodes in one year, five per year for two years, or three per year for three years — tonsillectomy is worth discussing. A landmark 2008 study by Pfoh and colleagues confirmed that tonsillectomy reduces the frequency of strep throat significantly in children who meet these criteria, though the benefit diminishes over subsequent years as the tonsils would have naturally become less reactive anyway. This is a quality-of-life decision as much as a medical one, and it requires a conversation with an ENT specialist.
Returning to School and Work
The rule is simple: a person with confirmed or suspected GAS pharyngitis can return to school or work after 24 hours on antibiotics and when they are fever-free without fever-reducing medication. Both conditions must be met.
You do not need to wait until you feel 100 percent. Throat soreness can linger for several days even as antibiotic-treated GAS becomes non-infectious. The 24-hour mark is when bacterial counts in secretions have dropped enough to make close contact safe for others.
At home during the first 24 hours:
- Avoid sharing utensils, cups, or water bottles.
- Cover coughs and sneezes. GAS spreads primarily through respiratory droplets, not surfaces — but hand hygiene still matters.
- Wash hands frequently, especially after touching your face or blowing your nose.
- Replace your toothbrush after starting antibiotics. The bristles can harbor bacteria and cause re-infection or re-exposure to family members.
For household members who develop a sore throat, test them promptly. Untreated cases in the same home are the most common source of recurrent strep cycles.
Do Not Treat Viral Sore Throats With Antibiotics
The vast majority of sore throats — estimates range from 70 to 85 percent in adults — are caused by viruses, most commonly rhinovirus, adenovirus, Epstein-Barr virus (infectious mononucleosis), and influenza. Antibiotics do nothing against viruses. Taking them anyway causes real harm:
- Side effects: diarrhea, nausea, yeast infections (vaginal and oral), and allergic reactions ranging from mild rash to anaphylaxis.
- Antibiotic resistance: every unnecessary antibiotic course kills sensitive bacteria in your gut and on your skin, leaving resistant strains to proliferate. This affects your future health and the community around you.
- Unnecessary cost: even generic antibiotics have copays, and missing work for a prescription pickup has costs too.
The McIsaac clinical decision rule (1998) assigns points based on symptoms — fever, absence of cough, swollen tender anterior cervical nodes, tonsillar exudate, and age under 15 — to estimate the probability of GAS being the cause. A score of 0 or 1 suggests less than a 10 percent probability of GAS, and a test is not warranted. A score of 2 or higher warrants a rapid antigen test or throat culture to confirm before prescribing.
When a sore throat is clearly viral (gradual onset, runny nose, cough, hoarseness, no fever or mild fever, no visible exudate), the right treatment is comfort care, not antibiotics. Pain management works well. Rest and hydration matter. The illness typically peaks at days two through four and resolves by day seven to ten.
Symptom Relief While You Recover
Whether your sore throat is bacterial or viral, the following measures genuinely help with comfort while your body or your antibiotics do their work.
Pain and fever: Ibuprofen (Advil, Motrin) and acetaminophen (Tylenol) are both effective for throat pain and fever. Ibuprofen, as an anti-inflammatory, may provide slightly better throat pain relief since the pain of strep throat is largely due to inflammation. Alternate them if needed to maintain more consistent relief. Follow standard dosing for age and weight in children — never give aspirin to children or teenagers with a viral illness (risk of Reye syndrome).
Salt water gargle: Dissolve half a teaspoon of table salt in eight ounces of warm water and gargle for 30 seconds. This is low-cost, low-risk, and genuinely reduces throat swelling and discomfort temporarily. Adults and older children can do this every few hours.
Throat lozenges: Benzocaine-containing lozenges (Cepacol, Chloraseptic) numb the throat and provide short-term relief. They are not a substitute for treatment but make the first 12 to 24 hours more tolerable. Avoid in very young children who cannot gargle or spit.
Staying hydrated: Sore throats make swallowing painful, and people drink less. Dehydration makes everything worse — thicker secretions, higher fever, fatigue. Cold liquids (ice water, popsicles) can temporarily numb the throat and make hydration easier. Warm broth or decaffeinated tea with honey works for adults and children over one year old.
When to go to the emergency room: Most strep throats respond well to outpatient treatment. Go to the ER or call 911 if you or your child:
- Cannot swallow saliva and is drooling (suggests peritonsillar abscess or epiglottitis)
- Has difficulty breathing or a muffled, "hot potato" voice
- Has severe neck stiffness (possible meningitis)
- Has a high fever that is not responding to acetaminophen or ibuprofen
- Develops a spreading rash (especially if bright red and sandpaper-textured — scarlet fever) that is not responding to treatment
- Is an immunocompromised person with worsening symptoms
Overview of Prevention
Strep pharyngitis is contagious. Preventing spread requires interrupting transmission, and protecting high-risk individuals from the most serious consequence — rheumatic heart disease — requires ongoing prophylaxis in some cases.
Hand hygiene: the most effective everyday tool. GAS spreads primarily through respiratory droplets when an infected person coughs, sneezes, or talks. But hands contaminated with droplets then touch mouths and noses, completing the chain of transmission. Regular hand washing with soap and water for at least 20 seconds is the most consistently proven measure for reducing GAS spread in schools and households.
