Streptococcus pneumoniae: Pneumococcal Disease, Pneumonia, and Meningitis
Symptoms & Diagnosis
Fever, productive cough, and chest pain — the classic pneumococcal pneumonia triad.
Pneumonia Symptoms
CAP severity scoring, lobar consolidation, and when to hospitalize.
Meningitis & Invasive Disease
Pneumococcal meningitis, bacteremia, and septic shock.
Diagnosis Tests
Blood cultures, sputum culture, urinary antigen test, and chest X-ray.
Treatment & Prevention
Antibiotics for pneumonia and the vaccines that prevent it.
Antibiotic Treatment
Penicillin, amoxicillin, and respiratory fluoroquinolones for CAP.
Pneumococcal Vaccines
PCV13, PCV20, PCV21, and PPSV23 — who gets which vaccine and when.
Antibiotic Resistance
Penicillin-non-susceptible pneumococci, multidrug resistance, and serotype shifts post-vaccine.
Streptococcus pneumoniae (the pneumococcus) is the leading bacterial cause of community-acquired pneumonia and a major cause of meningitis and sepsis — responsible for over 1 million deaths per year globally. It is particularly dangerous in elderly adults, infants, and people without a spleen, and vaccines have transformed outcomes in vaccinated populations. Despite its fearsome reputation as a killer, the pneumococcus is also a harmless colonizer of the throat in millions of people, and understanding why it turns dangerous in some while ignoring others is one of the more fascinating puzzles in infectious disease.
Table of Contents
- What S. pneumoniae Is
- Serotypes and Carriage
- Diseases It Causes
- Symptoms
- Diagnosis
- Treatment and Antibiotic Resistance
- Vaccines — PCV15, PCV20, and PPSV23
- Research Papers
- Connections
- Featured Videos
What S. pneumoniae Is
Streptococcus pneumoniae is a gram-positive, lancet-shaped bacterium that typically pairs up (it is described as "diplococcus"). It was first isolated in the 1880s, independently by Louis Pasteur in France and George Miller Sternberg in the United States, from the saliva of people with pneumonia. For much of the twentieth century, it was one of the most feared pathogens in medicine — pneumococcal pneumonia killed vast numbers of people before antibiotics existed, and early antibiotic-resistant strains began appearing even as penicillin became widely available.
One of its most important physical features is its polysaccharide capsule — a thick sugar coat that surrounds the bacterium and makes it highly resistant to being engulfed and destroyed by the immune system's phagocytes (the cells that are supposed to eat bacteria). The capsule is the primary virulence determinant of the pneumococcus, and strains without a capsule are far less dangerous. Crucially, the capsule is also the main target of protective immunity — both from natural infection and from vaccines. Antibodies that recognize capsular polysaccharides mark the bacterium for destruction by phagocytes, a process called opsonization.
The bacterium also produces a pore-forming toxin called pneumolysin that damages lung cells and red blood cells, enzymes that help it evade immune recognition, and proteins that allow it to attach to and invade mucosal surfaces. Together these virulence factors explain why, once the pneumococcus breaches the airway's defenses, it can spread rapidly and cause severe tissue damage.
Serotypes and Carriage
S. pneumoniae has one of the most diverse capsular polysaccharide systems of any bacterial pathogen: over 100 distinct serotypes have been identified, each defined by a different polysaccharide structure. This diversity matters enormously because immunity to one serotype does not cross-protect against others, and because vaccine formulations can only target a limited number of serotypes at a time. Not all serotypes are equally dangerous: a relatively small subset (around 20–30) account for the vast majority of invasive pneumococcal disease worldwide, though the specific dominant serotypes vary by geography and age group.
