Strep Throat and Pharyngitis: Symptoms, Signs, and When to Test
- How Strep Throat Starts
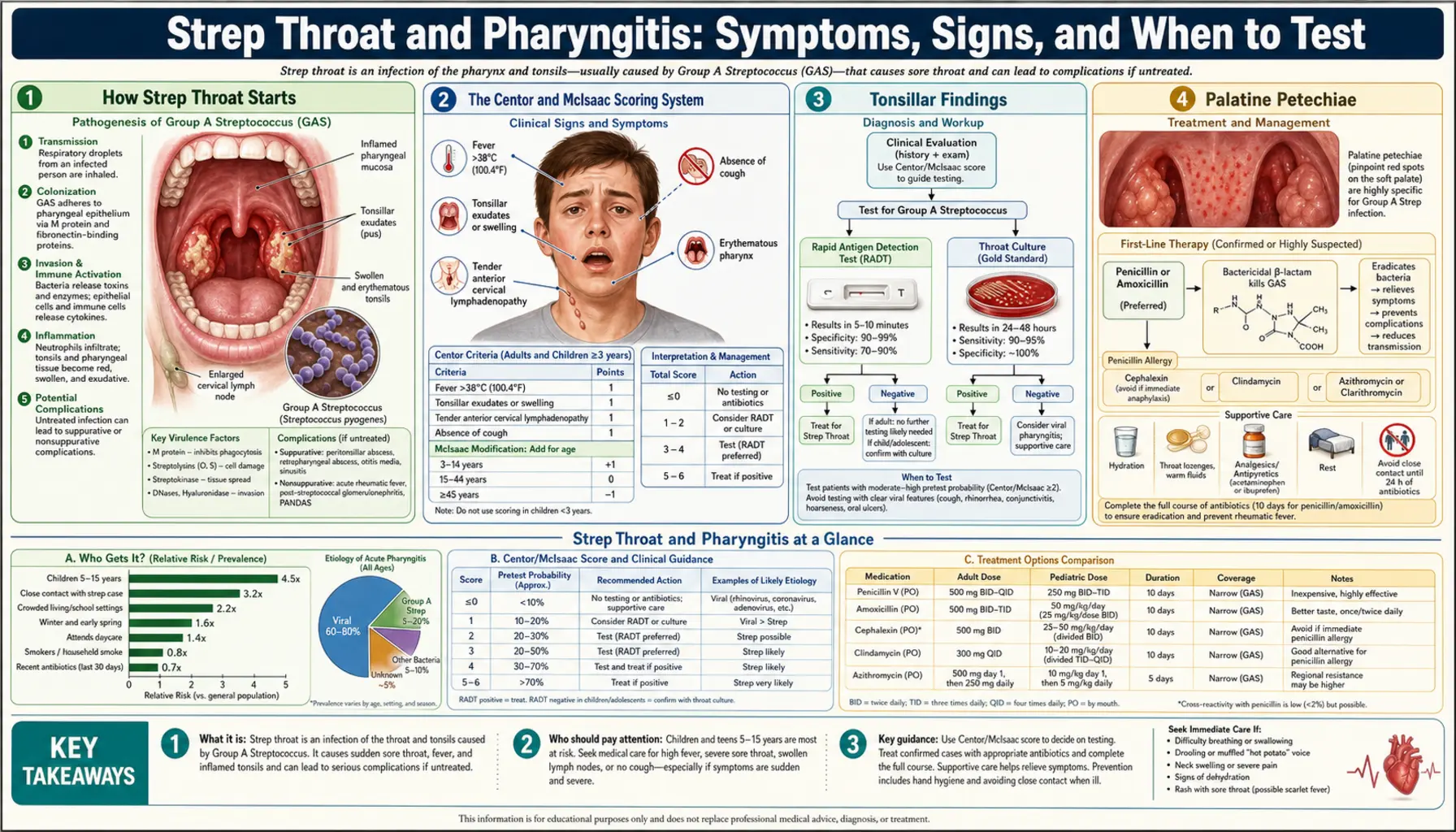
- The Centor and McIsaac Scoring System
- Tonsillar Findings
- Palatine Petechiae
- Anterior Cervical Lymphadenopathy
- Scarlet Fever Rash
- Symptoms in Children vs Adults
- When to Suspect Peritonsillar Abscess
- Differentiating From Viral Pharyngitis
- Key Research Papers
- Connections
How Strep Throat Starts
Strep throat caused by Group A Streptococcus (GAS) — also called Streptococcus pyogenes — has a distinctive feel from the very first hours. Unlike a cold or flu that builds slowly over a day or two, strep typically strikes fast. You feel fine, then within a few hours you have a throat that burns with every swallow and a fever that arrives without much warning.
