Antibiotics for Pneumococcal Infections: Beta-Lactams and Alternatives
When your doctor says you have a pneumococcal infection — whether that is community-acquired pneumonia, a bloodstream infection, or bacterial meningitis — the antibiotic choice matters enormously. Streptococcus pneumoniae was once reliably killed by penicillin, but resistance has changed the landscape. Today, the right drug depends on where you caught the infection, how severe it is, what your allergy history looks like, and the local resistance patterns in your community. This page walks through the main antibiotic options in plain language, including how they work, typical doses, and when your doctor might choose one over another.
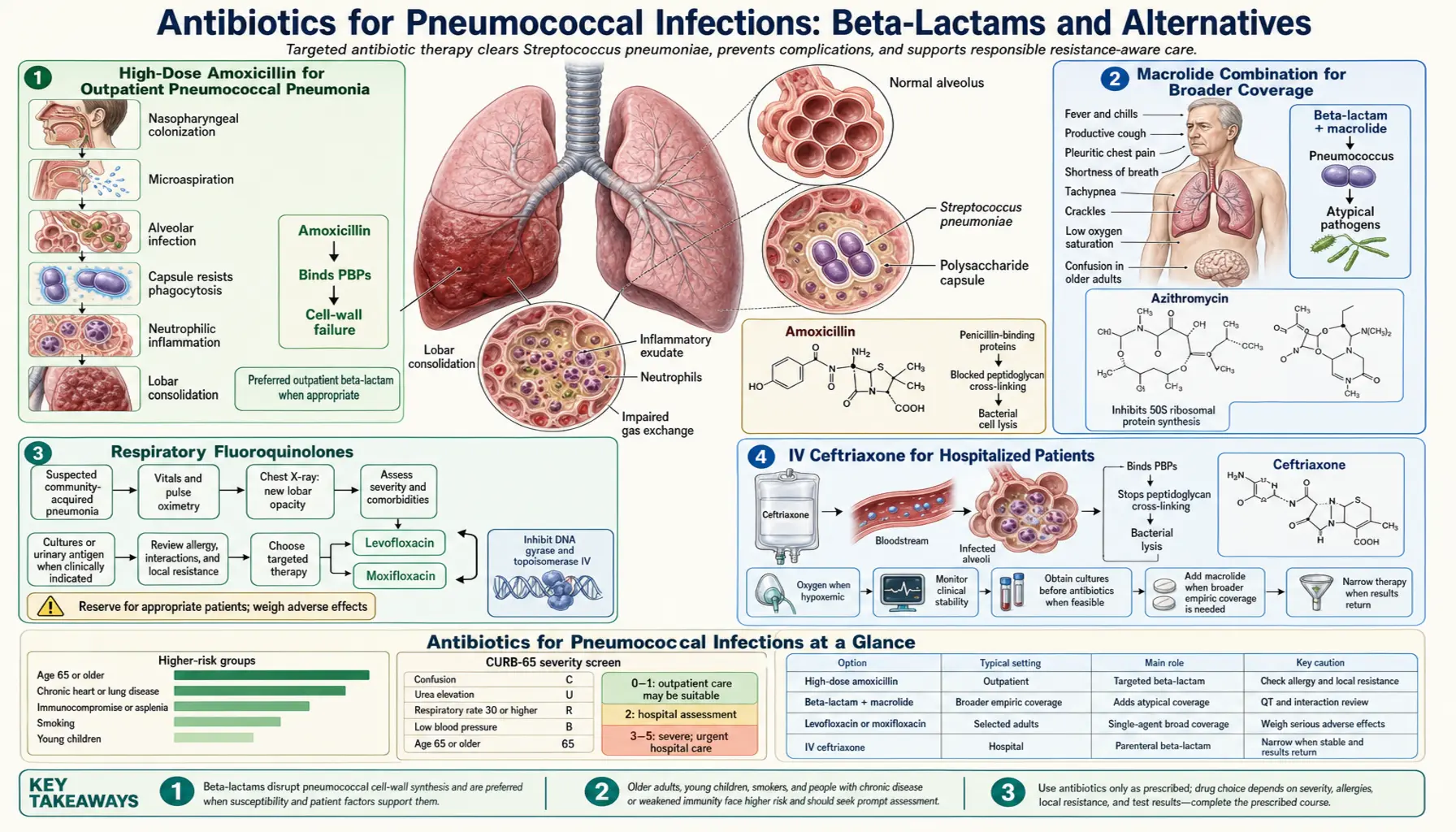
- High-Dose Amoxicillin for Outpatient Pneumonia
- Macrolide Combination for Broader Coverage
- Respiratory Fluoroquinolones
- IV Ceftriaxone for Hospitalized Patients
- Antibiotics for Pneumococcal Meningitis
- When Vancomycin Is Needed
- IV to Oral Step-Down Therapy
- Managing Penicillin Allergy
- Key Research Papers
High-Dose Amoxicillin for Outpatient Pneumococcal Pneumonia
If you are generally healthy, your doctor diagnoses you with community-acquired pneumonia, and you are well enough to stay home, the most likely prescription is amoxicillin 1 gram taken three times a day (TID) for five days. This is the cornerstone recommendation from the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) for outpatient pneumonia in patients without significant comorbidities and in areas where macrolide resistance is high.
