Tuberculosis in Vulnerable Groups: HIV, Children, Pregnancy, and the Elderly
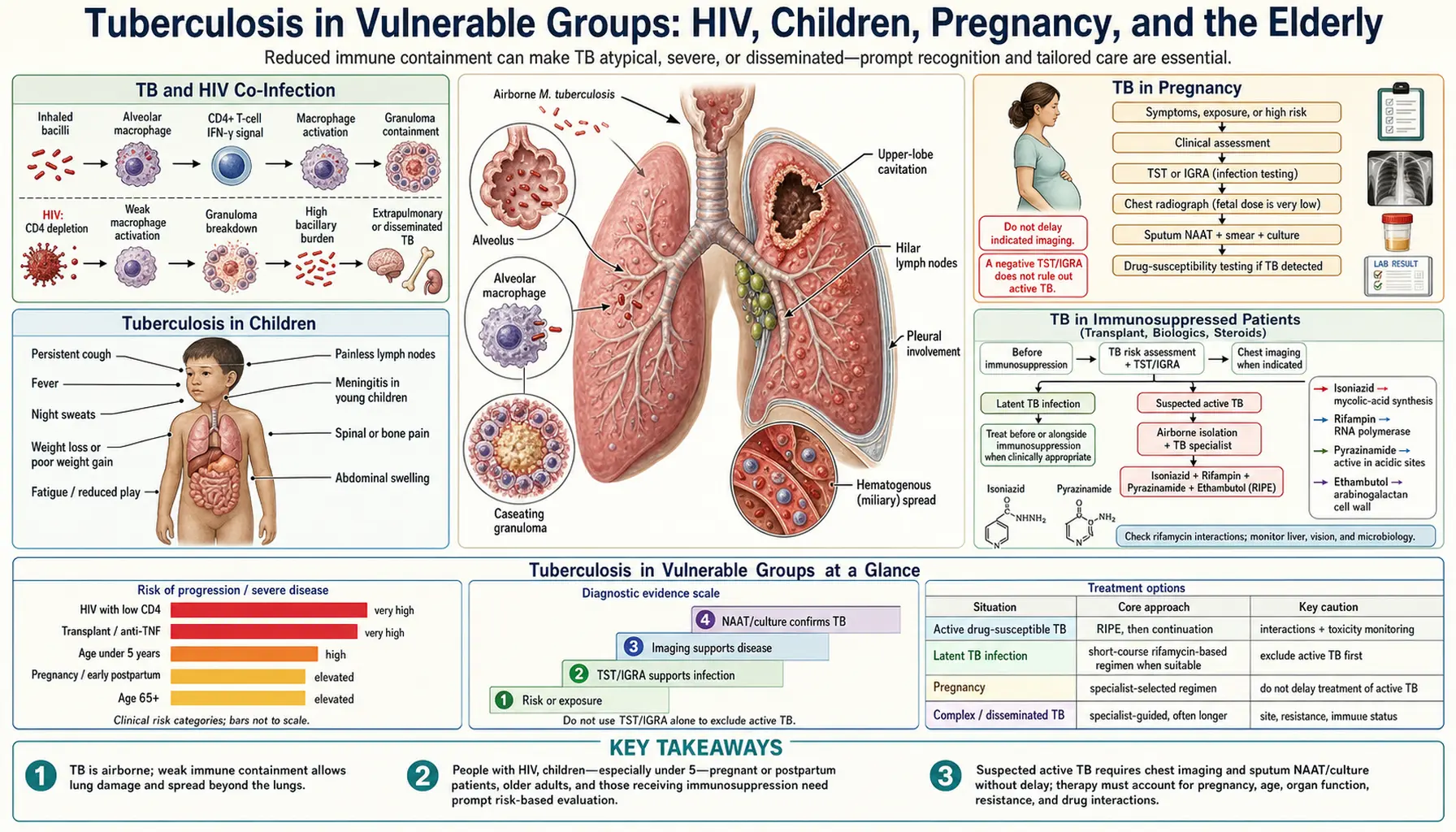
While anyone exposed to Mycobacterium tuberculosis can develop tuberculosis, certain groups face dramatically higher risks of infection, faster progression from latent to active disease, and far worse outcomes — and they often present with atypical symptoms that are easy to miss. HIV-positive individuals, young children, pregnant women, the elderly, transplant recipients, people on immune-suppressing biologics, those living with diabetes, and people in crowded institutional settings like prisons all occupy this vulnerable category. Understanding how TB behaves differently in each group is essential, because standard checklists — persistent cough, night sweats, cavities on X-ray — frequently do not apply, and delays in diagnosis cost lives.
