Tuberculosis Treatment and Prevention
HRZE First-Line Regimen
The four-drug standard of care: isoniazid, rifampicin, pyrazinamide, and ethambutol — dosing, monitoring, and managing side effects.
Prevention & BCG Vaccine
BCG vaccination, latent TB treatment, isoniazid preventive therapy, and contact tracing strategies.
MDR-TB & Drug Resistance
Multidrug-resistant and extensively drug-resistant TB: causes, second-line drugs, new regimens, and global crisis.
Table of Contents
- Treatment Principles: Bactericidal vs Sterilizing Drugs
- DOTS: Directly Observed Therapy Short-Course
- The Intensive Phase: First 2 Months (2HRZE)
- The Continuation Phase: 4 Months on HR
- Monitoring During Treatment
- Drug-Induced Hepatotoxicity
- Pyridoxine (Vitamin B6) Supplementation
- Treatment Success Rates and Preventing Relapse
- Research Papers
- Connections
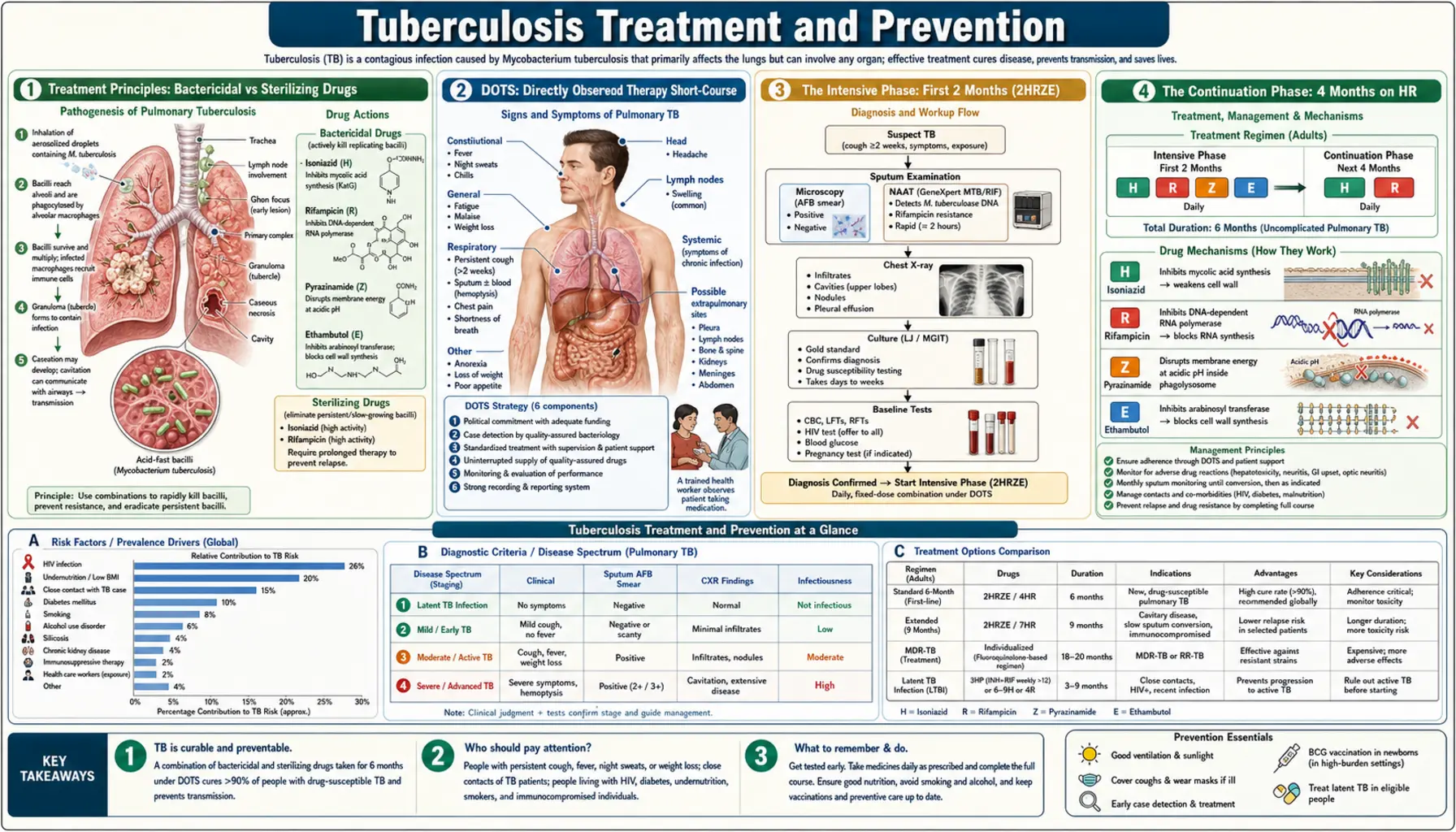
Treatment Principles: Bactericidal vs Sterilizing Drugs
TB treatment works on a fundamentally different logic than most antibiotic courses. You can't just take a single drug for a week and be done. Understanding why helps you stick with a long, multi-drug regimen that can feel overwhelming at first.