The hallmark features of strep pharyngitis are:
- Sudden onset of severe sore throat — pain with swallowing that often feels out of proportion to what a sore throat "should" feel like
- Fever at or above 38.3°C (101°F) — sometimes reaching 39–40°C (102–104°F) in children
- Absence of cough — this is one of the most reliable distinguishing features; strep does not cause cough, while most viral throat infections do
- Absence of runny nose and nasal congestion — another strong viral indicator that is usually absent with strep
The incubation period — time from exposure to symptoms — is typically two to five days. Strep spreads through respiratory droplets, so sharing food, drinks, or close contact with an infected person in that window is the usual path. The bacteria attach to cells lining the throat and tonsils, triggering an inflammatory response that causes the swelling, redness, and pain you feel.
It is worth knowing that roughly 20–30% of children carry GAS in their throats with no symptoms at all — these are called "strep carriers." A carrier who then develops a viral sore throat may test positive on a rapid test even though the strep is not the cause. This is one reason why combining test results with the clinical picture (including the Centor/McIsaac score below) matters.
The Centor and McIsaac Scoring System
Doctors and nurse practitioners use a simple point-based checklist to decide whether a sore throat warrants a test or even empiric treatment. The McIsaac score — an updated version of the original Centor criteria — assigns one point for each of these four features:
- Tonsillar exudate or swelling — pus visible on the tonsils, or tonsils that are noticeably enlarged
- Tender anterior cervical lymphadenopathy — swollen, painful lymph nodes in the front of the neck
- No cough — the absence of cough adds a point because cough strongly suggests a virus
- History of fever or fever present — a temperature above 38°C (100.4°F) at any point during the illness
McIsaac also added an age adjustment: subtract one point if the patient is 45 years or older (adults are far less likely to have GAS pharyngitis), and add one point for ages 3–14. This gives a possible range of 0 to 5 points.
How the score guides testing and treatment:
- 0–1 points: Strep is very unlikely. No test needed, no antibiotic. Treat symptoms with pain relievers and rest.
- 2–3 points: Moderate probability. Test with a rapid antigen detection test (RADT). Treat if positive; hold antibiotics if negative.
- 4–5 points: High probability. Some guidelines support empiric treatment without testing in resource-limited settings, though testing is still preferred when available.
The score was validated in a large Canadian study (McIsaac 1998, PMID 9875180) and is now embedded in the Infectious Diseases Society of America (IDSA) guidelines. It does not replace a test — it tells you how urgently you need one.
Tonsillar Findings
The tonsils are two pads of lymphatic tissue sitting at the back of the throat, one on each side. In strep pharyngitis, they often become enlarged and red — sometimes dramatically so, nearly meeting in the midline and making swallowing feel like pushing food through a narrow gap.
About half of people with confirmed strep will develop tonsillar exudate — patches of white or yellowish material on the surface of the tonsils. This is a mixture of dead immune cells, bacteria, and tissue debris. It looks alarming but is not dangerous by itself. The presence of exudate does make strep more likely, but it is not a reliable solo predictor: infectious mononucleosis (mono, caused by Epstein-Barr virus) can produce identical-looking white exudate, and about half of strep cases never develop visible pus at all.
Key observations during a throat examination:
- Bilateral redness and enlargement — both tonsils red and swollen, typical of strep
- White or gray patches — exudate on tonsillar surfaces; more specific for bacterial infection than viral
- Membrane covering the tonsil — a gray-white membrane that bleeds when scraped suggests diphtheria (very rare in vaccinated populations) rather than strep
- Unilateral bulging — one tonsil pushed forward and the uvula shifted to the opposite side; this suggests peritonsillar abscess, a complication requiring drainage (see Section 8)
Clinicians are taught not to rely on tonsillar appearance alone. A severely inflamed throat with no exudate can still be strep; a throat covered in white patches can still be viral. The visual exam is one data point among several.
Palatine Petechiae
Look at the soft palate — the soft, movable part at the back of the roof of your mouth, just above the tonsils. In some cases of strep pharyngitis you will see petechiae: tiny pin-point red or purple spots, usually smaller than 2 mm, scattered across the surface. These are tiny areas of bleeding under the mucosal surface caused by the intense inflammatory response and capillary fragility.
