MDR-TB and XDR-TB: Drug Resistance in Tuberculosis
Drug-resistant tuberculosis is one of the most serious infectious disease crises of our time — MDR-TB requires treatment 4–5 times longer and up to 100 times more expensive than drug-sensitive TB, with far worse outcomes. Understanding why resistance develops and how the newest drugs are transforming care is essential for patients, families, and anyone navigating a health system dealing with this disease.
Table of Contents
- Defining MDR-TB, XDR-TB, and Pre-XDR-TB
- Global Burden — Scale and Distribution
- How Resistance Arises — Genetic Mutations
- Second-Line Drugs for MDR-TB
- The BPaL Regimen — A Revolution in MDR-TB Treatment
- Outcomes and Mortality in MDR-TB
- Programmatic Challenges — Cost, Adherence, and Access
- Preventing Drug Resistance — The Essential Strategy
- Research Papers
- Connections
- Featured Videos
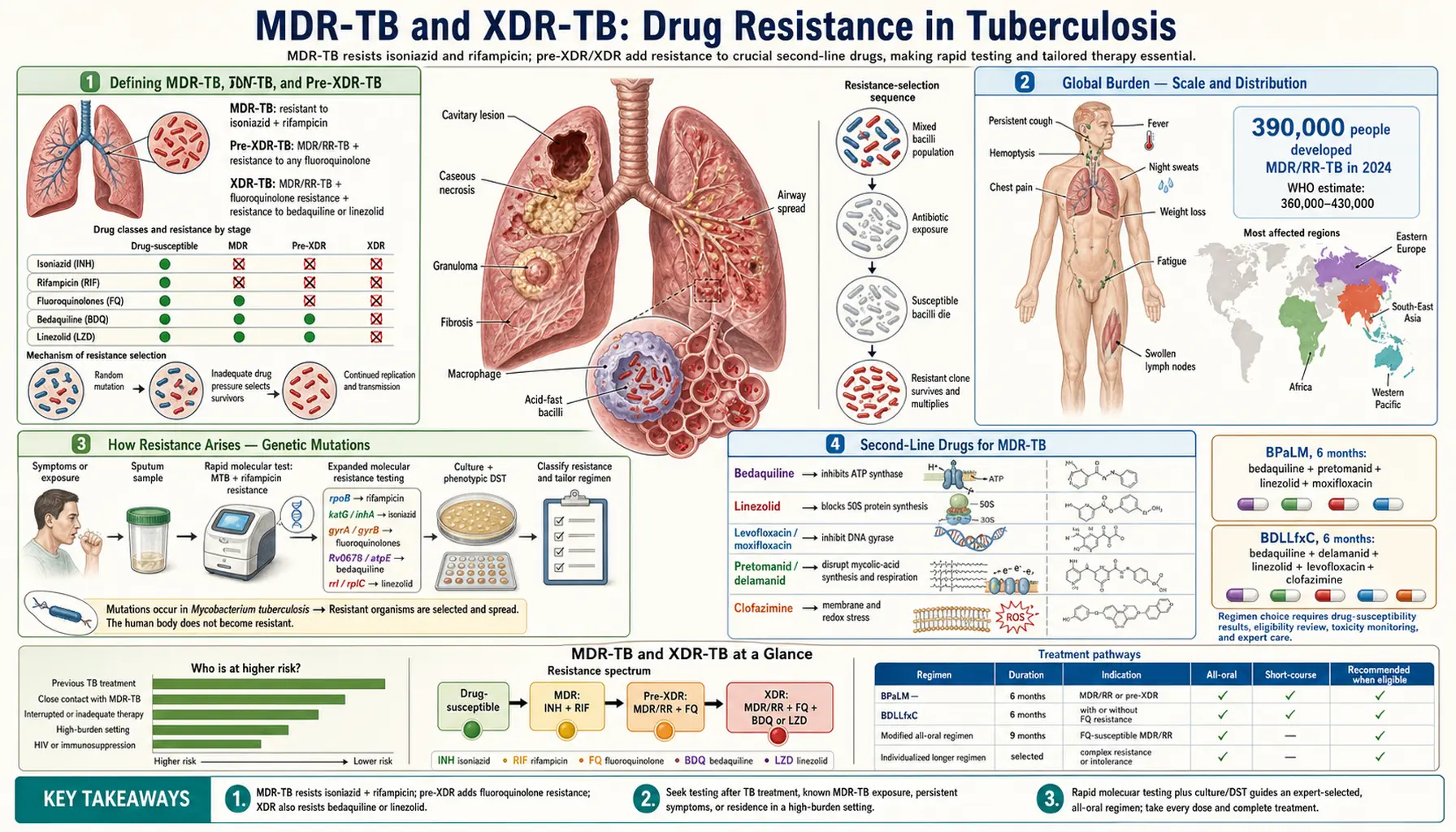
Defining MDR-TB, XDR-TB, and Pre-XDR-TB
The language around drug-resistant TB can be confusing, so understanding the precise definitions helps you follow medical discussions and understand why your treatment plan looks the way it does.