Why such a high dose? Standard amoxicillin doses used for ear infections (500 mg twice daily) are often not enough to reliably kill S. pneumoniae strains that have developed intermediate resistance to penicillin-class drugs. These strains are not fully resistant — they can still be killed — but they require higher drug concentrations for longer periods.
Beta-lactam antibiotics like amoxicillin work through what pharmacologists call time-dependent killing. Unlike some antibiotics where a very high peak concentration kills bacteria, amoxicillin needs to maintain its concentration above the bacteria's minimum inhibitory concentration (MIC) for more than 50% of each dosing interval. The high 1-gram dose achieves this by pushing drug levels well above the MIC for intermediate-resistant strains throughout most of the six-to-eight hours between doses.
Amoxicillin has a practical advantage over the older oral penicillin V: it can be taken with food without losing effectiveness, making it much easier to tolerate three times a day. It is also inexpensive, widely available as a generic, and has a well-established safety record over decades of use.
Five days of treatment is typically sufficient for outpatient pneumonia in otherwise healthy adults. Longer courses do not appear to improve outcomes and increase the risk of side effects and disruption of your gut microbiome.
Macrolide Combination for Broader Coverage
If you are older, have chronic lung disease, diabetes, heart failure, kidney disease, or other significant health conditions, your doctor may prescribe amoxicillin plus a macrolide antibiotic rather than amoxicillin alone. The reason is that older patients and those with chronic illnesses are at higher risk for infections with so-called "atypical" bacteria — organisms like Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila — that do not respond to amoxicillin at all.
The two most common combinations are:
- Amoxicillin 1g TID plus azithromycin — azithromycin 500 mg on day 1, then 250 mg on days 2 through 5. Azithromycin's long half-life means it lingers in lung tissue for days after the last dose, which is why this shorter schedule works.
- Amoxicillin 1g TID plus clarithromycin — clarithromycin 500 mg twice daily for seven days. Clarithromycin has slightly better tissue penetration for some organisms but requires a longer course and twice-daily dosing.
An important caveat: macrolide resistance in S. pneumoniae is now 20 to 30% in many parts of the United States and higher in some regions of Asia and Europe. This means that if you have confirmed pneumococcal pneumonia and your doctor prescribes azithromycin alone (without amoxicillin), there is a meaningful chance the drug will not kill your specific bacterial strain. Macrolide monotherapy for pneumococcal pneumonia is therefore no longer recommended as a primary approach in most current guidelines. The macrolide in the combination serves mainly to cover atypicals — the amoxicillin handles the pneumococcus.
Macrolide side effects are usually mild — nausea, stomach cramps, diarrhea — and typically resolve within days of finishing the course. Azithromycin and clarithromycin can prolong the heart's QT interval (a measure of electrical activity), so patients with certain heart rhythm abnormalities or those taking other QT-prolonging drugs should flag this with their prescriber.