Why multiple drugs? In any large population of TB bacteria in your lungs, a small number will have random genetic mutations that make them resistant to any single drug. If you take only one antibiotic, the sensitive bacteria die — but the resistant ones survive and multiply until they dominate. This is exactly how drug-resistant TB is created. Using three or four drugs simultaneously means that the probability of a bacterium having mutations that resist ALL of them simultaneously is vanishingly small. Multi-drug therapy is resistance insurance.
Why so long? M. tuberculosis divides only once every 12 to 24 hours — compared to 20 minutes for a common gut bacterium like E. coli. Most antibiotics work by attacking bacteria while they're actively growing and replicating. A slow-growing organism needs much more time of sustained drug exposure to be killed. Beyond that, TB bacteria can essentially go dormant inside your immune cells, pausing their metabolism and becoming temporarily invisible to drugs that target growing bacteria. These dormant survivors are the seeds of relapse months or years later.
Three bacterial populations that treatment must kill:
- Actively replicating bacteria — thriving in the oxygen-rich cavities of the lungs. Isoniazid and rifampicin are bactericidal (directly killing) against these. This is the population responsible for spreading TB to other people.
- Intermittently replicating bacteria — cycling in and out of slow replication, often in the walls of lung cavities. Rifampicin is particularly effective here because it kills bacteria during brief spurts of activity even when they're mostly dormant.
- Dormant/intracellular bacteria — hiding inside macrophages (the immune cells that engulf TB bacteria but can't always kill them). The interior of an infected macrophage is acidic. Pyrazinamide is uniquely active in this acidic environment and is the only first-line drug that reaches and kills this dormant population. Without pyrazinamide, treatment would need to be 9-12 months instead of 6.
"Sterilizing" activity is the term used for drugs that can eliminate that last dormant population. Pyrazinamide and rifampicin have sterilizing activity. This is what allows treatment to end at 6 months rather than years — without sterilization, dormant bacteria would reactivate and cause relapse. When treatment is complete and the sterilizing phase is done, there are theoretically zero living TB bacteria left in your body. That's a cure, not just remission.
With proper adherence to the full 6-month course, drug-sensitive TB has a treatment success rate exceeding 95%. That's an extraordinary outcome for a disease that was a death sentence for much of human history.
DOTS: Directly Observed Therapy Short-Course
In the early days of TB treatment, when patients were given drugs to take at home, treatment failure rates were alarmingly high — not because the drugs didn't work, but because people stopped taking them. This is understandable: the drugs have side effects, people feel better after a few weeks and assume they're cured, the regimen is long and complicated, and poverty, work obligations, and stigma all get in the way. The consequence of poor adherence isn't just treatment failure for that person — it's the creation of drug-resistant strains that can spread to others.
DOTS (Directly Observed Therapy Short-Course) was developed as the solution. A healthcare worker, community volunteer, or trained family member physically watches the patient swallow every single dose. Not just checking in — actually watching, every time. The "Short-Course" refers to the 6-month regimen, which was an improvement over the 12-18 month regimens used before effective sterilizing drugs were available.
The WHO's DOTS strategy has five components:
- Political commitment — governments must fund TB programs and prioritize them as a public health emergency, not an afterthought.
- Smear microscopy — laboratory diagnosis (sputum examination) to identify infectious cases and monitor treatment response.
