Diagnosing Pneumococcal Infections: Cultures, Antigen Tests, and Imaging
When a doctor suspects a pneumococcal infection, several tests work together to confirm the diagnosis, identify the exact strain, and guide treatment decisions. No single test is perfect on its own — understanding what each one reveals (and what it misses) helps you make sense of what your care team is ordering and why timing matters so much.
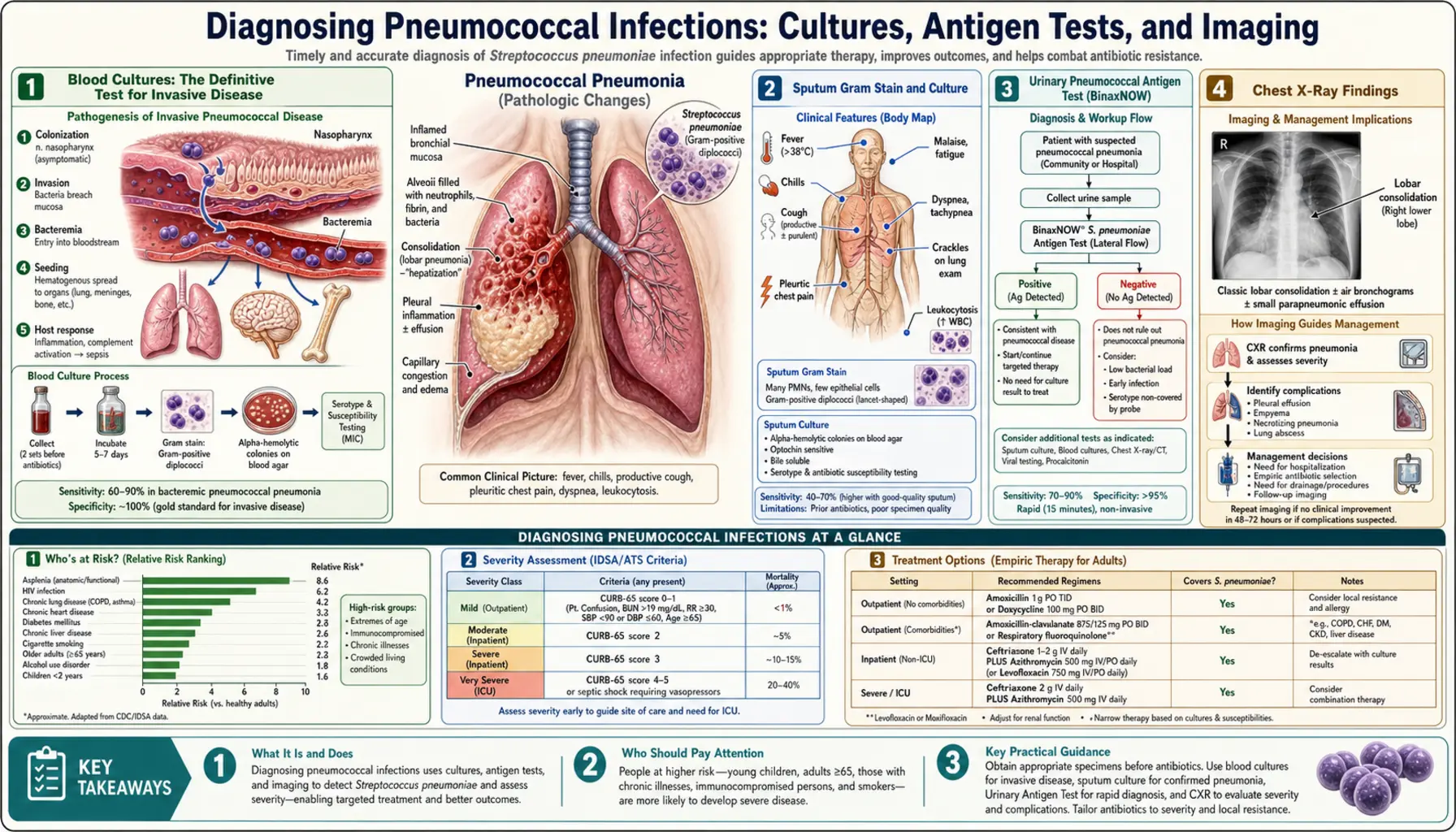
- Blood Cultures: The Definitive Test for Invasive Disease
- Sputum Gram Stain and Culture
- Urinary Pneumococcal Antigen Test (BinaxNOW)
- Chest X-Ray Findings
- CT Chest for Complex Cases
- Lumbar Puncture for Suspected Meningitis
- Procalcitonin and CRP: Inflammatory Markers
- When to Treat Before Tests Are Complete
- Key Research Papers
- Connections
Blood Cultures: The Definitive Test for Invasive Disease
A blood culture is the gold standard for proving that Streptococcus pneumoniae has entered the bloodstream — a condition called bacteremia. When the blood culture grows pneumococcus, there is no doubt about the diagnosis, and you get a definitive answer about which antibiotics will work.