Respiratory Fluoroquinolones
Two antibiotics in the fluoroquinolone class — levofloxacin and moxifloxacin — are sometimes called "respiratory fluoroquinolones" because they cover virtually all the bacteria that cause community-acquired pneumonia in a single pill. Both also work for pneumococcal infections including penicillin-resistant strains, atypical organisms, and Haemophilus influenzae.
- Levofloxacin 750 mg once daily for 5 days — the higher dose over a shorter course has replaced the older 500 mg for 10 days schedule in most guidelines.
- Moxifloxacin 400 mg once daily for 5 days — slightly broader anaerobic coverage but cannot be used for urinary tract infections (poor urinary excretion).
These drugs work by blocking two bacterial enzymes — DNA gyrase and topoisomerase IV — that S. pneumoniae needs to copy and repair its DNA. Because this mechanism is entirely different from beta-lactams, fluoroquinolones retain activity against many penicillin-resistant strains.
When are respiratory fluoroquinolones preferred?
- True penicillin allergy (not just a reported rash, but confirmed allergy)
- Failed initial beta-lactam therapy
- High suspicion of macrolide-resistant pneumococcus
- Severe or moderately severe outpatient pneumonia requiring broad coverage
However, fluoroquinolones are not first-line for healthy young adults with straightforward pneumonia. Overusing them accelerates resistance not only in pneumococcus but also in other bacteria. Guidelines recommend "preserving" fluoroquinolones for patients who genuinely need them.
The most important safety warning is tendon rupture, particularly of the Achilles tendon. The risk is low overall but higher in people over 60, those taking corticosteroids, and people with kidney disease. Stop the antibiotic and contact your doctor immediately if you develop sudden tendon pain or swelling while taking a fluoroquinolone. They can also cause changes in blood sugar levels (important for people with diabetes), and in rare cases, they have been linked to peripheral neuropathy and worsening of myasthenia gravis.
IV Ceftriaxone for Hospitalized Patients
When your pneumococcal infection is severe enough to require hospital admission — you have low oxygen levels, high fever, confusion, or very low blood pressure — your treatment switches from oral pills to intravenous (IV) antibiotics. The standard choice for most hospitalized patients with community-acquired pneumonia is ceftriaxone, a third-generation cephalosporin given as an IV infusion.
Typical dose: 1 to 2 grams IV once daily. Like amoxicillin, ceftriaxone is a beta-lactam — it kills bacteria by blocking the enzyme transpeptidase, which is essential for building the bacterial cell wall. Without a functional cell wall, the bacterium lyses and dies. Ceftriaxone binds the penicillin-binding proteins (PBPs) that S. pneumoniae uses to construct this wall, but it does so with enough affinity to overcome intermediate-level penicillin resistance.
Ceftriaxone has several practical advantages that make it the go-to choice for hospitalized patients:
- Once-daily dosing — easier for nursing staff to administer and more comfortable for patients than antibiotics requiring every-6-hour infusions.
- Excellent tissue penetration — reaches good concentrations in the lungs, bloodstream, and (at higher doses) the cerebrospinal fluid surrounding the brain and spinal cord.
- Broad coverage — handles S. pneumoniae, H. influenzae, many gram-negative bacteria, and some anaerobes in a single drug.
- Long track record — used in clinical practice for decades with well-understood side effects (mainly diarrhea, rash, and in rare cases, biliary sludging with prolonged use).
For hospitalized patients who also need atypical coverage (the same logic as outpatient combination therapy), a macrolide — typically azithromycin given IV or orally — is added alongside ceftriaxone. Once you are clearly improving — fever gone for more than 24 hours, oxygen saturation normal breathing room air, able to eat and drink — your medical team will switch you to oral antibiotics and, if stable, discharge you to finish the course at home.
Antibiotics for Pneumococcal Meningitis
Pneumococcal meningitis — infection of the membranes surrounding the brain — is a medical emergency requiring immediate IV antibiotics. The treatment approach is more aggressive than for pneumonia because the antibiotic must penetrate the blood-brain barrier and reach therapeutic concentrations in the cerebrospinal fluid (CSF), which is much harder than reaching the lungs.