MDR-TB (multidrug-resistant TB) means the bacteria are resistant to both isoniazid AND rifampicin — the two most powerful first-line drugs. Because these two drugs form the backbone of all standard TB treatment, losing them means a completely different, longer, and more toxic treatment course is required.
RR-TB (rifampicin-resistant TB) means resistant to rifampicin regardless of isoniazid status. It is treated the same as MDR-TB because rifampicin is the single most critical drug — losing it alone forces the same treatment redesign.
Pre-XDR-TB (WHO 2021 definition): MDR-TB or RR-TB plus resistance to any fluoroquinolone (levofloxacin or moxifloxacin). Fluoroquinolones are the most important second-line drug class, so losing them marks a serious escalation.
XDR-TB (extensively drug-resistant TB) — WHO revised definition from 2021: MDR/RR-TB plus resistance to any fluoroquinolone, plus resistance to at least one of bedaquiline or linezolid. Note that the pre-2021 XDR definition was different (MDR + fluoroquinolone + an injectable aminoglycoside like amikacin) — the updated definition reflects which drugs are now actually critical to modern regimens.
Why these distinctions matter: each category requires a completely different drug regimen with different durations, different monitoring requirements, and different expected outcomes. A person with MDR-TB has more treatment options than someone with pre-XDR-TB or XDR-TB, and treatment planning must account for exactly which drugs remain effective.
Global Burden — Scale and Distribution
Drug-resistant TB is not a rare edge case — it is a global public health emergency affecting hundreds of thousands of people every year, with a massive gap between those who need treatment and those who actually receive it.
According to the WHO Global TB Report 2023 (data for 2022):
- Approximately 410,000 people developed MDR/RR-TB worldwide
- 187,000 people died from MDR/RR-TB
- Only about 40% of estimated MDR-TB patients were detected and treated — a massive diagnostic gap that means most people with resistant TB go undetected
Highest burden countries: India, Russia, China, Pakistan, the Philippines, Ukraine, Uzbekistan, and Myanmar carry the majority of the global MDR-TB burden. Former Soviet states have particularly high MDR rates, partly due to historically poor TB program quality in the 1990s.
MDR-TB rates by context:
- Globally, about 3–4% of new TB cases are MDR — meaning someone who has never been treated for TB before still has a small but real chance of having a resistant strain (acquired from someone else)
- In former Soviet states: up to 25–35% of new cases are MDR
- In previously treated cases: MDR rates jump to 12–15% globally, and up to 50% or more in high-burden countries
Healthcare cost: Treating one MDR-TB patient in the United States costs $100,000–$400,000, compared to roughly $1,000–$2,000 for drug-sensitive TB. In low-income countries the absolute costs are lower, but still represent a severe strain on national health budgets.
Treatment success rate: About 60% for MDR-TB globally, compared to 85% or higher for drug-sensitive TB — though new regimens are improving this significantly.
How Resistance Arises — Genetic Mutations
Understanding how TB develops resistance helps explain why taking every dose of your medicine matters more than almost any other decision in TB treatment.
M. tuberculosis develops resistance exclusively through spontaneous chromosomal mutations — it cannot acquire resistance genes from other bacteria through horizontal gene transfer the way many other bacteria can. This is actually both good news and bad news: good, because resistance can't spread through bacterial communities like a virus; bad, because it means resistance is entirely self-generated, and the main driver is inadequate therapy.
The core mechanism: Every large bacterial population naturally contains a tiny number of mutants that are resistant to any given drug — perhaps 1 in every 100 million bacteria. If a patient takes only one drug at a time, or takes the wrong combination, or skips doses, the drug-sensitive bacteria die but those rare resistant mutants survive and multiply. Within weeks, the entire population is resistant.
Key resistance mutations:
- Isoniazid resistance: Most commonly caused by mutations in the katG gene, which encodes the enzyme that activates isoniazid as a prodrug — without activation, the drug can't work. katG mutations account for 50–70% of isoniazid resistance. Mutations in the inhA promoter (reducing binding to the drug's target) account for another 20–30%.