- Uninterrupted drug supply — the supply chain must never break. Running out of one drug mid-treatment is how resistance emerges.
- Directly observed treatment — the literal watching-them-swallow-it protocol.
- Monitoring and recording — systematic tracking of every patient's treatment outcome to measure program effectiveness and catch problems early.
DOTS-Plus extended this framework to MDR-TB, which requires longer and more toxic second-line drug regimens. The End TB Strategy (launched by WHO in 2015) builds on DOTS with additional goals around universal health coverage, social protection, and research — aiming to reduce TB deaths 90% and new cases 80% by 2030.
Does DOT actually beat self-administered therapy (SAT)? Randomized trials and systematic reviews have found that when patients receive strong education, support, pill organizers, and follow-up, their treatment outcomes are similar to those under DOT. The evidence suggests it's the package of support — not the surveillance itself — that matters. Highly motivated, well-supported patients on SAT do just as well as those on DOT.
Video DOT (VDOT) has emerged as an innovative middle ground: the patient takes their medication in front of a phone camera, and the video is reviewed in real time or asynchronously by a health worker. Studies have shown VDOT can achieve adherence rates equivalent to in-person DOT, with much greater convenience and reduced cost. It's particularly valuable for patients who live far from clinics or have work schedules that make daily clinic visits impossible.
Adherence supports that work: pill organizers with built-in alarms, SMS or phone reminders, peer supporters (other TB survivors who check in), nutritional support (malnutrition is both a risk factor for TB and a consequence of active disease — providing food packages significantly improves adherence in food-insecure populations), and treating addiction or mental health conditions that interfere with medication-taking.
The Intensive Phase: First 2 Months (2HRZE)
The first two months of TB treatment use all four first-line drugs simultaneously. This is the most powerful phase — the one that rapidly reduces the bacterial load in your lungs and stops you from being infectious to others.
The four drugs and what they do:
- Isoniazid (H) — the backbone of TB treatment. Kills actively replicating bacteria rapidly by blocking mycolic acid synthesis (mycolic acid is a critical component of TB's unique cell wall — the same thick, waxy wall that makes it so hard to kill). Bactericidal. Also has some sterilizing activity. Taken once daily on an empty stomach for best absorption.
- Rifampicin (R) — the other backbone drug. Kills bacteria by blocking RNA polymerase (an enzyme TB bacteria need to read their genetic code and make proteins). Works against actively AND intermittently replicating bacteria. Has excellent sterilizing activity. Turns urine, sweat, and tears orange-red — this is harmless but surprising if patients aren't warned (it can permanently stain soft contact lenses).
- Pyrazinamide (Z) — the sterilizing drug that cuts treatment from 9+ months to 6. Works uniquely in the acidic environment inside macrophages where dormant bacteria hide. Only used in the intensive phase (first 2 months) because its sterilizing effect is achieved by then. Main risk: hepatotoxicity (liver inflammation) and elevated uric acid (can trigger gout).
- Ethambutol (E) — added to the intensive phase primarily as resistance protection. Inhibits arabinosyl transferase enzymes involved in the TB cell wall. Its main risk: optic neuritis (inflammation of the optic nerve causing blurred vision and loss of red-green color discrimination — usually reversible if caught early, potentially permanent if not). Used until drug susceptibility results confirm sensitivity to isoniazid and rifampicin, then typically stopped.
What happens during these 2 months? Most patients start feeling significantly better within the first 2-4 weeks. Fever typically breaks, night sweats diminish, cough starts improving. This is when the danger of stopping early is greatest — feeling well creates a false sense of being cured. The TB bacteria have been severely reduced in number, but the survivors — the dormant, intracellular ones — are still there.
The sputum conversion test: At the end of the intensive phase, sputum is rechecked for TB bacteria. Smear conversion (bacteria no longer visible under microscopy) occurs in over 80% of patients by 2 months. Culture conversion (no growth in culture — a more sensitive test) takes longer, typically 8-12 weeks after starting treatment. If sputum culture is still positive at 8 weeks, this is a red flag. It could mean the bacteria are drug-resistant, the patient isn't absorbing the drugs properly, or adherence has been poor. Drug susceptibility testing (DST) should be sent urgently if not already done.