Palatine petechiae are considered one of the most specific signs of strep throat. When they are present, they point strongly toward GAS as the cause rather than a virus. However, they are not sensitive — most strep cases never produce visible petechiae — so their absence does not rule anything out.
A practical point: petechiae on the palate can also occur with infectious mononucleosis (in about 50% of mono cases), so a positive mono test alongside petechiae changes the picture. If a teenager or young adult has severe exudative pharyngitis with petechiae, fatigue out of proportion to the throat symptoms, and posterior cervical lymphadenopathy (lymph nodes in the back of the neck rather than the front), mono should be high on the list.
Examining for petechiae requires a good light and a tongue depressor to fully visualize the soft palate. Patients sometimes notice a feeling of raw sensitivity at the back of the roof of the mouth before petechiae are visible.
Anterior Cervical Lymphadenopathy
The lymph nodes of the neck serve as immune checkpoints, filtering fluid and bacteria that drain from the throat and mouth. In strep pharyngitis, the nodes most likely to enlarge are the anterior cervical nodes — a chain running along the front edge of the sternocleidomastoid muscle on each side of the neck, roughly beneath the angle of the jaw.
With active strep infection these nodes become:
- Enlarged — often reaching 1–2 cm or more, noticeable even without pressing
- Tender — pressure causes pain, sometimes quite sharp; this tenderness is what earns a point on the McIsaac score
- Firm but movable — they slide under the fingertip; fixed or very hard nodes suggest a different diagnosis
The location matters clinically. Anterior cervical adenopathy is associated with bacterial infections including strep. Posterior cervical adenopathy — nodes behind the sternocleidomastoid, toward the back of the neck — is more associated with viral infections, particularly Epstein-Barr virus (mono) and rubella. Generalised lymphadenopathy (swollen nodes in the armpits, groin, and neck all at once) raises concern for mono, HIV, or lymphoma and warrants broader evaluation.
Nodes typically remain enlarged and tender for several days even after antibiotic treatment begins, gradually shrinking over one to two weeks. Persistent or enlarging nodes after two weeks of appropriate treatment deserve re-evaluation.
Scarlet Fever Rash
Some strains of Streptococcus pyogenes carry genes that allow them to produce proteins called pyrogenic exotoxins (also known as erythrogenic toxins). In susceptible people who lack prior immunity to these toxins, these proteins trigger a systemic inflammatory response that produces a characteristic rash. The result is scarlet fever — historically feared as a killer of children, now usually a manageable complication when caught and treated promptly.
The scarlet fever rash has a distinctive progression and texture:
- Onset: Appears 12–48 hours after the throat symptoms begin
- Starting location: Neck, groin, and axillae (armpits) first, then spreads to the trunk and extremities within hours to a day
- Texture: Often described as feeling like sandpaper — tiny raised bumps (papules) on a diffusely red background, the skin feels rough to the touch even where it looks uniformly red
- Pastia lines: Bright red lines of concentrated rash in the skin creases of the elbows and armpits, a distinctive finding
- Circumoral pallor: The area around the mouth stays pale while the cheeks are flushed — creating a ring of white skin around the lips that looks out of place
- Desquamation: As the illness resolves, the skin peels, starting on the face and then moving to the hands, feet, and trunk; this peeling can last one to three weeks
The tongue also goes through a characteristic progression that many parents notice and find alarming. In the first day or two it is covered in a white coating with red bumps showing through — called a "white strawberry tongue." As the white coating sheds over days two to five, the raw red bumps underneath remain visible — the "red strawberry tongue." Both phases are normal and resolve with treatment.
Scarlet fever does not indicate a more dangerous infection than strep throat without rash — it simply means the infecting strain carries the exotoxin gene and the patient's immune system responded to it. Treatment is the same: penicillin or amoxicillin. The rash itself requires no special treatment. A resurgence of scarlet fever cases was documented in the UK and East Asia from 2014 onward, possibly linked to spread of specific GAS clones carrying phage-encoded toxin genes (Hayes 2017, PMID 28455279).
Symptoms in Children vs Adults
Strep throat is primarily a disease of school-age children, with peak incidence between ages 5 and 15. The way it presents, however, differs enough between children and adults that the same scoring criteria need to be interpreted differently across age groups.