Nasopharyngeal carriage — where the bacterium lives in the nose and throat without causing illness — is extremely common, especially in young children. Studies in pre-vaccine eras found that up to 40–60% of healthy children under five carried S. pneumoniae at any given time, and children are the main reservoir from which adults become colonized. Most carriers never develop disease; invasive infection is the exception, not the rule, and depends on a combination of bacterial virulence, host immune status, and co-factors such as viral respiratory infections (influenza and other respiratory viruses can disrupt the mucosa and allow the pneumococcus to penetrate deeper).
The introduction of conjugate vaccines has dramatically reduced carriage of vaccine-targeted serotypes, particularly in children, which has had the additional benefit of reducing disease in unvaccinated adults through herd protection. However, serotype replacement — where non-vaccine serotypes increase in prevalence to fill the ecological niche — has been an important and ongoing challenge, driving the development of vaccines targeting ever-broader serotype ranges.
Diseases It Causes
S. pneumoniae causes a wide spectrum of illnesses ranging from common and relatively mild to rare and life-threatening:
Community-Acquired Pneumonia (CAP)
Pneumococcal pneumonia is the most common serious manifestation. The bacterium spreads from the nasopharynx to the lungs, typically during or after a viral respiratory infection that has disrupted normal defenses, and causes lobar pneumonia — consolidation of one or more lobes of the lung filled with fluid and inflammatory cells. It can progress to bacteremia (bacteria in the bloodstream) in up to 25–30% of patients, which significantly worsens prognosis. Even in high-income countries, pneumococcal pneumonia carries a substantial mortality rate in elderly patients and those with underlying illness.
Meningitis
Pneumococcal meningitis is one of the most severe forms of bacterial meningitis. The bacterium reaches the meninges (membranes covering the brain and spinal cord) either by direct spread from nearby infection (such as sinusitis or otitis media) or through the bloodstream. It causes intense inflammation of the meninges, raised pressure inside the skull, and direct injury to brain tissue. Even with appropriate antibiotic treatment, death rates from pneumococcal meningitis remain around 20–30% in adults, and a significant proportion of survivors sustain permanent neurological damage — deafness, cognitive impairment, or focal neurological deficits.
Otitis Media (Middle Ear Infection)
The pneumococcus is one of the two most common causes of acute otitis media (the other being Haemophilus influenzae). Middle ear infections are usually not dangerous in themselves, but they are the most common reason for antibiotic prescriptions in children and a common trigger for surgical tube placement. The widespread use of pneumococcal conjugate vaccines has led to significant reductions in childhood otitis media rates.
Sepsis
Pneumococcal bacteremia without an obvious focus of infection can rapidly progress to sepsis, a systemic inflammatory response with organ dysfunction. People without a spleen (either surgically removed or functionally absent, as in sickle cell disease) are at extreme risk of overwhelming pneumococcal sepsis, which can be fatal within hours. This is why asplenic patients are given lifelong prophylactic antibiotics and are a priority for pneumococcal vaccination.
Sinusitis and Other Sites
The pneumococcus also causes a proportion of bacterial sinusitis cases and, less commonly, pericarditis (infection around the heart), peritonitis, and septic arthritis.
Symptoms
Symptoms of pneumococcal disease depend heavily on which organ system is affected.
