Tuberculosis Symptoms and Diagnosis
Pulmonary TB Symptoms
The classic chest disease: productive cough, hemoptysis, night sweats, weight loss, and cavitary X-ray findings.
TB in Vulnerable Groups
How TB behaves differently in people with HIV, children, pregnant women, the elderly, and the immunosuppressed.
Diagnosis: Tests and Tools
Tuberculin skin test, IGRA blood tests, chest X-ray patterns, sputum culture, and GeneXpert molecular testing.
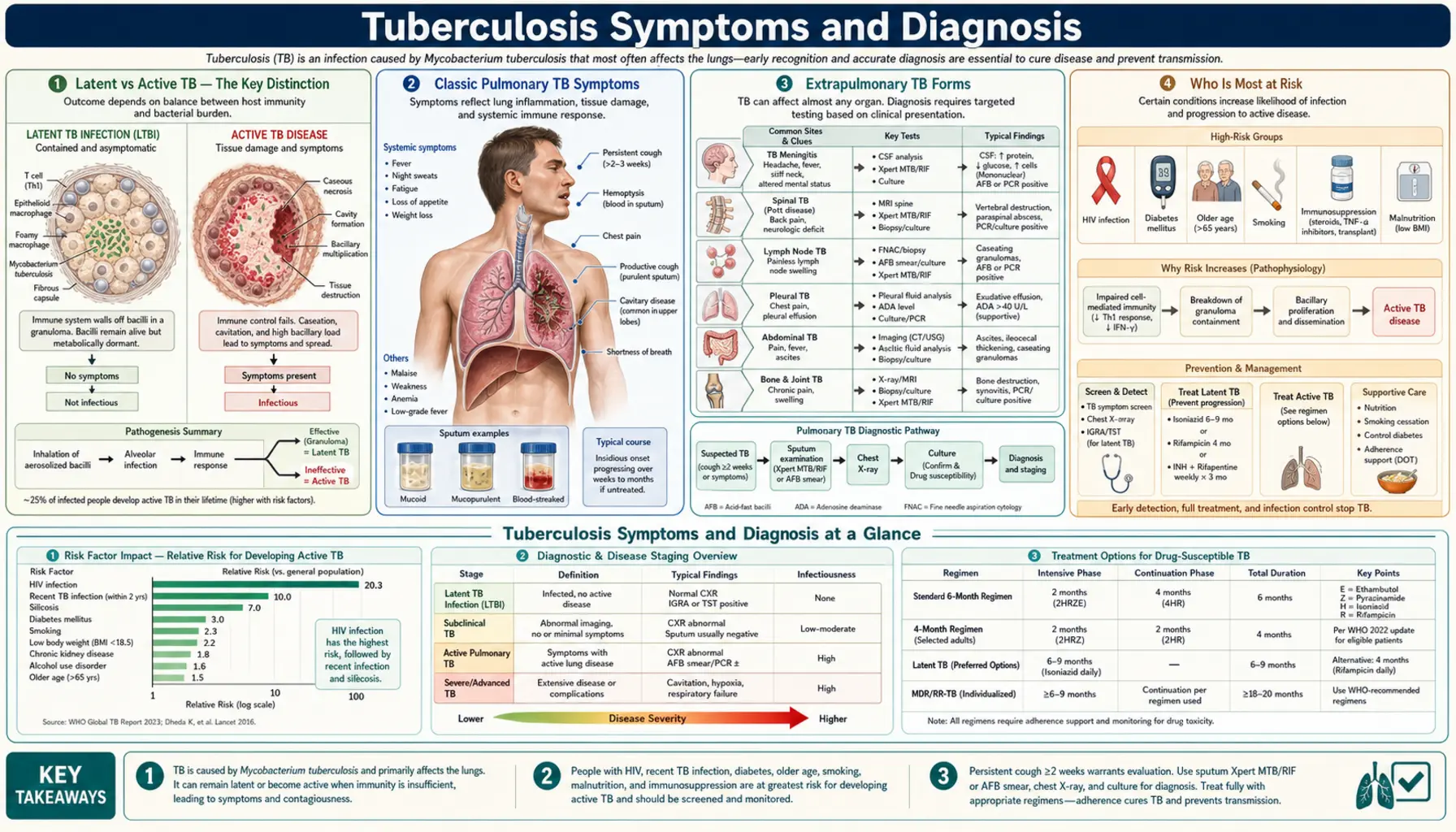
- Latent vs Active TB — The Key Distinction
- Classic Pulmonary TB Symptoms
- Extrapulmonary TB Forms
- Who Is Most at Risk
- When to Suspect TB — Red Flags
- Overview of Diagnostic Tools
- Sputum Collection
- Chest X-Ray Findings in TB
- Research Papers
- Connections
Latent vs Active TB — The Key Distinction
One of the most important things to understand about tuberculosis is that being infected with the bacteria and having the disease are two very different things. About 1.7 billion people worldwide — roughly one in four people on the planet — carry Mycobacterium tuberculosis in their bodies right now without knowing it and without feeling sick at all. This is called latent tuberculosis infection, or LTBI.