Becoming non-infectious: One of the most important things to know is that most patients with pulmonary TB become non-infectious within 2 weeks of starting effective treatment. The bacterial load in their sputum drops dramatically. Children can typically return to school after 2 weeks; adults can often return to non-crowded work settings. This knowledge reduces stigma and isolation — though patients must complete the full course regardless of how quickly they improve.
The Continuation Phase: 4 Months on HR
After successfully completing the 2-month intensive phase — confirmed by sputum smear conversion and clinical improvement — treatment continues for 4 more months using just two drugs: isoniazid and rifampicin. This is the continuation phase, and it's where the war against dormant bacteria is won or lost.
Why still 4 more months? By the end of the intensive phase, the bacterial burden in your lungs has been dramatically reduced. But "dramatically reduced" is not zero. Dormant TB bacteria are still hiding in the scar tissue, old cavities, and macrophages throughout your respiratory system. They're metabolically inactive — not replicating, not making proteins — so they're relatively protected from antibiotics. Isoniazid and rifampicin together slowly eliminate these survivors over 4 months. If you stop too early, these dormant bacteria reactivate weeks, months, or even years later. This is a relapse — active TB returning after apparent cure.
The full standard regimen notation: 2HRZE/4HR. The numbers indicate the number of months, and the letters indicate the drugs used in each phase. This shorthand is used globally and you may see it in your TB documentation.
A shorter 4-month regimen: Research has investigated whether treatment can be shortened without increasing relapse rates. The TBTC Study 31/ACTG A5349 (published in 2021) tested a 4-month regimen that substituted rifapentine (a longer-acting rifamycin, taken weekly in some LTBI regimens but daily in this study) for rifampicin and added moxifloxacin (a fluoroquinolone antibiotic with TB activity). Results: the 4-month regimen was non-inferior to the standard 6-month regimen for drug-sensitive pulmonary TB in adults. This represents the first major reduction in TB treatment duration in decades. The FDA and some guidelines now support it for select patients — typically adults with drug-sensitive pulmonary TB who don't have very severe disease.
End-of-treatment evaluation: At month 6 (or end of the alternative 4-month regimen), patients are evaluated with repeat sputum examination and often chest X-ray. The goal is to confirm treatment success — bacteriologic cure. Most patients are discharged from active treatment at this point, with instructions to return immediately if symptoms recur.
Global treatment completion rates: The WHO 2023 Global TB Report documented an 88% treatment success rate for new drug-sensitive TB cases globally — an encouraging figure representing decades of improvements in drug supply, DOTS implementation, and patient support programs. However, treatment completion rates are significantly lower for MDR-TB (around 60%) and XDR-TB (around 40%), reflecting the much harder path those patients face.
What "treatment success" means: The WHO defines treatment success as patients who are cured (bacteriologically confirmed negative sputum) plus those who completed treatment (finished the full course without bacteriologic confirmation either way). Both are counted as success; the distinction matters for research but not for the individual patient who finished their course.
Monitoring During Treatment
TB treatment involves potent drugs taken for 6 months or longer. Regular monitoring catches side effects before they become serious — and protects your liver, eyes, kidneys, and nervous system throughout the process.
Baseline tests before starting treatment:
- Liver function tests (LFTs): ALT, AST, and bilirubin. Establishes baseline before hepatotoxic drugs are started. If liver enzymes are already elevated (alcohol use, hepatitis B/C, liver disease), closer monitoring is essential.
- Full blood count (FBC): Checks for pre-existing anemia (common in TB patients due to chronic infection and malnutrition).
- Renal function: Creatinine and eGFR. Ethambutol is primarily cleared by the kidneys — impaired renal function increases the risk of optic neuritis by allowing drug to accumulate.
- Visual acuity and color vision: Baseline eye test before starting ethambutol. Use a Snellen chart (reading chart) and Ishihara plates (red-green color discrimination test). This becomes the comparison point for detecting early optic neuritis.
- Uric acid: Pyrazinamide inhibits uric acid excretion by the kidneys. Patients with pre-existing gout or high uric acid levels are at risk of acute gout flares during the intensive phase.
- Weight: Drug doses are weight-based. Patients with active TB are often malnourished — as they regain weight during treatment, doses may need to be increased.
- HIV test: If status unknown. HIV profoundly alters TB management — drug interactions, immune reconstitution inflammatory syndrome (IRIS), timing of ART initiation.