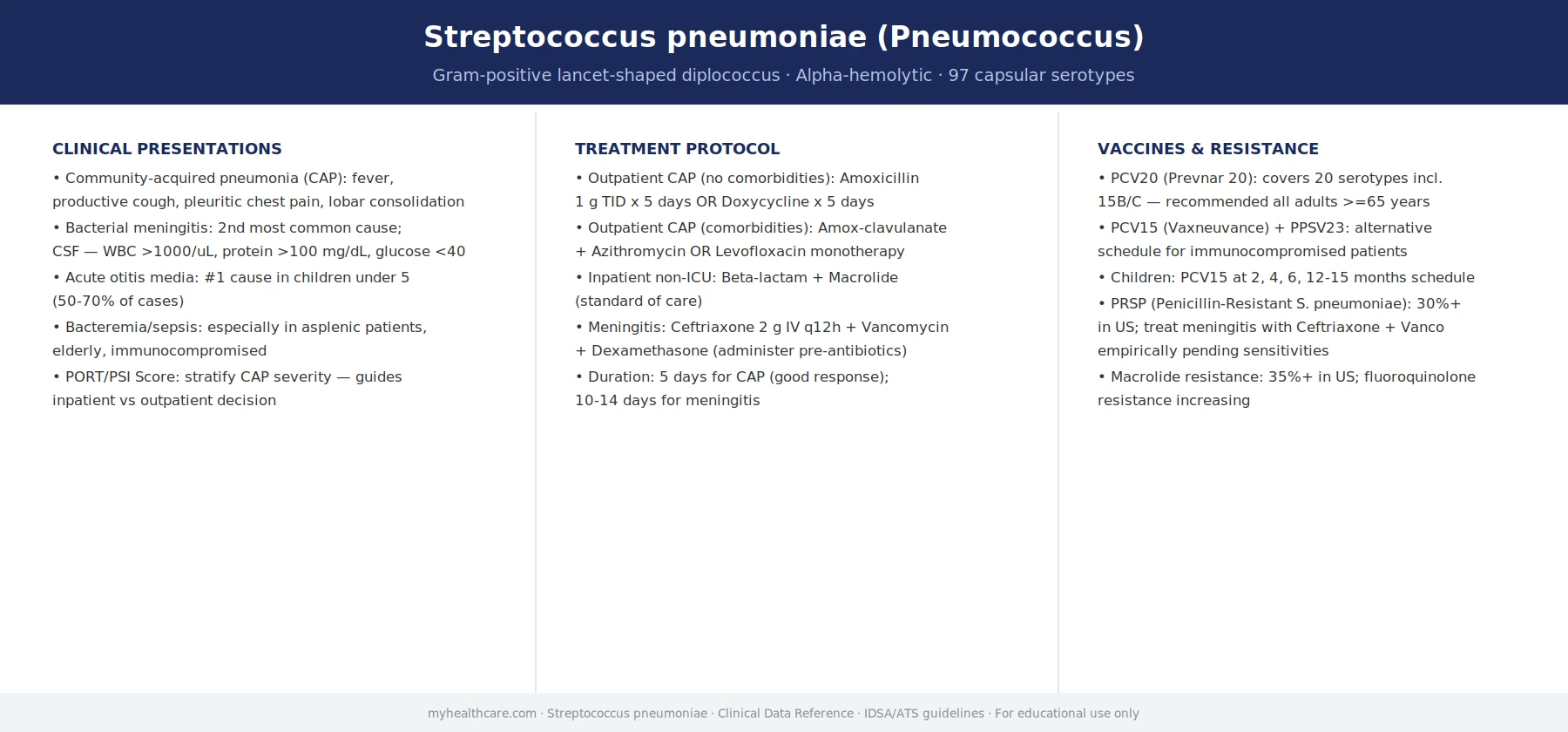
In pneumococcal pneumonia, the classic presentation is an abrupt onset of high fever, shaking chills (rigors), chest pain that worsens with breathing (pleuritic chest pain), productive cough (often with rust-colored or blood-tinged sputum), and shortness of breath. Patients often look and feel dramatically ill within hours of onset. Elderly patients may present more subtly, with confusion, weakness, or a fall rather than the classic fever-and-cough picture, which can delay diagnosis.
In pneumococcal meningitis, the classic triad is fever, severe headache, and neck stiffness (meningismus). Sensitivity to light (photophobia) and sound (phonophobia) are common. Altered mental status — confusion, lethargy, or frank coma — is a sign of severe disease and a medical emergency. A non-blanching rash (a rash that does not fade when pressed) can occur in pneumococcal sepsis and is a sign of serious systemic infection.