The catch is that blood cultures are positive in only about 25% of people hospitalized with community-acquired pneumonia. This means three out of four patients with genuine pneumococcal pneumonia will have negative blood cultures. A negative result does not rule out the infection — it simply means the bacteria are not circulating in detectable numbers in the blood at that moment.
Proper collection technique matters enormously. Doctors draw two separate sets of cultures from two different sites on your body — usually one from each arm — to reduce the chance of false-positive results from skin bacteria that accidentally contaminate the sample. Each set contains two bottles: one that grows bacteria in the presence of oxygen (aerobic) and one without (anaerobic). This gives the lab four bottles total, increasing the sensitivity of detection.
The most important rule: blood cultures must be drawn before the first antibiotic dose. Even one dose of antibiotics can suppress bacterial growth enough to render the culture negative for days. Drawing blood cultures adds only about five minutes to your care, but the information they provide — particularly the antibiotic sensitivity profile — can save your life or shorten your hospital stay significantly.
Modern hospital laboratories use automated blood culture systems, most commonly the BACTEC or BacT/Alert platforms. These machines monitor the bottles every ten minutes, detecting carbon dioxide released by growing bacteria. Most positive cultures are flagged within 24 to 48 hours. A preliminary Gram stain result can come back even sooner — sometimes within hours — giving doctors an early look at whether the bacteria are gram-positive cocci (consistent with pneumococcus) before the full culture result is ready.
While you are waiting for culture results, your doctor will not sit on their hands. Empiric antibiotic treatment — starting a broad-spectrum antibiotic based on the most likely bacteria — begins immediately in seriously ill patients. This is not guessing; it is evidence-based standard of care. Once culture results return (usually within two days), the antibiotic is often narrowed to a more targeted option, a process called de-escalation.
Sputum Gram Stain and Culture
Sputum is the mucus you cough up from deep in your lungs. Unlike saliva (which comes from your mouth), a good sputum sample comes from the bronchi and carries bacteria directly from the site of infection. Analyzing sputum under a microscope and growing it in the lab can identify pneumococcus and test its antibiotic sensitivities.
Timing is everything. The ideal sputum sample is collected before antibiotics are started and preferably before the patient rinses their mouth or brushes their teeth, which would wash away bacteria and dilute the sample. A patient who has already received several doses of antibiotics will usually produce a sputum culture that grows nothing, even if pneumococcus is genuinely causing the infection.
Laboratory technicians assess quality before proceeding with culture. Under the microscope, a good-quality sputum sample shows fewer than 10 squamous epithelial cells per low-power field (these are mouth cells indicating the sample is too contaminated by saliva) and at least 25 neutrophils per low-power field (these are the white blood cells rushing to fight the infection, confirming the sample came from inflamed lung tissue). A sample that fails these criteria is rejected and a new one requested.
The Gram stain appearance of pneumococcus is distinctive: pairs of oval bacteria (diplococci) shaped like the bottom of a football or a lance tip, staining dark purple (gram-positive), often surrounded by clusters of neutrophils trying to engulf them. An experienced microbiologist who sees this pattern in a quality sputum sample can call a presumptive diagnosis of pneumococcal pneumonia within an hour.