During treatment — standard monitoring schedule:
- Monthly visits: Weight check (dose adjustment if significant change), symptom review (nausea, jaundice, visual changes, tingling/numbness), adherence assessment, pill supply.
- Monthly LFTs: For all patients at elevated risk — age over 35, alcohol use, pre-existing liver disease, HIV, pregnancy, malnutrition. Low-risk patients may need LFTs only if symptoms develop.
- Monthly eye tests while on ethambutol: Visual acuity and red-green color discrimination at every visit. The first sign of optic neuritis is usually blurred vision or difficulty distinguishing red from green. Ethambutol must be stopped immediately if these develop — delay risks permanent visual loss.
- Sputum at 2 months: Critical milestone — confirming smear conversion and triggering urgency if not converted (signals possible drug resistance).
- Sputum at end of treatment: Confirms bacteriologic cure.
- Uric acid monitoring: For patients with gout symptoms during pyrazinamide phase — allopurinol may be needed.
HIV-positive patients: Additional complexity. CD4 count monitoring guides immune function assessment. Antiretroviral drug interactions with rifampicin are significant — rifampicin powerfully induces liver enzymes (CYP3A4) and reduces blood levels of many ARVs, particularly protease inhibitors and some NNRTIs. Most current guidelines recommend efavirenz-based ART regimens during rifampicin-containing TB treatment, as efavirenz levels are only modestly reduced. The timing of ART initiation after starting TB treatment depends on CD4 count — earlier is generally better for very immunocompromised patients, but increases the risk of immune reconstitution inflammatory syndrome (IRIS), a paradoxical worsening of TB symptoms as the immune system recovers.
Drug-Induced Hepatotoxicity — The Most Feared Side Effect
Of all the side effects of TB treatment, drug-induced liver injury (DILI) is the one clinicians worry about most — because it can be severe, because the drugs causing it are essential to treatment, and because figuring out which drug is the culprit requires careful detective work.
Which drugs are hepatotoxic? Isoniazid, rifampicin, and pyrazinamide — three of the four first-line drugs — all carry hepatotoxicity risk. Ethambutol is rarely hepatotoxic. When used together (as they are in the intensive phase), the risk is higher than any one drug alone. Pyrazinamide is generally considered the most hepatotoxic of the three and the most likely culprit when severe DILI occurs.
Risk factors that increase hepatotoxicity risk:
- Age over 35 (slower metabolism of isoniazid)
- Alcohol use (even moderate amounts significantly increase risk)
- Malnutrition (reduced glutathione — the liver's main antioxidant defense)
- Pre-existing liver disease (hepatitis B or C, fatty liver, cirrhosis)
- HIV infection (both the virus itself and antiretroviral drugs can affect liver function)
- Pregnancy and the postpartum period
- Slow acetylator status (a genetic variant in the enzyme that metabolizes isoniazid — more common in certain populations; slow acetylators accumulate more isoniazid)
Symptoms of drug-induced liver injury: Nausea, vomiting, right upper quadrant abdominal pain or discomfort, loss of appetite, fatigue, jaundice (yellowing of eyes and skin), dark urine, pale stools. The symptoms are often nonspecific and can be confused with TB itself (which also causes nausea and fatigue) or other causes of liver disease. Jaundice is a late sign — don't wait for it before checking liver tests.
When to stop TB drugs:
- Symptomatic DILI: Stop ALL TB drugs if ALT is more than 3 times the upper limit of normal WITH symptoms of hepatitis (nausea, jaundice, right upper quadrant pain).
- Asymptomatic liver enzyme elevation: Stop if ALT exceeds 5 times the upper limit of normal, even without symptoms.
- Any clinical jaundice: Stop all drugs regardless of exact ALT level — jaundice indicates significant liver dysfunction.
What happens after stopping? Liver enzymes typically start falling within 1-2 weeks of stopping the offending drugs. Once ALT has returned to less than 2 times the upper limit of normal (and symptoms resolve), drugs can be carefully reintroduced one at a time — called sequential rechallenge. The recommended sequence is:
- Start rifampicin alone for 3-7 days — monitor LFTs. If tolerated without enzyme rise, proceed.
- Add isoniazid — monitor. Isoniazid is the most common culprit in mild-to-moderate DILI.