In otitis media, the hallmark is ear pain (otalgia), muffled hearing, and sometimes fever, particularly in children. Young children who cannot yet express ear pain may pull at their ear, be unusually irritable, or have disturbed sleep.
Diagnosis
Diagnosis depends on which syndrome is suspected and usually involves a combination of clinical assessment, imaging, and laboratory testing.
- Chest X-ray and CT scan. Lobar consolidation on a chest X-ray is strongly suggestive of bacterial pneumonia, including pneumococcal disease, though it cannot distinguish the causative organism. CT is more sensitive and can detect complications such as pleural effusion or abscess.
- Blood cultures. Blood cultures are essential in patients admitted to hospital with pneumonia, and are the standard way to confirm bacteremia. They are positive in roughly 25–30% of pneumococcal pneumonia cases in hospitalized patients. Cultures take 24–48 hours to grow, so treatment must begin before results return.
- Sputum culture and Gram stain. In patients who can produce sputum, a properly collected sample can identify the causative organism in pneumonia. A Gram stain showing gram-positive diplococci with numerous white blood cells (and few contaminating cells from the mouth) is strongly suggestive of pneumococcal pneumonia.
- Urine pneumococcal antigen test. A rapid test for pneumococcal capsular antigen in urine is widely used in hospitalized patients with pneumonia. It detects most clinically relevant serotypes within hours, which can allow earlier, targeted therapy even before cultures return. Its main limitation is that it does not tell you the serotype or antibiotic susceptibility of the organism.
- Lumbar puncture (spinal tap). When meningitis is suspected, a lumbar puncture to analyze the cerebrospinal fluid (CSF) is essential — it typically shows a high white blood cell count, elevated protein, low glucose, and may show gram-positive diplococci on Gram stain. CSF culture and PCR confirm the diagnosis. Lumbar puncture should generally be done before antibiotics in bacterial meningitis if it can be done safely and without delay, because CSF cultures become negative quickly after antibiotic therapy begins.
Treatment and Antibiotic Resistance
Penicillin was the first effective antibiotic for pneumococcal disease and for decades was used as a simple single drug. That era is over. S. pneumoniae has developed resistance to penicillin through a mechanism different from most bacteria: rather than producing an enzyme that destroys the antibiotic, pneumococci have gradually modified their penicillin-binding proteins (the targets of penicillin) so that the drug binds less effectively. The result is a spectrum from fully sensitive to intermediately resistant to fully resistant strains, and resistance rates vary widely by geography and patient population.
Current treatment recommendations for community-acquired pneumococcal pneumonia in outpatients who are otherwise healthy generally use a macrolide antibiotic such as azithromycin or a respiratory fluoroquinolone (levofloxacin or moxifloxacin). Hospitalized patients typically receive a beta-lactam (amoxicillin-clavulanate or a cephalosporin) plus a macrolide, or a fluoroquinolone alone, with the choice guided by local resistance patterns and patient factors.
For pneumococcal meningitis, the stakes are higher and speed is critical. Current empirical treatment pending culture results typically combines a high-dose third-generation cephalosporin (ceftriaxone or cefotaxime) with vancomycin, to cover even highly penicillin-resistant strains. Dexamethasone (a corticosteroid) given before or with the first antibiotic dose has been shown to reduce the risk of severe hearing loss and other neurological complications in pneumococcal meningitis in adults, and is now standard of care in high-income countries. Treatment duration for meningitis is typically 10–14 days.
Multidrug resistance is an increasing concern: some strains are resistant to penicillin, macrolides, and tetracyclines simultaneously, leaving fluoroquinolones as the main remaining oral options. The CDC has classified drug-resistant S. pneumoniae as a "serious threat" requiring surveillance and stewardship. Vaccination, which reduces the total number of pneumococcal infections, is therefore also an antibiotic stewardship intervention.