Table of Contents
- TB and HIV Co-Infection
- Tuberculosis in Children
- TB in Pregnancy
- TB in Immunosuppressed Patients
- TB in the Elderly
- TB in Prisons, Homeless Shelters, and High-Risk Settings
- Diabetes and TB
- Malnutrition and TB
- Research Papers
- Connections
- Featured Videos
TB and HIV Co-Infection
The intersection of HIV and tuberculosis represents one of the most lethal partnerships in modern infectious disease. Without HIV, a person who has been infected with TB bacteria and carries it in a latent state faces roughly a 5–10% lifetime risk that it will reactivate into active disease. With HIV, that same lifetime risk becomes a 5–10% annual risk — a 50- to 100-fold increase per year. The numbers are stark: TB is the single leading cause of AIDS-related death globally, responsible for approximately one in four HIV deaths.
The mechanism is direct. HIV destroys CD4+ T cells — specifically the CD4+ T helper cells that coordinate the immune response to mycobacteria. These are the very cells that form and maintain the granulomas (tight clusters of immune cells) that wall off TB bacteria and prevent them from spreading. As CD4+ counts fall below 200 cells per microliter, granuloma integrity collapses, bacteria escape containment, and disseminated disease becomes possible. Below 50 cells per microliter, the immune system is essentially incapable of mounting any organized response to TB.
This immune failure profoundly changes how TB looks in HIV-positive patients. The classic presentation — productive cough, upper lobe cavities on chest X-ray, positive sputum smear — depends on the immune response itself being strong enough to cause tissue damage, cavity formation, and bacterial shedding. In advanced HIV, none of that happens. Instead, TB in HIV-positive patients is frequently:
- Smear-negative: Far fewer bacteria in the sputum because lung damage is muted, making standard microscopy miss the diagnosis.
- Extrapulmonary: Lymph nodes (peripheral lymphadenopathy is the most common presentation), the central nervous system (TB meningitis), the bloodstream (miliary TB), bone marrow, liver, and abdomen are all common sites.
- Radiologically atypical: No cavities, sometimes a normal chest X-ray, or only subtle hilar adenopathy — because the immune response that creates the classic X-ray findings is absent.
A critical complication unique to HIV-TB co-infection is Immune Reconstitution Inflammatory Syndrome (IRIS). When antiretroviral therapy (ART) is started and the immune system begins to recover, the newly revived immune cells mount an aggressive inflammatory response to the TB bacteria still present in tissues. This paradoxical deterioration — appearing to get worse just when treatment should be helping — can manifest as worsening lymphadenopathy, fever, new pulmonary infiltrates, or expanding CNS lesions. Management typically requires corticosteroids to dampen the inflammatory surge without stopping either HIV or TB treatment.
Drug interactions add further complexity. Rifampicin, the cornerstone of TB therapy, is a potent inducer of the CYP3A4 liver enzyme system, which accelerates the metabolism of many HIV antiretrovirals — particularly protease inhibitors and some non-nucleoside reverse transcriptase inhibitors — to the point of rendering them ineffective. The solution is either rifabutin (a weaker CYP inducer that can substitute for rifampicin) or switching to an ART regimen compatible with rifampicin such as efavirenz-based or dolutegravir-based therapy. TB screening is mandatory for all HIV-positive individuals at diagnosis and annually in high-burden settings — it is one of the most important and cost-effective interventions in HIV care.