Here is what happens physiologically: when your immune system first encounters TB bacteria, it does not destroy them. Instead, it walls them off inside tiny immune structures called granulomas — think of them as microscopic fortresses your body builds around the bacteria to contain them. The bacteria go dormant inside these granulomas, like a fire that has been smothered but not extinguished. As long as your immune system stays strong, those walls hold. The bacteria cannot multiply, cannot spread, and cannot infect anyone else. You have no symptoms because there is no active disease.
The problem comes when those walls weaken. If your immune system becomes compromised — by HIV infection, malnutrition, immunosuppressive drugs, or even just aging — the granulomas can break down. The bacteria escape, begin multiplying, and latent TB reactivates into active disease. The lifetime risk of this happening is roughly 5 to 10 percent in people with healthy immune systems. In people with HIV, that risk jumps to about 10 percent per year — every single year they are co-infected.
This distinction matters enormously for testing and treatment. People with latent TB feel completely well, are not contagious, and will not show up on sputum tests or typical X-rays. Diagnosing them requires different tests — the tuberculin skin test (TST) or interferon-gamma release assays (IGRAs) — that detect immune memory, not active bacteria. People with active TB, by contrast, are often visibly unwell, can spread the disease to others through the air, and require a completely different diagnostic workup.
Classic Pulmonary TB Symptoms
The lungs are where TB most commonly causes active disease — about 80 to 85 percent of active TB cases involve the lungs (pulmonary TB). The symptoms develop gradually over weeks to months, which is part of why they are so often missed or mistaken for other conditions early on.
The single most important warning sign is a persistent cough lasting three weeks or longer. Almost everyone gets a cough from a cold or flu, but those clear up within one to two weeks. A cough that keeps going, especially one that is productive (bringing up sputum), should prompt concern about TB. At first the cough may be dry, but as the disease progresses it typically becomes productive with yellowish or greenish mucus.
Hemoptysis — coughing up blood or blood-stained sputum — is one of the most alarming TB symptoms. It occurs because TB bacteria gradually destroy lung tissue, forming cavities (hollow pockets) inside the lung. These cavities erode into the walls of nearby blood vessels. When a vessel wall gives way, blood leaks into the airway and gets coughed up. Hemoptysis is not always a massive bleed; it can be as subtle as streaks of blood in sputum. Any amount of blood in sputum is a medical red flag, especially with a prolonged cough.
Night sweats are drenching sweats that occur during sleep — not the mild warmth of sleeping under too many blankets, but sweating that soaks through bedclothes and sheets. The mechanism involves the immune system's inflammatory response to the bacteria, which disrupts normal temperature regulation. Many patients describe waking up needing to change their clothes or sheets.
Fever in TB tends to be low-grade (often 37.5–38.5°C / 99–101°F) and characteristically comes on in the late afternoon or evening — a pattern called hectic or quotidian fever. Unlike the high fevers of acute infections like pneumonia, TB fever can be subtle enough that patients barely notice it.