Sputum culture sensitivity for pneumococcus ranges from about 40% to 60% — meaning it misses the diagnosis in nearly half of cases, particularly in patients who cannot produce a good deep cough, who have already started antibiotics, or who have partially treated disease. However, when the culture is positive, the specificity is high, and critically, the culture provides antibiotic susceptibility testing that the urinary antigen test cannot offer.
Urinary Pneumococcal Antigen Test (BinaxNOW)
The BinaxNOW pneumococcal urinary antigen test has become one of the most widely used rapid diagnostic tools in hospital emergency departments and wards. It detects a specific protein from the pneumococcal capsule — the outer coating of the bacterium — that is shed into the urine during infection and remains there even after antibiotic treatment has started.
This last point is the test's greatest advantage over cultures. If you arrive at the hospital having already taken two days of antibiotics prescribed by your primary care doctor, blood cultures and sputum cultures will almost certainly be negative. But the urinary antigen test will still be positive, because the capsular material continues to be filtered through the kidneys long after the bacteria themselves have been killed. This makes the test valuable for confirming a clinical suspicion when cultures have been rendered useless by prior antibiotic use.
The test works like a pregnancy test: a strip is dipped into a urine sample, and a result appears as a colored line within 15 minutes. Results in published studies show sensitivity between 70% and 80% for pneumococcal pneumonia (meaning it correctly identifies 7 to 8 out of every 10 true cases) and specificity between 90% and 97% (meaning false positives are uncommon). A positive result strongly supports the diagnosis and is accepted as sufficient evidence for pneumococcal diagnosis in most clinical guidelines.
There are important limitations to understand. First, the test detects the presence of pneumococcal antigen but cannot tell you which serotype is responsible or whether the organism is resistant to penicillin or other antibiotics — that information still requires culture. Second, some studies have documented false-positive results in young children who are colonized with pneumococcus in their throat without being ill, though this is less of a concern in adults. Third, the test may remain positive for weeks after a resolved infection, which can cause confusion in patients re-presenting with new symptoms.
Current guidelines from the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) recommend urinary antigen testing for all patients hospitalized with severe community-acquired pneumonia, in addition to blood cultures. For outpatient pneumonia, routine testing is generally not recommended because it would not change management — treatment is empiric regardless of result.
Chest X-Ray Findings
A chest X-ray is usually the first imaging test ordered when pneumonia is suspected, and it plays a central role in both diagnosing the infection and assessing its extent. Pneumococcal pneumonia has a classic radiographic appearance that distinguishes it from other types of lung infection, though no pattern is unique enough to be diagnostic on its own.
The hallmark finding is lobar consolidation — one or more entire lobes of the lung filled with inflammatory fluid and pus, appearing as a dense white area on the X-ray. Unlike the patchy, scattered shadows seen with atypical organisms like Mycoplasma pneumoniae, pneumococcal pneumonia tends to occupy a defined lobe with a sharp border. You may see the entire right lower lobe, for example, appearing white against the darker (air-filled) surrounding tissue.
Within this white area, the airways (bronchi) often remain open and appear as dark streaks — a finding called air bronchograms. Seeing air bronchograms within a consolidation is important because it confirms the density is actually lung tissue filled with fluid, not a solid mass or a collapsed airway. This pattern strongly suggests an air-space infection like bacterial pneumonia rather than a tumor.
Pleural effusion — fluid collecting between the lung and the chest wall — appears as a white crescent at the base of the lung. Small effusions are common in pneumococcal pneumonia (called para-pneumonic effusions) and usually resolve with antibiotic treatment. Larger effusions, or those that become infected (empyema), require drainage and indicate more serious disease.
Early in the illness — within the first 12 to 24 hours — the chest X-ray can appear completely normal even when the patient is clearly unwell. This is because the consolidation needs time to fully develop. If your first X-ray is negative but symptoms are consistent with pneumonia, a repeat film 24 to 48 hours later often reveals the changes. CT scanning, described below, is far more sensitive in this early window.