In children (ages 3–15):
- Sore throat is almost always present, but younger children (under 3) may not be able to articulate it; they may simply refuse food, drool more, or cry during meals
- Abdominal pain, nausea, and vomiting are common, sometimes preceding the sore throat — parents may initially suspect a stomach bug
- Headache is frequent and can be severe
- High fever (39–40°C / 102–104°F) is typical and can trigger febrile seizures in children under 5
- Tonsillar exudate is more common in children than adults
- Scarlet fever rash is more commonly seen in children
- The risk of acute rheumatic fever (ARF), a serious complication, is highest in children ages 5–15; this is the primary reason we treat strep at all
In adults:
- Strep accounts for only 5–15% of pharyngitis cases in adults, compared to 15–30% in children
- Adults are less likely to develop tonsillar exudate and high fever than children with the same infection
- Adults over 45 have very low risk of ARF, so the threshold to test and treat is higher; the McIsaac score subtracts a point for this age group
- Recurrent strep in adults — more than 4–6 episodes per year — raises the question of chronic carriage or whether tonsillectomy should be considered
- Adults with weakened immune systems (diabetes, steroid use, HIV) are at higher risk of complications from untreated strep
Children under 3 rarely develop ARF and rarely have true strep pharyngitis (they more commonly get strep skin infections). Routine testing is not recommended for this age group unless a sibling or household contact has a confirmed strep infection.
When to Suspect Peritonsillar Abscess
A peritonsillar abscess (PTA) — sometimes called a "quinsy" — is a collection of pus that forms in the soft tissue just outside the capsule of one tonsil. It is the most common deep neck infection and develops when strep (or mixed bacteria) spreads beyond the tonsil into the surrounding space. Most cases follow an episode of tonsillitis, sometimes one that seemed to be improving.
The warning signs that suggest a sore throat has progressed to peritonsillar abscess are:
- Severe, worsening unilateral throat pain — pain that is dramatically worse on one side than the other, often rated 8–10 out of 10
- Trismus — difficulty opening the mouth fully, caused by spasm of the nearby pterygoid muscle; patients can often open their jaw only 1–2 cm instead of the normal 4–5 cm
- "Hot potato voice" — a muffled, thick quality to the voice, as if the patient has a hot potato in their mouth; caused by swelling pushing the soft palate forward
- Drooling — difficulty swallowing even saliva, so it accumulates and drips
- Uvular deviation — on examination, the uvula (the little dangling structure at the back of the throat) is pushed away from the swollen side; the tonsil on that side bulges toward the midline
- Fullness or bulging of the anterior tonsillar pillar — the tissue in front of the tonsil looks swollen and tense
This is a medical urgency. A peritonsillar abscess will not resolve on its own with antibiotics alone — it requires drainage, either by needle aspiration or incision and drainage (I&D) performed by an emergency medicine physician or otolaryngologist (ENT specialist). Delay risks spread of the infection into the deep neck spaces, which can compress the airway or cause life-threatening descending mediastinitis.
If you or someone in your care develops unilateral throat pain with trismus, muffled voice, and difficulty swallowing, go to an emergency department rather than waiting for a regular clinic appointment. An untreated PTA is one of the genuine surgical emergencies of ENT medicine (Frost 2018, PMID 30481380).
Differentiating From Viral Pharyngitis
The most important practical skill in managing a sore throat is knowing whether it is likely bacterial (and needs antibiotics) or viral (and should be managed with supportive care alone). This matters because antibiotics do nothing for viral infections, and unnecessary prescribing contributes to antibiotic resistance while exposing patients to side effects.
Viruses cause the vast majority of pharyngitis cases — roughly 70–80% across all age groups. The most common viral culprits are rhinovirus (common cold), adenovirus, Epstein-Barr virus, and influenza. Each tends to produce a syndrome that goes beyond the throat alone.