Weight loss is so characteristic of TB that for centuries the disease was called "consumption" — because it appeared to consume the body from within. TB bacteria trigger a sustained inflammatory state that dramatically increases the body's energy demands while simultaneously suppressing appetite. Patients may lose 5 to 10 kilograms (10 to 20 pounds) over the course of weeks or months without trying. Significant unexplained weight loss combined with cough should always raise suspicion for TB.
Other common symptoms include fatigue (persistent exhaustion that doesn't improve with rest), chest pain (particularly with breathing, from inflammation of the pleura surrounding the lung), and shortness of breath (from destroyed or compressed lung tissue). Appetite loss is nearly universal in active TB.
Extrapulmonary TB Forms
TB bacteria can travel through the bloodstream and lymphatic system to infect virtually any organ in the body. When this happens outside the lungs, it is called extrapulmonary TB. It accounts for about 15 to 20 percent of TB cases in people with healthy immune systems, but is far more common — sometimes exceeding pulmonary TB — in people with HIV or other immune deficiencies. Extrapulmonary TB is often harder to diagnose because the symptoms are less typical and specimens are harder to obtain.
Lymph node TB (tuberculous lymphadenitis) is the most common form of extrapulmonary TB. It typically appears as painless, slowly enlarging swelling of lymph nodes in the neck (cervical lymphadenopathy), though it can affect lymph nodes elsewhere. Over time the nodes may become matted together, and in some cases they rupture and drain through the skin, forming a chronic draining sinus. This form is particularly common in children and in people from high-burden countries.
Pleural TB occurs when TB bacteria infect the pleural space — the thin cavity between the lung and the chest wall. This causes a pleural effusion (fluid accumulation) and pleurisy (sharp chest pain that worsens with breathing). Patients typically present with chest pain, shortness of breath, and fever. Diagnosis requires sampling the pleural fluid and performing a pleural biopsy.
Meningeal TB (tuberculous meningitis) is one of the most dangerous forms of extrapulmonary TB. The bacteria infect the membranes surrounding the brain (meninges), causing headache, stiff neck, photophobia (light sensitivity), confusion, and seizures. It develops subacutely over days to weeks rather than the rapid hours of bacterial meningitis. Without prompt treatment, it carries a high risk of permanent neurological damage or death. Any case of meningitis that does not respond to standard antibiotics should be urgently evaluated for TB.
Spinal TB (Pott's disease) infects the vertebrae, typically in the thoracic (mid-back) or lumbar (lower-back) spine. It causes progressive back pain, vertebral collapse, and potentially catastrophic spinal cord compression if untreated. The classic clinical picture is a patient from a high-burden country presenting with chronic back pain and a deforming "gibbus" hump where a collapsed vertebra has pushed the spine forward.
Renal TB infects the kidneys and urinary tract, causing symptoms resembling a urinary tract infection — flank pain, frequent urination, blood in the urine — but not responding to standard antibiotics. It can progress to scarring and destruction of kidney tissue.
Pericardial TB infects the sac surrounding the heart, causing chest pain, shortness of breath, and in severe cases cardiac tamponade — a life-threatening compression of the heart by accumulated fluid.
Miliary TB is the most widespread and dangerous form, occurring when large numbers of bacteria escape into the bloodstream simultaneously and seed multiple organs. The name comes from the appearance on chest X-ray: thousands of tiny nodules scattered through both lungs, resembling millet seeds. Patients are typically very unwell with high fevers, weight loss, and multi-organ involvement. Miliary TB can be rapidly fatal without treatment.
Who Is Most at Risk
Not everyone exposed to M. tuberculosis gets infected, and not everyone infected progresses to active disease. Several biological, social, and environmental factors dramatically shift those odds.
HIV co-infection is the single most powerful risk factor for progressing from latent TB to active disease. Where a healthy person has a 5 to 10 percent lifetime risk of reactivation, someone with HIV faces approximately a 10 percent risk every year. This is because HIV progressively destroys CD4 T-cells — precisely the immune cells that maintain the granulomas containing latent TB. As CD4 counts fall, those containment structures break down. Globally, people with HIV account for roughly 8 percent of TB cases despite being a much smaller fraction of the population.