Comparing pneumococcal X-ray patterns to other common causes helps: Mycoplasma pneumonia typically shows patchy, bilateral interstitial infiltrates without consolidation (the so-called "walking pneumonia" appearance); Staphylococcal pneumonia can show cavitation — holes developing within the consolidation — which is unusual with pneumococcus; Legionella can look identical to pneumococcal pneumonia on X-ray, which is why antigen testing for both is recommended in hospitalized patients.
CT Chest for Complex Cases
Computed tomography (CT) of the chest is not required for straightforward pneumococcal pneumonia, but it becomes essential when the clinical picture is complicated or when plain X-ray findings do not match the severity of symptoms.
CT is significantly more sensitive than plain chest X-ray, detecting early consolidation that is not yet visible on the plain film. In patients with severe pneumonia or a rapidly deteriorating course, CT provides a much clearer picture of which lung segments are involved and whether complications are developing. A finding that appears to be a simple effusion on X-ray might reveal on CT to be a loculated empyema (a collection of pus walled off by fibrous tissue) that requires surgical drainage rather than simple observation.
CT is particularly valuable for detecting lung abscess — a cavity filled with pus that develops when part of the consolidated lung breaks down. This complication is more common with aspiration pneumonia and Staphylococcal infections, but it can occur with pneumococcus, especially in patients with impaired immunity or delayed treatment. A lung abscess changes the antibiotic choice and duration significantly and sometimes requires bronchoscopy or percutaneous drainage.
In patients who fail to improve after several days of appropriate antibiotics, CT can identify explanations: a missed empyema, a second area of consolidation in a different lobe, or an obstructing lesion (such as a tumor) causing post-obstructive pneumonia behind it. CT-guided drainage procedures — where a radiologist uses CT images in real time to guide a needle or drain into a fluid collection — are some of the most important interventional uses of the technology in pneumonia management.
The main consideration in using CT is radiation exposure. A chest CT delivers significantly more radiation than a plain X-ray — roughly 100 times more. For a single acute illness, this is an entirely acceptable trade-off when the clinical information is needed. However, in patients who may need multiple scans over their illness or who are younger, the decision is made thoughtfully based on whether the result will genuinely change management.
Lumbar Puncture for Suspected Meningitis
When pneumococcal infection spreads to the brain and spinal cord, it causes meningitis — one of the most serious infections a person can develop. Diagnosing meningitis definitively requires examining the cerebrospinal fluid (CSF) that bathes the brain and spinal cord, which means performing a lumbar puncture (spinal tap).
A lumbar puncture is performed with the patient lying curled on their side or sitting and leaning forward, bending the spine to open the gaps between the vertebrae. A needle is inserted between two lower vertebrae (typically L3/L4 or L4/L5, well below where the spinal cord ends) and CSF is withdrawn. The procedure takes about 20 to 30 minutes. Patients often feel pressure rather than sharp pain, and most experience no serious complications. A headache in the days following is the most common side effect, caused by a small amount of CSF leaking through the puncture site.
The classic clinical triad that should prompt urgent consideration of lumbar puncture is: fever, neck stiffness (the patient cannot bring their chin to their chest without pain), and altered consciousness (confusion or drowsiness). Any two of these three findings in an adult patient justify rapid evaluation for meningitis.
However, a lumbar puncture should not be performed until a CT scan of the head has been done in patients who show signs that pressure inside the skull may be dangerously elevated. These signs include papilledema (swelling of the optic disc seen when a doctor looks into the eye with an ophthalmoscope), focal neurological findings (weakness on one side, speech problems), or significantly depressed consciousness. Performing a lumbar puncture when intracranial pressure is very high risks a catastrophic complication called brain herniation. In these patients, antibiotics are started immediately and CT is done first, with lumbar puncture following if no contraindication is found.