Standard empiric regimen while awaiting culture and sensitivity results:
- Ceftriaxone 2g IV every 12 hours (4g per day total — double the pneumonia dose). The higher dose is necessary because the blood-brain barrier substantially limits how much drug gets into the CSF. Only at this higher dose can ceftriaxone maintain concentrations in the CSF above the MIC of typical pneumococcal strains throughout the dosing interval.
- Vancomycin 15–20 mg/kg IV every 8–12 hours added empirically. This is because before you have culture results, you cannot know whether your patient's S. pneumoniae strain is highly penicillin-resistant. If it is, ceftriaxone alone may fail. Vancomycin covers this gap.
- Dexamethasone 0.15 mg/kg IV every 6 hours for 4 days — a corticosteroid started at the same time as (or just before) the first antibiotic dose. This is one of the most important developments in meningitis treatment of the past two decades. The landmark 2002 NEJM trial by de Gans and van de Beek showed that dexamethasone reduced the risk of death and severe neurological complications in adults with bacterial meningitis, particularly pneumococcal meningitis. The mechanism: dexamethasone dampens the intense inflammatory response triggered when bacteria die and release their cell contents — it is this inflammation, not the bacteria themselves, that causes most of the brain damage. Dexamethasone must be given before or with the first antibiotic dose to be effective; giving it hours later after inflammation is already in full swing provides much less benefit.
Duration: Pneumococcal meningitis is treated for 10 to 14 days — significantly longer than pneumonia — because eliminating the bacteria from the CSF takes longer, and under-treatment raises the risk of relapse.
Rifampicin as an add-on: Some protocols, particularly in Europe, add rifampicin to the ceftriaxone-plus-vancomycin regimen for pneumococcal meningitis caused by highly resistant strains. Rifampicin penetrates the CSF exceptionally well and synergizes with ceftriaxone against resistant pneumococcus. It is not universally adopted in US guidelines but may be used in severe cases.
When Vancomycin Is Needed
Vancomycin is a glycopeptide antibiotic — completely different in structure and mechanism from the beta-lactams. It kills bacteria by binding to the D-Ala-D-Ala terminus of peptidoglycan precursors — essentially blocking the raw material that bacteria use to assemble their cell wall, at an entirely different step than where penicillin acts. This means vancomycin can kill S. pneumoniae strains that have become resistant to penicillin and cephalosporins by altering their penicillin-binding proteins (PBPs).
When is vancomycin used for pneumococcal infections?
- Pneumococcal meningitis (empirically, as described above, until susceptibilities are known)
- Highly penicillin-resistant S. pneumoniae — defined as an MIC of ≥2 mcg/mL for penicillin in non-meningitis infections, or ≥0.12 mcg/mL for meningitis (the brain requires much stricter standards)
- Failure of initial beta-lactam therapy with documented resistant organism
- Serious pneumococcal infections in geographic regions with high rates of resistance
Geographic variability: Highly penicillin-resistant pneumococcus is not equally distributed around the world. Rates are higher in parts of Asia (particularly South Korea and some areas of Southeast Asia), Spain, Eastern Europe, and some US states — notably those with higher antibiotic use. Your doctor's decision to add vancomycin empirically may reflect what strains are circulating in your community.
Vancomycin requires IV administration and careful monitoring of kidney function and drug blood levels ("vancomycin troughs" or AUC monitoring). Side effects include kidney toxicity (nephrotoxicity), hearing problems (ototoxicity) with high levels, and the "red man syndrome" — a flushing reaction during rapid infusion that is not a true allergy but can be alarming. Slowing the infusion rate usually prevents it.
Linezolid — an oxazolidinone antibiotic — serves as a second reserve agent for vancomycin-resistant situations or when vancomycin cannot be used due to kidney problems. Linezolid penetrates the CSF well and has good oral bioavailability. However, it is expensive and carries risks of bone marrow suppression with prolonged use. It is not a first-choice antibiotic for pneumococcal infections but provides an important backup option.