Recent exposure carries high risk. Household contacts of an active TB patient have roughly a 25 to 50 percent chance of becoming infected if they share living space over weeks. Healthcare workers who encounter TB patients regularly, especially those without proper ventilation or respiratory protection, face elevated exposure.
Immunosuppressive medications — particularly TNF-alpha inhibitors (such as adalimumab, infliximab, etanercept, used for rheumatoid arthritis, psoriasis, and Crohn's disease) — significantly increase the risk of TB reactivation. TNF-alpha is a critical cytokine for maintaining granuloma integrity. Blocking it can cause latent TB to reactivate even years after infection. This is why TB screening (TST or IGRA) is mandatory before starting these medications, and why treatment for latent TB is required if screening is positive.
Diabetes mellitus approximately triples the risk of active TB and is thought to account for up to 15 percent of TB cases globally. High blood sugar impairs the function of the macrophages — the immune cells that form the core of granulomas.
Malnutrition is one of the oldest known risk factors, explaining why TB historically devastated poverty-stricken populations. Deficiencies of vitamins D and A, zinc, and protein all impair the immune response to TB bacteria.
Additional risk factors include chronic kidney disease (uremia suppresses immune function), silicosis (silica dust damages macrophages in the lung, dramatically increasing TB risk among miners and stone cutters), smoking, incarceration (overcrowded facilities with poor ventilation), homelessness, and birth or residence in a high-burden country (sub-Saharan Africa, South and Southeast Asia, Eastern Europe).
When to Suspect TB — Red Flags
TB is often called "the great masquerader" because its symptoms overlap with many common conditions. Part of the reason TB causes so much preventable illness and death is that patients and providers assume the chronic cough is from smoking, the weight loss is from stress, the fatigue is from overwork. Knowing when to override those assumptions is critical.
The most important clinical rule is: cough lasting more than three weeks, combined with any of the following — fever, night sweats, or unexplained weight loss — should be treated as TB until proven otherwise. This combination of symptoms is sometimes called the "classic TB tetrad," and in any patient from or who has traveled to a high-burden country, it must trigger a full diagnostic workup.
Hemoptysis in any endemic context — any amount of blood in sputum, in a patient with prolonged cough or TB risk factors — should prompt immediate TB evaluation rather than reassurance.
Unexplained lymphadenopathy — particularly painless, slowly growing lymph node swelling in the neck in a patient from a high-burden country — should raise TB lymphadenitis as a leading diagnosis. Many such cases are initially attributed to reactive lymph nodes from minor infections and only investigated after months of swelling.
Chronic back pain in immigrants from high-burden countries deserves spinal imaging and consideration of Pott's disease, particularly if there is a history of TB exposure or if pain is slowly progressive over months.
Meningitis not responding to standard antibiotics must immediately raise concern for tuberculous meningitis. Standard bacterial meningitis treatments (antibiotics for Streptococcus pneumoniae, Neisseria meningitidis, etc.) have no effect on TB. Time lost before adding anti-TB therapy directly worsens neurological outcomes.
In patients who are immunocompromised — particularly those with HIV, on biologics, or on corticosteroids — the threshold for suspecting TB should be even lower, and the presentation may be atypical (minimal cough, no fever, lower-lobe disease on X-ray rather than the classic upper-lobe pattern).
Overview of Diagnostic Tools
TB diagnosis uses a two-track system depending on whether you are looking for latent infection or active disease. The same test cannot do both, because they detect completely different things — and understanding why helps make sense of the testing process.
For latent TB, the goal is to detect immune memory — evidence that your immune system has encountered TB bacteria in the past, even though there is no active infection happening now. Two tests do this:
- The Tuberculin Skin Test (TST), also called the Mantoux test or PPD, injects a small amount of tuberculin protein under the skin. A raised, hardened bump (induration) at the injection site 48 to 72 hours later indicates an immune memory response to TB proteins.