- Rifampicin resistance: Over 96% of cases involve mutations in the rpoB gene, which encodes the beta subunit of RNA polymerase — the molecule rifampicin binds to and blocks. This is why GeneXpert (the rapid molecular test) can detect rifampicin resistance in under 2 hours by sequencing just the rpoB "hot spot" region.
- Fluoroquinolone resistance: Mutations in gyrA and gyrB genes encoding DNA gyrase, which fluoroquinolones inhibit.
- Bedaquiline resistance: Mutations in atpE, which encodes the beta subunit of mycobacterial ATP synthase — bedaquiline's target.
How MDR-TB arises in practice: Inadequate therapy — wrong drug choices, inadequate doses, poor patient adherence, interrupted drug supply, or misdiagnosis — is the root cause of resistance development. Once MDR-TB strains exist, they can be transmitted person to person through the air exactly like drug-sensitive TB, which is why MDR-TB can spread in communities even among people who have never previously been treated for TB.
Second-Line Drugs for MDR-TB
When isoniazid and rifampicin are no longer effective, treatment requires second-line drugs. The WHO 2022 operational handbook organizes these into priority groups based on efficacy and safety evidence. Doctors aim to build a regimen using the highest-priority drugs first.
Group A — highest priority, include all three if susceptible:
- Levofloxacin or moxifloxacin (fluoroquinolones): inhibit DNA gyrase, disrupting bacterial DNA replication. These are the most effective second-line drug class available. Levofloxacin is preferred in most programs.
- Bedaquiline: inhibits mycobacterial ATP synthase — essentially starving the bacteria of energy. Highly effective and now central to modern MDR-TB treatment. Requires QT interval monitoring by ECG throughout treatment, as it prolongs the electrical conduction time in the heart.
- Linezolid: inhibits protein synthesis by binding the 50S ribosomal subunit. Highly effective but significantly toxic with long courses — can cause myelosuppression (bone marrow suppression leading to anemia and low white cell counts), peripheral neuropathy, and optic neuropathy. Regular blood counts and neurological monitoring are required.
Group B — add one or both:
- Clofazimine: originally developed for leprosy, repurposed for MDR-TB. Disrupts bacterial membrane function and generates reactive oxygen species that kill mycobacteria. Side effects include skin discoloration (red-brown pigmentation, reversible) and gastrointestinal upset.
- Cycloserine or terizidone: inhibit cell wall peptidoglycan synthesis through a different mechanism than isoniazid. Notable for psychiatric side effects including depression, anxiety, psychosis, and seizures — patients should be monitored closely and may need pyridoxine (vitamin B6) supplementation.
Group C — use only if Groups A and B are not available or not fully effective: Ethambutol, delamanid, pyrazinamide, imipenem-cilastatin or meropenem with clavulanate, amikacin, streptomycin, ethionamide or prothionamide, and p-aminosalicylic acid.
A note on injectable drugs (amikacin, kanamycin, capreomycin): Previously these were central to MDR-TB treatment, requiring patients to receive daily injections for 6–8 months. They have now been de-emphasized in WHO guidelines due to serious toxicity — permanent hearing loss (deafness) occurs in 15–30% of patients — and because better oral alternatives now exist.
The BPaL Regimen — A Revolution in MDR-TB Treatment
For decades, MDR-TB treatment was a 18–24 month ordeal involving injectable drugs that caused permanent deafness, a regimen of 5–6 pills daily with serious side effects, and a treatment success rate of only 50–55%. The development of the BPaL regimen represents one of the most significant advances in TB treatment in decades.
BPaL stands for Bedaquiline + Pretomanid + Linezolid. It is a 6-month, all-oral regimen for patients with pre-XDR and XDR-TB.
Pretomanid is a nitroimidazole antibiotic approved by the FDA in 2019. It works against both actively replicating bacteria and dormant bacteria (a key challenge in TB treatment), and received approval specifically as part of the BPaL combination for XDR-TB. It is not approved as a standalone agent.
BPaLM adds Moxifloxacin to the regimen — used when the strain is still susceptible to fluoroquinolones (pre-XDR-TB or MDR-TB without fluoroquinolone resistance).