IV to Oral Antibiotic Step-Down Therapy
One of the most well-supported advances in pneumonia management over the past 20 years is the practice of switching from IV to oral antibiotics early — as soon as the patient shows signs of improvement — rather than completing the entire course via IV drip in the hospital. This is called step-down therapy.
Criteria for switching to oral antibiotics (all four should be met):
- Temperature normal for more than 24 hours (no fever)
- Oxygen saturation normal on room air (not needing supplemental oxygen)
- Able to eat, drink, and take oral medications without vomiting
- Not bacteremic — blood cultures negative (if drawn and resulted)
When these criteria are met — often by day 2 or 3 in the hospital for patients with pneumonia — switching to oral antibiotics is as effective as continuing IV therapy. The evidence from multiple randomized trials shows no difference in cure rates, recurrence, or mortality, but significant benefits in patient experience and cost.
What oral antibiotic is used for step-down?
- Amoxicillin 1g TID — the oral equivalent of ceftriaxone for susceptible strains
- Oral levofloxacin or moxifloxacin — if the patient started on IV levofloxacin, or if penicillin allergy is an issue
- Oral amoxicillin-clavulanate for patients with additional concerns about resistant organisms or aspiration pneumonia
Total treatment duration: The evidence increasingly supports 5 days total for community-acquired pneumonia in patients who respond well to treatment (rather than the older standard of 7 to 10 days). The IDSA/ATS guidelines recommend treatment until the patient has been afebrile for 48 to 72 hours, which in practice often means 5 days total. Longer courses are reserved for complicated infections, bacteremia, or poor initial response. Shorter, more targeted antibiotic courses reduce side effects, lower the risk of Clostridioides difficile colitis (a serious antibiotic-related gut infection), and slow the development of resistance.
Managing Penicillin Allergy
About one in ten patients tell their doctor they are allergic to penicillin — but studies consistently show that more than 90% of those people are not actually allergic when formally tested. This matters because many patients unnecessarily receive second-line antibiotics (like vancomycin or fluoroquinolones) for their entire lives, leading to worse outcomes and contributing to antibiotic resistance.
Why so many false penicillin allergy labels?
- A rash during childhood amoxicillin treatment — the most common scenario. Most of these rashes are a viral exanthem (a skin reaction caused by the underlying viral infection the amoxicillin was treating, not the drug itself). Only a small percentage are true allergic reactions.
- Remote history with no documentation — "I was told as a child" without details about the reaction type.
- Family member's allergy incorrectly attributed to the patient.
- True allergy that has resolved over time — IgE-mediated penicillin allergy wanes in most people within 5 years, and over 80% of people who were truly allergic test negative after 10 years.
What is your doctor's approach if you report penicillin allergy?
- Mild reported reaction (rash without hives, no anaphylaxis history): Many clinicians will use cephalosporins such as ceftriaxone, since the cross-reactivity between penicillins and cephalosporins is much lower than historically believed — probably 1-2% at most. Sharing a beta-lactam ring does not mean sharing the side chains that trigger most allergic reactions.
- Confirmed anaphylaxis or severe IgE-mediated reaction: Avoid all beta-lactams. Use a respiratory fluoroquinolone (levofloxacin or moxifloxacin) for serious pneumococcal infections — this is the preferred alternative in guidelines.
- Mild disease with confirmed penicillin allergy: Azithromycin can be used for mild outpatient pneumonia, but only if macrolide susceptibility is likely — significant risk of failure given macrolide resistance rates.
- Penicillin allergy testing: If time allows (elective surgery, pre-procedure planning), formal allergy testing with skin test and oral challenge can de-label penicillin allergy in the majority of patients who report it. This "de-labeling" is increasingly recognized as one of the highest-value interventions in antimicrobial stewardship.
- Penicillin desensitization: For situations where penicillin or a related beta-lactam is truly the best option and the patient has a confirmed severe allergy, allergists can perform rapid desensitization under controlled conditions in a monitored setting.
If you carry a penicillin allergy label, ask your doctor whether formal allergy testing might be appropriate for you. Being de-labeled can meaningfully improve your future healthcare options.