- Add pyrazinamide last — monitor. In severe DILI, pyrazinamide may be omitted permanently, requiring an extended 9-month regimen to compensate for the loss of its sterilizing activity.
For patients with severe pre-existing liver disease (advanced cirrhosis, active viral hepatitis), standard TB regimens may be too risky. Hepatologist involvement is essential. Alternative regimens that avoid the most hepatotoxic drugs — sometimes using ethambutol plus a fluoroquinolone plus streptomycin (an injectable) for extended periods — may be necessary. These regimens are less effective and harder to tolerate, which is why managing underlying liver disease before TB treatment, where possible, is important.
Pyridoxine (Vitamin B6) Supplementation
Isoniazid has a chemical quirk that causes it to deplete vitamin B6 (pyridoxine) in the body. B6 is essential for normal nerve function — without enough of it, peripheral nerves can become inflamed and damaged, causing a condition called peripheral neuropathy. The good news: this side effect is almost entirely preventable with cheap, safe B6 supplementation.
How isoniazid depletes B6: Isoniazid forms a chemical complex with pyridoxal phosphate (the active form of B6) that the body can't use. It essentially ties up the vitamin and accelerates its excretion. In people with adequate B6 stores and good nutrition, this effect is usually subclinical — they have enough reserve. In people who are already B6-depleted (from malnutrition, alcohol, pregnancy, or kidney disease), isoniazid pushes them into frank B6 deficiency.
What peripheral neuropathy feels like: Tingling, burning, or numbness starting in the toes and fingers (a "stocking-glove" distribution), sometimes progressing up the legs and arms. It can also cause weakness. In severe cases it becomes debilitating. Patients often describe it as walking on glass or having their feet feel like they're wrapped in cotton. It typically starts subtly and worsens over weeks to months — which is why routine prevention is better than waiting for symptoms.
Who is at high risk and requires routine B6 supplementation:
- HIV-positive patients (isoniazid neuropathy risk is significantly elevated)
- Malnourished patients (common in active TB — protein-energy malnutrition depletes all B vitamins)
- Diabetes (peripheral neuropathy from diabetes is already present in many patients; isoniazid compounds it)
- Chronic kidney disease (kidneys normally process B6; impaired renal function worsens depletion)
- Alcohol use disorder (alcoholism causes severe B vitamin deficiency across the board)
- Pregnancy and breastfeeding (higher B6 requirements; neonatal risk from maternal isoniazid)
- Seizure disorders (B6 deficiency can lower seizure threshold; isoniazid also affects GABA metabolism in the brain)
Standard dose: 25 to 50 mg of pyridoxine daily, taken alongside the isoniazid dose. This is a low, safe dose — well below the levels that can themselves cause neuropathy (which occur only at very high chronic doses, typically 200 mg/day or more). B6 at these doses has essentially no side effects.
All patients on isoniazid preventive therapy (IPT) for latent TB should receive B6. This recommendation applies broadly — anyone taking isoniazid alone for 6-9 months to prevent progression from latent to active TB is at risk for neuropathy. Pyridoxine is cheap (pennies per dose), safe, and definitively preventive. There's no good reason not to prescribe it alongside IPT.
If neuropathy develops despite supplementation: Increase pyridoxine to 100 mg/day. If symptoms persist or worsen, discuss with your TB specialist whether the dose of isoniazid can be reduced or whether the risk-benefit calculation of continuing isoniazid has changed. In most cases, mild neuropathy improves when isoniazid is stopped or the B6 dose is raised.
Treatment Success Rates and Preventing Relapse
Drug-sensitive TB is one of the most curable serious infectious diseases in medicine, with a greater than 95% success rate when patients complete the full treatment course. Understanding what success looks like — and what puts it at risk — helps patients and families navigate the 6-month journey.
Treatment outcomes (WHO definitions):
- Cured: Pulmonary TB patient with bacteriologically confirmed TB at start who was smear- or culture-negative in the last month of treatment AND on at least one previous occasion. The gold standard.
- Treatment completed: Finished the full treatment course without bacteriologic evidence of failure, but without a smear or culture result confirming negativity (often because testing wasn't done). Still counted as success.
- Treatment failed: Still smear- or culture-positive at 5 months or later. This triggers an urgent workup for drug resistance.