Key clinical trial results:
- Nix-TB trial (Conradie et al., NEJM 2020): BPaL achieved 90% favorable outcomes in XDR-TB patients — a condition that had previously been nearly untreatable
- ZeNix trial (Conradie et al., Lancet 2022): Refined the optimal linezolid dose — found 600 mg daily achieved 93% favorable outcomes with lower toxicity than 1200 mg
- TB-PRACTECAL trial (2022): BPaLM achieved 89% treatment success vs 52% for standard of care, with only 6 months of treatment
WHO 2022 recommendation: BPaL or BPaLM is now the standard recommendation for pre-XDR-TB and XDR-TB. For standard MDR-TB (without fluoroquinolone resistance), WHO recommends BPaLM or a shorter all-oral 9-month regimen combining bedaquiline, levofloxacin, linezolid, clofazimine, and pyrazinamide.
Monitoring during BPaL treatment:
- QTc monitoring by ECG: bedaquiline prolongs the QT interval (risk of serious cardiac arrhythmia), especially when combined with clofazimine or moxifloxacin — monthly ECGs are required throughout treatment
- Audiometry: linezolid can rarely affect hearing; baseline and periodic testing
- Complete blood count (CBC): linezolid causes myelosuppression; monthly CBCs during treatment
- Liver function tests (LFTs): multiple drugs can cause hepatotoxicity
- Peripheral neuropathy assessment: linezolid neuropathy, assessed at each visit
Outcomes and Mortality in MDR-TB
The outcomes for drug-resistant TB are significantly worse than for drug-sensitive TB, but are improving rapidly with new treatment regimens.
Global treatment success rates (WHO 2023 report, largely pre-BPaL era data):
- MDR-TB: approximately 60% treatment success
- Pre-XDR-TB: approximately 38% treatment success
- XDR-TB: approximately 34% treatment success
With new BPaL-based regimens, these numbers are dramatically improving — the ZeNix trial showed 93% favorable outcomes in XDR-TB patients, a condition that was previously associated with 34% success.
Predictors of poor outcomes:
- HIV co-infection (raises mortality 2–3 times)
- Low CD4 count in HIV-positive patients
- Bilateral extensive cavitary disease on chest X-ray
- Low body mass index and malnutrition
- Older age
- Additional drug resistances beyond MDR
- Inconsistent adherence to the treatment regimen
Treatment failure is defined as a confirmed positive sputum culture at 8 months or later while still on treatment — this requires full regimen review and usually additional drug susceptibility testing to identify any further resistances that have developed.
IRIS in HIV-MDR co-infection: Immune Reconstitution Inflammatory Syndrome is particularly challenging in patients who have both HIV and MDR-TB. When antiretroviral therapy (ART) successfully reconstitutes the immune system, the newly active immune response can paradoxically worsen TB lesions, causing fever, enlarged lymph nodes, and worsening chest X-rays despite bacteria actually being killed. Timing ART initiation relative to MDR-TB treatment requires careful specialist judgment.
Mortality in context: Untreated MDR-TB is nearly universally fatal over time. Among treated patients, mortality ranges from approximately 5–10% in high-resource settings with access to second-line drugs and comprehensive supportive care, to 30–40% in high-burden, resource-limited settings.
Programmatic Challenges — Cost, Adherence, and Access
Even with better drugs available, translating MDR-TB treatment advances into real-world outcomes for patients in low-income, high-burden settings involves enormous practical challenges.
Drug cost and supply: Bedaquiline and linezolid were initially extremely expensive, though prices have fallen significantly with the introduction of generic production. A full BPaL course can still cost thousands of dollars — prohibitive without subsidized supply in countries where most MDR-TB patients live. The Global Drug Facility (Stop TB Partnership) is the central procurement mechanism providing subsidized MDR-TB drugs to high-burden countries, but supply chains remain fragile.
Duration: Even with the new 6-month BPaL regimens, MDR-TB treatment is at minimum double the duration of drug-sensitive TB. The prior standard was 18–24 months. Maintaining adherence across many months while managing side effects is a profound challenge, especially for patients who also need to work and support families.
Monitoring requirements: Monthly blood draws, ECG monitoring, audiometry, and clinic visits are required to catch potentially serious side effects early. In areas with limited laboratory infrastructure or transportation barriers, maintaining this schedule is extremely difficult.
Social support as medicine: Multiple trials and observational studies have shown that providing food baskets, transportation reimbursements, and conditional cash transfers significantly improves MDR-TB treatment completion rates. These are not charity — they are clinically effective interventions. The WHO strongly recommends patient-centered support packages as part of MDR-TB care.
Drug-resistant TB in children: Historically, children with MDR-TB were severely under-diagnosed (pediatric TB often lacks the sputum needed for drug susceptibility testing) and under-treated (adult formulations are not appropriate for children). WHO estimates that in 2019, only about 3% of children with MDR-TB received appropriate treatment. Progress has been made — child-friendly dispersible formulations of bedaquiline (called Paedbedaquiline) have now been approved for children, and WHO guidance now specifically addresses pediatric MDR-TB management.