The CSF findings in pneumococcal meningitis are characteristic. The white blood cell count is typically very high — usually between 1,000 and 5,000 cells per microliter, predominantly neutrophils (the infection-fighting cells). By comparison, normal CSF has fewer than 5 white cells. The protein level is elevated, typically above 1 gram per liter (normal is less than 0.45 g/L), reflecting breakdown of the blood-brain barrier. The glucose level in the CSF is low, typically less than 50% of the blood glucose measured simultaneously (normal is around 60-70%), because the bacteria are consuming glucose for energy.
CSF Gram stain shows gram-positive diplococci in approximately 80% of untreated bacterial meningitis cases — a result that can come back within an hour and dramatically accelerates targeted treatment. CSF culture identifies the organism definitively and provides antibiotic sensitivities, though this takes 24 to 48 hours. In patients who have received antibiotics before the lumbar puncture, CSF culture sensitivity falls significantly. PCR testing of the CSF for pneumococcal DNA has become increasingly available and remains positive even when cultures are negative due to prior antibiotics, with sensitivity above 90% in specialized centers.
Procalcitonin and CRP: Inflammatory Markers
Procalcitonin (PCT) and C-reactive protein (CRP) are blood tests that measure how strongly your body's immune system is responding to infection. They do not identify which bacteria is causing the illness — but they are extremely useful for determining whether a bacterial infection is present at all, and for tracking your response to treatment.
Procalcitonin is a precursor to the hormone calcitonin, and it behaves unusually in infection. In healthy people, procalcitonin levels in the blood are essentially undetectable — below 0.1 micrograms per liter. In bacterial infections, levels rise dramatically within 6 to 12 hours of infection onset. A procalcitonin level above 0.25 micrograms per liter is generally considered the threshold suggesting bacterial infection; levels above 2.0 strongly suggest severe systemic bacterial infection. By contrast, viral infections cause only modest procalcitonin elevations — typically staying below 0.25 micrograms per liter — making the test useful for distinguishing bacterial from viral pneumonia when the clinical picture is unclear.
This distinction matters enormously for appropriate antibiotic use. Most respiratory infections are viral and do not benefit from antibiotics, but antibiotics cause side effects and contribute to antibiotic resistance when used unnecessarily. Several large randomized trials have demonstrated that using procalcitonin levels to guide antibiotic decisions — stopping antibiotics when levels fall rapidly, or withholding them when levels stay low — reduces antibiotic exposure by about 2 to 3 days without increasing mortality or treatment failure.
C-reactive protein is made by the liver in response to inflammatory signals released during infection. It rises more slowly than procalcitonin — reaching its peak at about 48 hours after infection onset — but it is measured in nearly every hospital laboratory worldwide and costs a fraction of procalcitonin testing. A CRP above 100 milligrams per liter strongly suggests bacterial pneumonia rather than a viral illness or non-infectious lung condition. CRP is also useful for monitoring response to treatment: levels should fall by 50% within 3 to 4 days of starting effective antibiotics. Failure to fall (or a rise after initial improvement) should trigger re-evaluation for complications like empyema or antibiotic resistance.
Neither procalcitonin nor CRP is specific to pneumococcus — they rise in any bacterial infection. They cannot replace cultures or antigen testing for identifying the causative organism. But they are invaluable tools in the diagnostic toolkit, particularly in the early hours of illness before culture results are available.
When to Treat Before Tests Are Complete
One of the most important principles in managing serious bacterial infections is this: collecting diagnostic samples and starting treatment happen simultaneously, not sequentially. Waiting for laboratory results before starting antibiotics in a seriously ill patient is dangerous and is not the standard of care.
The reason is timing. In pneumococcal bacteremia and meningitis, mortality rises measurably with every hour of antibiotic delay. A landmark study of bacterial meningitis found that patients who received antibiotics within 3 hours of hospital arrival had significantly better survival and neurological outcomes than those in whom treatment was delayed, even by a few hours. The bacteria are not waiting for lab results.