Vaccines — PCV15, PCV20, and PPSV23
Pneumococcal vaccines are one of public health's genuine success stories. Two types are available:
Conjugate vaccines (PCVs)
Pneumococcal conjugate vaccines attach capsular polysaccharides to a carrier protein, which converts them from a form that only stimulates short-lived antibody responses to one that stimulates long-lived immune memory (T-cell-dependent immunity). This makes them highly effective in infants and young children, who respond poorly to plain polysaccharide vaccines. PCV7 (7 serotypes, introduced in the US in 2000) dramatically reduced invasive pneumococcal disease in children and, through herd protection, in adults. PCV13 expanded to 13 serotypes and produced further reductions. The most recent formulations are PCV15 (15 serotypes) and PCV20 (20 serotypes), approved in the US in 2021 and now recommended for adults aged 65 and older and for younger adults with certain underlying conditions. The broader serotype coverage of PCV20 is intended to capture the non-vaccine serotypes that have emerged through serotype replacement.
PPSV23 (Pneumovax 23)
The polysaccharide vaccine PPSV23 covers 23 serotypes but, because it is not conjugated, produces a shorter-lived response that does not generate lasting memory. It is less effective in children under two years old and in people with impaired immune systems. It is still used in some situations, particularly as a follow-up to conjugate vaccination in high-risk adults to extend serotype coverage. Guidelines on the precise sequencing of PCV and PPSV23 in adults have evolved over the years as the conjugate vaccine options have expanded.
The effect of childhood conjugate vaccination programs has been striking. In the US, invasive pneumococcal disease rates in children under five fell by more than 75% after the introduction of PCV7 and PCV13. Deaths from pneumococcal meningitis in children declined by similar magnitudes. These reductions also cascaded to unvaccinated adults through herd protection, as children are the main reservoir for pneumococcal spread. Vaccination remains the most powerful tool available against this pathogen.
Research Papers
- Determination of Serotypes and Antibiotic Resistance in Streptococcus pneumoniae. Annals of Clinical and Analytical Medicine. 2015;6. doi:10.4328/jcam.3548 — Characterized the distribution of serotypes and patterns of antibiotic resistance in clinical pneumococcal isolates, illustrating the epidemiology of multidrug-resistant strains.
- Kumar K. Circulating Serotypes and Trends in Antibiotic Resistance of Invasive Streptococcus pneumoniae from Children under Five in Bangalore. Journal of Clinical and Diagnostic Research. 2013. doi:10.7860/jcdr/2013/6384.3741 — Documented the serotype distribution and rising antibiotic resistance among invasive pediatric pneumococcal isolates in India, with relevance to vaccine formulation for the developing world.
- Dobay O, et al. Antibiotic susceptibility and serotypes of Streptococcus pneumoniae isolates from Hungary. Journal of Antimicrobial Chemotherapy. 2003;51(4):887–893. doi:10.1093/jac/dkg171 — Provided surveillance data on penicillin resistance and serotype distribution in European pneumococcal isolates, helping map the landscape before widespread PCV13 introduction.
- Waraich HN, Haq I, Abdullah S. A Rare Case of Invasive Pneumococcal Disease Presenting With Pneumonia, Meningitis, Septic Arthritis, and Cerebral Infarcts. Cureus. 2025. doi:10.7759/cureus.99715 — A striking case report documenting the multi-organ invasive potential of the pneumococcus, illustrating the spectrum of simultaneous manifestations that can occur in vulnerable hosts.
- Marrie TJ. Bacteremic Pneumococcal Pneumonia Mortality Rate. Chest. 1993;103(3):658–660. doi:10.1378/chest.103.3.658 — Quantified the substantially elevated mortality rate of pneumococcal pneumonia when bacteremia is present, establishing a key benchmark for the severity of invasive disease.
Connections
- All Bacteria
- Pulmonology Conditions
- Neurology Conditions
- All Conditions
- Pneumonia
- Infectious Disease
- Meningitis — the general disease page for the infection this bacterium causes most lethally in adults.