Preventing Drug Resistance — The Essential Strategy
The most important fact about MDR-TB is this: it is entirely preventable through correct treatment of drug-sensitive TB. MDR-TB is largely a man-made catastrophe caused by inadequate treatment programs. The same principles that prevent resistance in individual patients, applied consistently at a population level, would eliminate most new MDR-TB.
Never-miss priorities to prevent resistance from developing:
- Ensure proper diagnosis first: always perform drug susceptibility testing on new cases — using standard HRZE on a patient who unknowingly has RR-TB effectively gives them monotherapy with only two active drugs
- Adequate drug supply: interruptions in drug supply force patients to take incomplete regimens or take drugs one at a time, directly selecting for resistance
- Appropriate weight-based dosing: under-dosing creates subtherapeutic blood levels that allow resistant mutants to survive
- Directly observed therapy (DOT) or video-DOT for high-risk patients: watching patients take medication (or using video calls) catches adherence problems early
- Patient education: helping patients genuinely understand why every single dose matters — not just following orders but understanding the biological mechanism — improves adherence
- Early monitoring for hepatotoxicity: catching drug-induced liver injury early allows safe regimen modification, preventing patients from self-stopping treatment
Infection control to prevent transmission of existing resistant strains:
- Isolate MDR-TB patients in negative-pressure rooms in hospitals
- N95 respirators (not surgical masks) for healthcare staff
- Rapid GeneXpert testing to identify rifampicin resistance within 2 hours — enabling immediate appropriate isolation and treatment adjustment
Contact investigation for MDR-TB: All household contacts of confirmed MDR-TB patients should be tested. Preventive therapy for MDR-TB contacts is more complex than for drug-sensitive TB contacts — there is no established standard regimen equivalent to 6 months of isoniazid for drug-sensitive contacts. Fluoroquinolone-based preventive therapy has been studied, including in the TB-CHAMP trial in children, and may be offered depending on local guidelines and the drug susceptibility profile of the source case.
Whole-genome sequencing (WGS): Increasingly used in high-income settings to map MDR-TB transmission chains with precision, identify outbreak clusters in healthcare settings or communities, and guide infection control responses. WGS can determine whether two cases are genetically linked with far more resolution than traditional fingerprinting methods, enabling public health teams to interrupt transmission chains that would otherwise be invisible.
Research Papers
- Search PubMed — Nix-TB trial demonstrating that the BPaL regimen (bedaquiline, pretomanid, linezolid) achieved 90% favorable outcomes in patients with XDR-TB and treatment-intolerant MDR-TB, establishing the foundation of modern MDR-TB treatment.
- Search PubMed — ZeNix trial showing that linezolid 600 mg daily in BPaL achieved 93% favorable outcomes with better tolerability than 1200 mg, refining the optimal BPaL regimen for clinical practice.
- Search PubMed — Comprehensive review of TB epidemiology, pathogenesis, diagnosis, and treatment providing essential background on the global TB burden including drug-resistant forms.
- Search PubMed — Authoritative review of tuberculosis covering the biology of resistance, second-line drug mechanisms, and the state of MDR-TB treatment as of the early era of bedaquiline development.
- Search PubMed — Overview of MDR-TB treatment advances documenting the shift from injectable-based to all-oral regimens and the early evidence supporting bedaquiline and delamanid.
- Search PubMed — Landmark review of tuberculosis pathogenesis and management covering the immunological basis of TB disease and the evidence base for standard and second-line drug treatment.
- Search PubMed — Analysis of what we know about how TB kills, including the contribution of MDR-TB to global TB mortality and the gaps in treatment delivery in high-burden settings.
- Search PubMed — TRUNCATE-TB trial exploring short-course intensive treatment strategies, contributing to understanding of bacterial killing kinetics relevant to MDR-TB regimen design.
- Search PubMed — Updated American Thoracic Society and CDC clinical practice guidelines for drug-susceptible TB treatment, providing the standard-of-care context against which MDR-TB outcomes are measured.
- Search PubMed — Modeling study on the population-level dynamics of TB drug resistance, showing how treatment program quality determines resistance rates at national and global levels.
Connections
- All Bacteria
- Mycobacterium Tuberculosis — Main Hub
- TB Treatments Overview
- HRZE First-Line Regimen
- TB Diagnosis — TST, IGRA, Imaging, Culture
- HIV — Co-infection and Immune Suppression