Avoiding close contact with infected people is effective but often impractical in families and classrooms. The 24-hour antibiotic rule helps, but household members and classmates who are untreated carriers continue to circulate GAS silently.
Secondary prophylaxis for rheumatic fever survivors. Anyone who has had confirmed rheumatic fever — whether or not they had carditis at the time — is at high risk for recurrence with each subsequent GAS pharyngitis episode. For these individuals, ongoing low-dose penicillin (oral penicillin V twice daily or monthly benzathine penicillin G injections) is recommended for years, sometimes decades, to prevent repeat rheumatic fever and progressive heart valve damage. The duration depends on whether carditis was present and how severe it was. This is one of the longest-running and best-established preventive antibiotic regimens in medicine.
Vaccine research: A GAS vaccine does not yet exist for human use, but this is an active area. The challenge is that GAS has more than 200 distinct M-protein types (the key surface protein used as a vaccine target), and a vaccine must cover enough types to be broadly effective. A 30-valent M-protein vaccine showed promising Phase 2 results, and newer approaches targeting conserved GAS proteins that don't vary by strain are in development. A licensed vaccine would be transformative for preventing childhood strep pharyngitis, rheumatic fever, and rheumatic heart disease — especially in low- and middle-income countries where these conditions still cause enormous morbidity. See the Prevention and Vaccine Research page for a detailed look at current clinical trials.
Key Research Papers
These are the primary sources underlying current treatment guidelines for Group A Strep pharyngitis.
- Shulman ST et al. (2012) — IDSA Clinical Practice Guideline for GAS Pharyngitis. The most widely used reference for clinicians in the United States, covering diagnosis, treatment selection, duration, and indications for tonsillectomy. — Search PubMed
- Bisno AL et al. (2003) — Practice Guidelines for Diagnosis and Management of Group A Streptococcal Pharyngitis (IDSA). An earlier iteration of IDSA guidance that established many of the current evidence-based principles around penicillin first-line treatment. — Search PubMed
- Bisno AL (2001) — Acute Pharyngitis. New England Journal of Medicine. A landmark review integrating diagnosis, microbiology, and treatment, emphasizing why most sore throats are viral and antibiotics should be reserved for confirmed GAS. — Search PubMed
- Gerber MA et al. (2002) — Once-Daily Amoxicillin for Streptococcal Pharyngitis. Randomized trial demonstrating that once-daily amoxicillin for 10 days was equivalent to standard twice-daily penicillin V, with implications for improving adherence. — Search PubMed
- Peyramond D et al. (1999) — 6-Day Amoxicillin vs. 10-Day Penicillin V. Head-to-head trial showing that shorter antibiotic courses achieve symptom relief but have higher bacteriological failure rates, supporting the 10-day standard for rheumatic fever prevention. — Search PubMed
- Choby BA (2009) — Diagnosis and Treatment of Streptococcal Pharyngitis. American Family Physician. A practical primary-care-focused review summarizing antibiotic options, clinical decision rules, and when to consider further workup. — Search PubMed
- Carapetis JR et al. (2005) — The Global Burden of Group A Streptococcal Diseases. Foundational epidemiological study quantifying the worldwide impact of GAS, including rheumatic heart disease, and providing context for why prevention matters globally. PMID 16253183
- McIsaac WJ et al. (1998) — A Clinical Score to Reduce Unnecessary Antibiotic Use in Patients With Sore Throat. Introduced the clinical scoring system used to estimate GAS probability and guide testing decisions, reducing inappropriate antibiotic prescribing. — Search PubMed
- Watkins DA et al. (2017) — Global, Regional, and National Burden of Rheumatic Heart Disease. New England Journal of Medicine. Comprehensive burden-of-disease analysis showing that rheumatic heart disease causes approximately 320,000 deaths per year — underlining the stakes of consistent strep pharyngitis treatment globally. — Search PubMed
- Pfoh E, Wessels MR, Goldmann D, Lee GM (2008) — Burden and Economic Cost of Group A Streptococcal Pharyngitis. Quantifies the healthcare costs and disease burden of recurrent strep pharyngitis and provides context for tonsillectomy decision-making in children with frequent episodes. — Search PubMed
- Pelucchi C et al. (2012) — Guideline for the Management of Acute Sore Throat (European). European consensus guidelines with particular focus on distinguishing viral from bacterial pharyngitis using clinical scoring before testing, reducing overall antibiotic use in primary care. — Search PubMed
Additional PubMed searches for ongoing research:
- Group A Streptococcal Pharyngitis Treatment
- Rheumatic Fever Prevention and Antibiotic Prophylaxis
- Streptococcus pyogenes Vaccine Clinical Trials
Connections
- Streptococcus Pyogenes Overview
- Symptoms and Diagnosis Overview
- Penicillin and Antibiotic Treatment
- Prevention and Vaccine Research
- Rheumatic Fever Complications
- Infectious Disease
- All Bacteria