Features that strongly suggest a viral cause:
- Cough — the single most reliable predictor of viral pharyngitis; strep does not cause cough
- Rhinorrhea (runny nose) — nasal congestion and discharge are hallmarks of respiratory viral infections
- Hoarseness — loss of voice quality suggests laryngitis from viral infection; strep does not inflame the larynx
- Conjunctivitis — red, watery, or itchy eyes accompanying a sore throat point strongly toward adenovirus ("pharyngoconjunctival fever")
- Oral ulcers or vesicles — blistering sores on the gums, tongue, or hard palate indicate herpangina (Coxsackievirus) or primary herpes simplex, not strep
- Gradual onset over several days — viral illnesses tend to build slowly; strep strikes fast
- Posterior cervical lymphadenopathy — nodes in the back of the neck suggest Epstein-Barr virus (mono)
- Splenomegaly or profound fatigue — extreme tiredness and a tender, enlarged spleen point to mono
Even experienced clinicians cannot reliably distinguish strep from viral pharyngitis on clinical grounds alone with sufficient accuracy to justify treating without a test. The IDSA recommends that the diagnosis be confirmed by rapid antigen test or throat culture before antibiotic prescribing — except in cases of documented epidemic GAS or very high clinical probability with scarlet fever rash (Shulman 2012, PMID 23139253).
The practical rule: if you have a sore throat and a cough, it is almost certainly viral. Rest, fluids, honey, and over-the-counter pain relievers are your best treatment. If you have a sore throat without a cough, plus fever and swollen neck nodes, getting tested is worth the few minutes it takes.
Key Research Papers
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2012;55(10):1279–1282 — Search PubMed — The authoritative IDSA guideline. Establishes the requirement for microbiologic confirmation before antibiotic prescribing and sets the framework for the rapid antigen test plus throat culture backup protocol.
- Bisno AL, Gerber MA, Gwaltney JM, Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2002;35(2):113–125 — Search PubMed — Earlier IDSA guideline underpinning the 2012 update; covers epidemiology, clinical criteria, and rationale for treatment to prevent rheumatic fever.
- Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344(3):205–211 — Search PubMed — Landmark clinical review in the New England Journal explaining the biology, epidemiology, and diagnostic approach to acute pharyngitis; essential background reading.
- McIsaac WJ, White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158(1):75–83 — Search PubMed — Original derivation and validation of the McIsaac score; demonstrated that applying the age-adjusted Centor criteria could reduce antibiotic prescribing by 48% without missing significant GAS cases.
- Aalbers J, O'Brien KK, Chan WS, et al. Predicting streptococcal pharyngitis in adults in primary care: a systematic review of the diagnostic accuracy of symptoms and signs and validation of the Centor score. BMC Med. 2011;9:67 — Search PubMed — Meta-analysis examining the accuracy of each individual Centor criterion and validating the composite score across multiple primary care settings.
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172(11):847–852 — Search PubMed — Validation study using a large electronic health record dataset; found both scores perform similarly and confirmed their utility as pre-test probability tools.
- Choby BA. Diagnosis and treatment of streptococcal pharyngitis. Am Fam Physician. 2009;79(5):383–390 — Search PubMed — Practical overview for primary care providers covering clinical presentation, diagnostic testing, and treatment in a family medicine context; excellent summary tables.
- Pelucchi C, Grigoryan L, Galeone C, et al. Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18 Suppl 1:1–27 — Search PubMed — European Society for Clinical Microbiology and Infectious Diseases (ESCMID) guideline; broadly consistent with IDSA but includes European epidemiology and antibiotic resistance patterns.
- Frost HM, Edmonson MB. Epidemiology and outcomes of peritonsillar abscess in children with and without prior tonsillitis. JAMA Otolaryngol Head Neck Surg. 2018;144(12):1079–1087 — Search PubMed — Large pediatric cohort study examining who develops peritonsillar abscess, clinical features at presentation, and outcomes with needle aspiration vs incision and drainage.
- Hayes CS, Williamson H Jr. Management of group A beta-hemolytic streptococcal pharyngitis. Am Fam Physician. 2001;63(8):1557–1564, and: Lamagni T, Guy R, Chand M, et al. Resurgence of scarlet fever in England, 2014–16: a population-based surveillance study. Lancet Infect Dis. 2017;17(6):627–635 — Search PubMed — Epidemiological analysis of the scarlet fever resurgence documented in England from 2014 onward; identified specific emm-types and phage-encoded pyrogenic toxin genes driving the upsurge.
Additional PubMed searches for further reading:
- Streptococcal pharyngitis diagnosis — PubMed
- Centor McIsaac score pharyngitis — PubMed
- Peritonsillar abscess management — PubMed
- Scarlet fever pyrogenic exotoxin — PubMed
- Viral vs bacterial pharyngitis differentiation — PubMed
Connections
- All Bacteria
- Group A Strep Overview
- Symptoms & Diagnosis Hub
- Rapid Strep Tests and Throat Culture
- Penicillin and Antibiotic Treatment
- Rheumatic Fever Complications
- ENT Diseases