- Lost to follow-up: Treatment interrupted for 2 or more consecutive months. A major challenge globally, often driven by poverty, stigma, healthcare access, or drug side effects.
- Died: Died during treatment for any reason.
- Relapse: New episode of active TB after completing treatment and being declared cured or treatment-completed. Relapse represents reactivation of dormant surviving bacteria, and must be distinguished from reinfection (exposure to a new TB strain from another person). Molecular typing (genotyping) of bacterial strains helps make this distinction in research settings.
Risk factors for relapse after completing treatment:
- Cavitary disease on chest X-ray (large, pre-existing lung cavities harbor large bacterial populations that are harder to fully sterilize)
- Smear-positive sputum still present at the end of the 2-month intensive phase (suggests higher bacterial burden)
- Poor adherence during treatment (incomplete sterilization = surviving dormant bacteria)
- Smoking (cigarette smoke impairs the immune response in the lung and is independently associated with both active TB and relapse)
- Diabetes mellitus (impairs immune function; associated with higher bacterial burden and slower sputum conversion)
- HIV infection (ongoing immunosuppression makes it harder for the immune system to clear the final bacterial remnants)
- Malnutrition (protein-energy malnutrition significantly impairs cell-mediated immunity — the arm of the immune system most critical for TB control)
Post-treatment monitoring: Most guidelines recommend follow-up symptom review at 3, 6, and 12 months after completing treatment — particularly for patients with high-burden cavitary disease. Some centers repeat a chest X-ray at 6 months to assess for cavitary changes or new infiltrates. Patients should be clearly instructed to seek medical attention immediately if TB symptoms recur: persistent cough, fever, night sweats, or unexplained weight loss.
Global context: While drug-sensitive TB has excellent outcomes, the global picture remains challenging. The WHO estimates 10.6 million new TB cases and 1.3 million TB deaths in 2022. Most of these deaths are preventable — they result from delayed diagnosis, inadequate drug supply, poverty, malnutrition, and HIV co-infection. Closing the gap between what TB treatment can achieve (95%+ cure) and what it actually achieves in the most vulnerable populations is the central challenge of global TB control.
Research Papers
- Search PubMed — ATS/CDC/IDSA official treatment guidelines for drug-susceptible TB, covering regimen selection, monitoring, and management of special populations including HIV and pregnancy.
- Search PubMed — Comprehensive NEJM review covering the epidemiology, pathogenesis, diagnosis, and treatment of tuberculosis with emphasis on emerging drug-resistant strains.
- Search PubMed — The landmark TBTC Study 31 demonstrating that a 4-month regimen with rifapentine and moxifloxacin is non-inferior to the standard 6-month regimen for drug-sensitive pulmonary TB.
- Search PubMed — Nature Reviews Disease Primers authoritative overview of tuberculosis: microbiology, epidemiology, pathogenesis, diagnosis, treatment, and prevention on a global scale.
- Search PubMed — NEJM review on latent TB infection management, including risk stratification, IGRA vs TST, and isoniazid preventive therapy protocols and efficacy.
- Search PubMed — ATS consensus statement on hepatotoxicity of anti-tuberculosis therapy, providing evidence-based definitions, monitoring recommendations, and drug rechallenge protocols for DILI.
- Search PubMed — European Respiratory Journal review of TB prevention strategies including BCG vaccine efficacy, isoniazid preventive therapy, and novel vaccine candidates in pipeline development.
- Search PubMed — Lancet seminar on tuberculosis providing a comprehensive clinical framework for diagnosis and treatment in both high- and low-resource settings with attention to HIV co-infection.
- Search PubMed — Lancet review of advances in TB drug development highlighting new compounds including bedaquiline and delamanid and their role in addressing the MDR-TB crisis.
- Search PubMed — NEJM study demonstrating GeneXpert MTB/RIF as a rapid molecular test providing simultaneous TB detection and rifampicin resistance identification within 2 hours, transforming TB diagnosis in high-burden settings.
Connections
- Mycobacterium Tuberculosis — Main Hub
- TB Symptoms & Diagnosis Hub
- HRZE First-Line Regimen
- Prevention & BCG Vaccine
- MDR-TB & Drug Resistance
- HIV and Immunodeficiency
- All Bacteria Diseases