Tuberculosis in Children
Children under five years old are at extreme risk of rapid, severe TB disease, and they are also among the hardest to diagnose. In an adult, years typically separate initial TB infection from potential reactivation. In a young child, that window can collapse to weeks or months — the progression from inhaling bacteria to developing serious disease can be startlingly fast.
The reason is immunological. Children's immune systems, particularly in the first few years of life, cannot form the tight, organized granulomas that contain TB bacteria in healthy adults. The granulomas that do form are loose and leaky, allowing bacteria to spread through the bloodstream to distant organs before the child's body can mount an effective containment response. This is why the two most feared complications of childhood TB — miliary TB (bacterial seeding of all organs via the bloodstream) and TB meningitis — are predominantly diseases of young children, not adults.
The clinical picture is further complicated by what childhood TB does not look like. Adults with pulmonary TB characteristically have:
- Upper lobe cavities on X-ray (bacteria concentrating in high-oxygen areas)
- Positive sputum smears (high bacterial loads being coughed up)
- A recognizable constellation of cough, fever, and weight loss
Children, especially those under five, instead show a primary complex pattern: hilar lymph node enlargement visible on X-ray, consolidation in a lower or middle lobe (where primary infection is most likely to occur), and minimal or no cough. The disease is paucibacillary — there are very few bacteria present at any given site — which means sputum smears are almost always negative, and even GeneXpert molecular testing has reduced sensitivity in children because there is simply not enough bacterial DNA to detect reliably. IGRA blood tests are also less reliable in infants under six months.
Because children cannot produce sputum on demand, obtaining diagnostic specimens requires either gastric lavage (washing stomach contents where swallowed respiratory secretions accumulate overnight) or induced sputum using hypertonic saline — both uncomfortable and requiring specialized facilities. Stool-based GeneXpert testing is an emerging approach that may simplify pediatric diagnosis.
Treatment uses the same four drugs as adults — isoniazid, rifampicin, pyrazinamide, ethambutol — but doses are weight-adjusted and need regular recalculation as children grow. BCG vaccination at birth provides approximately 60–80% protection against the most severe forms of childhood TB (meningitis and miliary disease), though its protection against pulmonary TB in adults is variable. Congenital TB — transmission from mother to fetus via the placenta or from infected amniotic fluid — is rare but devastating, presenting in the first weeks of life with fever, failure to thrive, and hepatosplenomegaly.
TB in Pregnancy
Tuberculosis is one of the most common serious infections complicating pregnancy in high-burden countries, and it carries consequences not just for the mother but for the developing baby. Active TB during pregnancy approximately triples the risk of premature birth and low birth weight, and in severe cases increases perinatal mortality. The risks to the baby are compounded by the fact that TB symptoms — fatigue, weight loss, mild fever — can be attributed to normal pregnancy changes, delaying diagnosis by weeks or months.
Pregnancy creates a genuine physiologic dilemma for TB diagnosis. Chest X-ray, the standard screening tool, is approached with caution (though with appropriate abdominal shielding, radiation exposure is minimal and considered safe). The immune shifts of pregnancy — particularly the shift toward a Th2-dominant state that prevents immune rejection of the fetus — may blunt the Th1 immune responses that contain TB, theoretically increasing reactivation risk, though the evidence for dramatically increased reactivation during pregnancy itself is mixed. The postpartum period carries a clearer risk of worsening disease.