Practically, this means the sequence looks like this in a seriously ill patient: blood cultures are drawn in about 5 minutes, the patient is taken for imaging, a lumbar puncture is performed if meningitis is suspected (another 20 to 30 minutes), and antibiotics are running into the IV within the hour. The laboratory processes samples while treatment is already underway. For straightforward community-acquired pneumonia that is not life-threatening, doctors have slightly more latitude, but even here the IDSA/ATS guidelines recommend initiating antibiotics within 4 hours of hospital admission.
The antibiotic started before results return is empiric — it is chosen based on which bacteria most commonly cause this type of infection in this type of patient. For community-acquired pneumonia requiring hospitalization, this typically means a beta-lactam antibiotic (such as ceftriaxone) combined with a macrolide (such as azithromycin) to cover both pneumococcus and atypical organisms. For suspected bacterial meningitis, empiric therapy covers the most dangerous organisms: ceftriaxone for pneumococcus and Neisseria meningitidis, plus ampicillin for Listeria in older adults and immunocompromised patients, plus dexamethasone (a steroid) given before or with the first antibiotic dose to reduce brain inflammation.
Once culture results and antibiotic sensitivities return — usually within 48 hours — the treatment is refined. If the blood culture grows penicillin-sensitive pneumococcus, for example, the regimen can be de-escalated to penicillin alone, which is narrower, cheaper, and has fewer side effects. This stepdown approach is called antibiotic stewardship, and it depends entirely on having collected proper specimens before treatment started — which is why those first few minutes of specimen collection are so important even when everyone is rushed.
Key Research Papers
The following studies have shaped how pneumococcal infections are diagnosed and how diagnostic tests are used in practice.
- Mandell LA, et al. "Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults." Clinical Infectious Diseases. 2007;44(Suppl 2):S27–S72. — Search PubMed
- Wunderink RG, Waterer G. "Community-Acquired Pneumonia." New England Journal of Medicine. 2014;370(6):543–551. — Search PubMed
- Musher DM, Thorner AR. "Community-Acquired Pneumonia." New England Journal of Medicine. 2014;371(17):1619–1628. Also see Musher DM, 2012 Lancet review of pneumococcal pneumonia. — Search PubMed
- Lynch JP 3rd, Zhanel GG. "Streptococcus pneumoniae: Epidemiology and Risk Factors, Evolution of Antimicrobial Resistance, and Impact of Vaccines." Current Opinion in Pulmonary Medicine. 2010;16(3):217–225. — Search PubMed
- Brouwer MC, et al. "Epidemiology, Diagnosis, and Antimicrobial Treatment of Acute Bacterial Meningitis." Clinical Microbiology Reviews. 2010;23(3):467–492. — Search PubMed
- van de Beek D, et al. "Corticosteroids for Acute Bacterial Meningitis." Cochrane Database of Systematic Reviews. 2013;(6):CD004405. — Search PubMed
- de Gans J, van de Beek D. "Dexamethasone in Adults with Bacterial Meningitis." New England Journal of Medicine. 2002;347(20):1549–1556. — Search PubMed
- Marrie TJ, et al. "Community-Acquired Pneumonia Requiring Hospitalization: 5-Year Prospective Study." Medicine. 2018;97(34):e11984. — Search PubMed
- Bogaert D, de Groot R, Hermans PW. "Streptococcus pneumoniae Colonisation: The Key to Pneumococcal Disease." Lancet Infectious Diseases. 2004;4(3):144–154. — Search PubMed
- Musher DM. "Infections Caused by Streptococcus pneumoniae: Clinical Spectrum, Pathogenesis, Immunity, and Treatment." Clinical Infectious Diseases. 1992;14(4):801–809. See also Musher DM, 2000. — Search PubMed
- Sorde R, et al. "Current and Potential Usefulness of Pneumococcal Urinary Antigen Detection in Hospitalized Patients with Community-Acquired Pneumonia to Guide Antimicrobial Therapy." Archives of Internal Medicine. 2011;171(2):166–172. — Search PubMed
Connections
- All Bacteria
- Streptococcus Pneumoniae Overview
- Symptoms & Diagnosis Hub
- Pneumonia Symptoms and Severity
- Beta-Lactam and Antibiotic Treatment
- Lab Tests
- Pneumonia