- Interferon-Gamma Release Assays (IGRAs) — blood tests (QuantiFERON-TB Gold and T-SPOT.TB) — measure the amount of interferon-gamma that white blood cells release when exposed to TB-specific proteins in a test tube. Unlike the TST, IGRAs are not affected by prior BCG vaccination, making them more specific in countries with BCG programs.
For active TB, the goal shifts entirely. You need to find actual bacteria — not just immune memory. The tests used are:
- Sputum smear microscopy — staining a sputum sample to look for acid-fast bacilli (AFB) under a microscope. Fast and cheap but misses roughly 40 to 60 percent of cases, especially those with lower bacterial loads.
- Sputum culture — growing the bacteria in a laboratory. The gold standard for detecting TB and for drug susceptibility testing, but takes 2 to 6 weeks for results.
- GeneXpert MTB/RIF (Xpert) — a rapid molecular test that detects TB DNA and simultaneously checks for rifampicin resistance in under 2 hours. The WHO now recommends Xpert as the first diagnostic test for people suspected of having TB, replacing smear as the initial test of choice.
- Chest X-ray — provides structural evidence of disease but cannot definitively confirm or exclude TB on its own.
It is important to understand that a positive TST or IGRA in a patient with symptoms of active TB does not mean the latent test is sufficient — you still need to look for active bacteria using sputum tests. Conversely, active TB can occasionally produce a negative TST or IGRA in severely immunocompromised patients (a "false-negative" from immune exhaustion).
Sputum Collection
Sputum testing is the cornerstone of active TB diagnosis, but the quality of the specimen makes an enormous difference in whether bacteria are found. Poor collection technique is one of the most common reasons TB is initially missed.
The key rule is early morning specimens are best. During sleep, secretions accumulate in the airways and airways narrow slightly. The bacterial concentration in first-morning sputum is measurably higher than in specimens collected later in the day. This is the specimen most likely to yield a positive result on smear or culture.
Proper collection means producing sputum from deep in the lungs — not just saliva from the mouth or nasal drip from the back of the throat. A proper specimen comes from a deep, productive cough that brings up mucus from the lower airways. Patients should be instructed to take three deep breaths, then cough forcefully on the third breath into a wide-mouthed container. Many people need demonstration or coaching to do this correctly the first time.
The WHO and most guidelines recommend three sputum specimens collected over three consecutive days (three samples on three separate mornings). The reason is straightforward: no single specimen detects 100 percent of cases. Adding a second sample increases detection from roughly 60 percent to 85 percent. Adding a third brings it to approximately 87 to 90 percent. Additional samples beyond three provide diminishing returns.
For patients who cannot produce sputum spontaneously — those with dry, non-productive coughs — induced sputum is an option. The patient inhales hypertonic saline (3 to 5 percent salt water) through a nebulizer for 15 to 20 minutes. The irritation triggers deep coughing and sputum production in most patients. Induced sputum should be collected in a negative-pressure room or well-ventilated space because the procedure generates aerosols that can transmit TB.
In children under five, sputum production is nearly impossible — they naturally swallow sputum rather than coughing it up. The alternative is gastric aspirate, where a thin tube is passed through the nose and down to the stomach early in the morning before the child has eaten. Overnight, swallowed sputum accumulates in the stomach and can be suctioned out and tested. While unpleasant, this is the most reliable method for bacteriological confirmation in young children who cannot produce sputum on demand.
Chest X-Ray Findings in TB
Chest X-ray is an essential but imperfect tool in TB diagnosis. It can show structural changes that strongly suggest TB, guide clinical decision-making, and detect complications — but it cannot confirm TB on its own, and some patients with active TB have nearly normal X-rays (especially those who are immunocompromised).
Primary TB pattern occurs when someone is infected for the first time, typically in childhood. The immune system has never encountered TB before, so it mounts a localized response wherever the bacteria initially land. On X-ray this appears as an infiltrate (a hazy density indicating inflammation) in the lower or middle lobes of the lung, often accompanied by enlarged hilar lymph nodes (the nodes at the center of the chest where the main bronchi enter the lungs). This combination of a peripheral lung opacity plus central lymph node enlargement is called a Ghon complex (or Ranke complex if calcified). This pattern is typical in children and in immunocompromised adults who have not previously mounted an immune response.