Treatment during pregnancy follows the standard HRZE regimen — isoniazid, rifampicin, pyrazinamide, and ethambutol — which is considered safe for both mother and fetus, with one critical exception: streptomycin must never be used in pregnancy. An aminoglycoside antibiotic, streptomycin crosses the placenta and is ototoxic to the developing fetal ear, causing sensorineural deafness. Other second-line injectable drugs (kanamycin, amikacin, capreomycin) carry the same risk and are similarly contraindicated.
Pyridoxine (vitamin B6) supplementation at 25–50 mg daily is essential for pregnant women on isoniazid, both because pregnancy increases pyridoxine requirements generally and because isoniazid blocks pyridoxine metabolism, increasing the risk of peripheral neuropathy.
A special management challenge arises when a mother has smear-positive pulmonary TB at delivery. The baby is at high risk of TB infection but cannot yet receive BCG until they are at least a few weeks old and ideally free of active TB themselves. The standard approach is to start the baby on isoniazid preventive therapy (IPT) for six months, then test for TB infection, and only then give BCG. Breastfeeding is considered safe while the mother is on standard TB treatment — the amounts of drug that pass through breast milk are insufficient to treat an infant but also too small to cause harm.
Vertical transmission (congenital TB) is rare but should be suspected in any newborn with unexplained fever, hepatosplenomegaly, or respiratory distress in the first few weeks of life, particularly when the mother has active or recently diagnosed TB.
TB in Immunosuppressed Patients (Transplant, Biologics, Steroids)
Beyond HIV, a wide range of medical treatments that intentionally suppress the immune system create dangerous vulnerability to TB — particularly reactivation of latent infection that may have been dormant for decades. Three major groups deserve specific attention: patients on biologic medications, solid organ and bone marrow transplant recipients, and people on prolonged high-dose corticosteroids.
Biologic medications and TNF inhibitors represent the highest-profile risk in this category. TNF-alpha (tumor necrosis factor) is not just a pro-inflammatory signaling molecule — it is essential for forming and maintaining the granulomas that contain latent TB. Block TNF, and granuloma integrity fails, releasing bacteria that have been contained for years or decades. The risk is especially pronounced with infliximab and adalimumab (monoclonal antibodies that neutralize TNF completely), where reactivation TB risk is increased approximately 7-fold compared to background rates. Etanercept (which intercepts TNF receptors rather than neutralizing free TNF) carries a somewhat lower risk. Other biologics — IL-6 inhibitors (tocilizumab), IL-17 inhibitors (secukinumab), JAK inhibitors (tofacitinib) — also increase TB risk through different immune pathways.
The clinical standard before starting any TNF inhibitor or other high-risk biologic is mandatory TB screening: an IGRA (preferred, as it is more specific than the TST in BCG-vaccinated individuals) or TST. If the result is positive (indicating latent TB), the patient must complete a full course of LTBI treatment — typically nine months of isoniazid or a shorter four-month rifampicin regimen — before starting the biologic. This screening and treatment step has substantially reduced, though not eliminated, reactivation TB in patients on biologics.
Transplant recipients face compounded immunosuppression: high-dose corticosteroids at the time of transplant, calcineurin inhibitors (tacrolimus, cyclosporine), antiproliferative agents (mycophenolate), and sometimes induction biologics — all operating simultaneously. TB rates in transplant recipients in high-burden countries can be 20–74 times higher than in the general population, and TB in this setting is frequently disseminated (extrapulmonary) and carries high mortality.
A critical drug interaction complicates TB treatment in transplant recipients: rifampicin is one of the most potent known inducers of the CYP3A4 and P-glycoprotein drug transport system. Tacrolimus and cyclosporine — the immunosuppressants that prevent organ rejection — are metabolized almost entirely by CYP3A4. When rifampicin is added, their blood levels can drop by 70–90%, putting the patient at immediate risk of acute rejection. Managing this requires either massively increasing tacrolimus doses (sometimes 3–5 times the usual dose) with daily therapeutic drug monitoring, or substituting rifabutin, a weaker CYP inducer that still provides antituberculosis activity but causes much smaller reductions in calcineurin inhibitor levels. Rifabutin is now the preferred choice in most transplant TB treatment protocols.