Key Research Papers
The following studies form the evidence base for current antibiotic treatment guidelines for pneumococcal infections. All citations link to PubMed.
- Mandell LA, et al. IDSA/ATS Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin Infect Dis. 2007;44(Suppl 2):S27–S72. — Search PubMed — The foundational US guideline document. Establishes amoxicillin as first-line for outpatient CAP, defines combination therapy criteria, and sets hospitalization thresholds.
- Wunderink RG, Waterer GW. Community-Acquired Pneumonia. N Engl J Med. 2014;370:543–551. — Search PubMed — Comprehensive clinical review covering pathogenesis, diagnosis, and treatment decisions including antibiotic selection and step-down therapy.
- de Gans J, van de Beek D. Dexamethasone in Adults with Bacterial Meningitis. N Engl J Med. 2002;347:1549–1556. — Search PubMed — Landmark randomized trial demonstrating that dexamethasone given before or with the first antibiotic dose significantly reduced death and neurological complications in adults with bacterial meningitis, especially pneumococcal.
- Brouwer MC, et al. Epidemiology, Diagnosis, and Antimicrobial Treatment of Acute Bacterial Meningitis. Clin Microbiol Rev. 2010;23:467–492. — Search PubMed — Detailed review of meningitis treatment protocols including ceftriaxone dosing, vancomycin use, and dexamethasone timing across different bacterial pathogens.
- Musher DM, Thorner AR. Community-Acquired Pneumonia. N Engl J Med. 2014;371:1619–1628. — Search PubMed — Clinical review emphasizing the importance of identifying pneumococcal pneumonia specifically and selecting antibiotics accordingly, including the limitations of macrolide monotherapy.
- Musher DM, et al. Pneumococcal Pneumonia. Lancet. 2012;380:1282–1292. — Search PubMed — Comprehensive review of pneumococcal pneumonia epidemiology, bacteriology, and treatment including mechanisms of beta-lactam resistance and treatment failure.
- Doern GV, et al. Antimicrobial Resistance Among Clinical Isolates of Streptococcus pneumoniae in the United States. Clin Infect Dis. 2001;32:S16–S23. — Search PubMed — Seminal US resistance surveillance data establishing macrolide resistance rates and the rationale for moving away from macrolide monotherapy.
- Pletz MW, et al. Antibiotic Therapy of Community-Acquired Pneumonia. Eur J Clin Microbiol Infect Dis. 2011;30:457–465. — Search PubMed — Comparison of beta-lactam monotherapy versus beta-lactam plus macrolide combination for CAP, addressing the question of whether combination therapy improves outcomes over beta-lactam alone.
- van de Beek D, et al. Clinical Features and Prognostic Factors in Adults with Bacterial Meningitis. N Engl J Med. 2004;351:1849–1859. PMID 15509818 — Large Dutch cohort study identifying prognostic factors in adult bacterial meningitis and outcomes by antibiotic regimen.
- Lynch JP 3rd, Zhanel GG. Streptococcus pneumoniae: Epidemiology and Risk Factors, Evolution of Antimicrobial Resistance, and Impact of Vaccines. Curr Opin Pulm Med. 2010;16:217–225. — Search PubMed — Overview of how pneumococcal resistance developed, geographic distribution of resistance, and how vaccine programs have affected which strains now cause disease.
- Musher DM. Infections Caused by Streptococcus pneumoniae: Clinical Spectrum, Pathogenesis, Immunity, and Treatment. Clin Infect Dis. 1992;14:801–809. PMID 1576274 — Classic foundational paper establishing the clinical spectrum of pneumococcal disease and the pharmacological basis for penicillin-class therapy.
For the most current treatment recommendations, search PubMed for Streptococcus pneumoniae antibiotic treatment guidelines.
Connections
- Streptococcus Pneumoniae Overview
- Treatment & Prevention Hub
- Antibiotic Resistance in S. pneumoniae
- Meningitis & Invasive Pneumococcal Disease
- Community-Acquired Pneumonia
- All Bacteria
- Meningitis — bacterial meningitis from all causes: why the drug must cross the blood-brain barrier and reach the CSF, not just the lungs.