Reactivation TB pattern (also called post-primary TB) is the classic adult presentation. When latent TB reactivates, the bacteria preferentially seed the upper lobes of the lungs — specifically the apical (top) and posterior segments. This is thought to be because the upper lobes have higher oxygen tension, and TB bacteria are obligate aerobes that thrive in high-oxygen environments. On X-ray you see infiltrates, consolidation, and the hallmark finding: cavities — hollow spaces with thick, irregular walls that form as the center of an infected area liquefies and is coughed out. Cavitation strongly correlates with high bacterial burden and high infectiousness.
Miliary pattern appears when TB bacteria spread through the bloodstream and seed both lungs diffusely. The X-ray shows thousands of tiny, uniformly sized nodules (1 to 3 mm each) scattered evenly throughout both lung fields. The appearance resembles scattered millet seeds — which is precisely how the name arose. Miliary TB is a radiological emergency; the pattern combined with systemic illness demands immediate treatment.
Pleural effusion appears as a white opacity layering along the bottom of the lung or the side of the chest cavity. In young adults from high-burden countries, a pleural effusion without an obvious cause (trauma, heart failure, cancer) should prompt strong consideration of pleural TB.
It is essential to understand the limits of X-ray. A normal chest X-ray does not rule out TB — early active TB, extrapulmonary TB, and TB in severely immunocompromised patients can all present with minimal or absent X-ray findings. Conversely, old healed TB, other infections (histoplasmosis, aspergillosis), and lung cancer can produce X-ray findings that mimic active TB. The chest X-ray guides the clinical picture but must always be interpreted alongside the patient's symptoms, risk factors, and microbiological results.
Research Papers
- Search PubMed — A landmark New England Journal of Medicine review of tuberculosis covering pathogenesis, epidemiology, diagnosis, and treatment, providing a comprehensive clinical framework for understanding the full spectrum of TB disease.
- Menzies et al., 2014 (PMID 25230299) — A major CMAJ review of latent tuberculosis infection covering prevalence, testing strategies with TST and IGRAs, risk stratification, and the evidence base for preventive therapy in different populations.
- Search PubMed — A Lancet paper examining the intersection of HIV and TB, quantifying the dramatically elevated risk of TB disease in HIV-positive individuals and analyzing strategies for integrated TB-HIV diagnosis and care.
- Search PubMed — A pivotal Lancet trial demonstrating that a 4-month treatment regimen containing rifapentine and moxifloxacin is non-inferior to the standard 6-month regimen for drug-sensitive TB, opening the door to shorter treatment courses.
- Search PubMed — The joint ATS/CDC/ERS/IDSA clinical practice guidelines for treatment of drug-susceptible tuberculosis, providing evidence-graded recommendations on regimen selection, monitoring, and special populations.
- Search PubMed — A comprehensive European Respiratory Journal review summarizing what is known about TB transmission, pathogenesis, immunology, and the global burden of disease, with emphasis on gaps that impede control efforts.
- Search PubMed — A Nature Reviews Disease Primers overview of tuberculosis providing a detailed reference on global epidemiology, microbiology, host-pathogen interaction, diagnosis, treatment, and prevention for clinicians and researchers.
- Search PubMed — A Lancet seminar on tuberculosis describing clinical features, radiological patterns, microbiological diagnosis, and treatment of both pulmonary and extrapulmonary TB with special attention to resource-limited settings.
- Kwan & Ernst, 2011 (PMID 21338485) — A Clinical Microbiology Reviews article examining the complex immunological and clinical interactions between HIV and TB, explaining why HIV so dramatically accelerates TB disease progression and complicates diagnosis.
- Search PubMed — A Science paper modeling the global TB burden and the conditions under which TB could be eliminated, providing quantitative analysis of how social determinants, HIV, and treatment coverage shape epidemic trajectories.
Connections
- Mycobacterium tuberculosis Overview
- TB Treatment and Prevention
- Pulmonology Conditions
- HIV and AIDS
- Infectious Disease
- All Bacteria
- Lab Tests