Corticosteroids at doses equivalent to prednisone 15 mg per day or more for four or more consecutive weeks are sufficient to meaningfully impair TB immunity. LTBI screening is recommended before planned prolonged steroid therapy in individuals who may have been exposed to TB.
TB in the Elderly — Atypical Presentation and Reactivation
In low-burden countries like the United States, the majority of active TB cases in older adults are not new infections — they are reactivations of infections acquired in childhood or young adulthood, sometimes 50 or 60 years earlier. The bacteria remained contained within calcified granulomas in the lungs or lymph nodes for decades, held in check by a functioning immune system. As that immune system weakens with age (a process called immunosenescence), the containment breaks down, and bacteria that have been dormant for half a century begin to multiply again.
This reactivation pattern in older adults frequently presents in ways that bear little resemblance to classic TB descriptions. Instead of fever and night sweats, older patients may have:
- Confusion or delirium — particularly in the context of miliary or CNS TB
- Unexplained weight loss attributed to malignancy or depression
- Falls or functional decline without obvious fever
- A chronic low-grade cough dismissed as chronic obstructive pulmonary disease or heart failure
Cognitive impairment makes symptom history unreliable — the patient cannot accurately describe when symptoms began, whether they have night sweats, or how much weight they have lost. Caregivers and family members become the essential history source.
Comorbidities accumulate in older patients and interact with TB at every level: diabetes impairs immune response (see below), kidney disease alters drug clearance, heart failure makes fluid management during treatment more complex, and liver disease increases hepatotoxicity risk from isoniazid and rifampicin. Polypharmacy creates additional drug interaction risk, particularly with the strong enzyme-inducing effects of rifampicin on warfarin, statins, calcium channel blockers, and many other medications commonly used in older adults.
Immunosenescence also reduces diagnostic test sensitivity. The tuberculin skin test (TST) depends on a functioning T-cell response — in older adults with blunted immune reactivity, false-negative TST results are common. IGRA tests are more sensitive in immunosenescence than TST but are also not perfectly reliable. Chest X-ray findings may be obscured by longstanding lung disease or may show only old healed calcifications from the original infection rather than new active disease.
Drug-induced hepatotoxicity from isoniazid and rifampicin occurs at higher rates in older patients, requiring more frequent liver function monitoring, particularly in the first two months of treatment. Age over 35 was historically considered a relative contraindication to isoniazid preventive therapy for exactly this reason, though current guidelines have moved away from strict age cutoffs in favor of individualized benefit-risk assessment.
TB in Prisons, Homeless Shelters, and High-Risk Settings
Tuberculosis does not affect all members of society equally — it concentrates in settings of poverty, crowding, and marginalization with a consistency that has been documented across centuries and continents. Incarcerated individuals carry TB rates that are typically 10 to 50 times higher than the general population, varying by country and income level. In some low-income countries, prison TB rates exceed 1,000 per 100,000 — compared to general population rates of 50–100 per 100,000.
The reasons are structural and compounding. Prisons and jails concentrate several major TB risk factors simultaneously:
- Overcrowding that dramatically increases the probability of inhaling aerosolized bacteria from an infectious individual
- Poor ventilation in older facilities — cells and dormitories with little air exchange allow infectious aerosols to accumulate
- High HIV prevalence among incarcerated populations due to high rates of injection drug use prior to incarceration
- Malnutrition from inadequate dietary provision
- Inadequate healthcare access — infectious TB cases may go undetected and untreated for extended periods, continuing to transmit
- High turnover — individuals released from custody while still infectious carry TB back into communities and into households
Homeless shelters, migrant worker housing, and refugee camps share many of these structural risk factors. Homeless individuals face additional barriers: no stable address for medication pickup, limited access to clinics, high rates of alcohol use (which increases TB risk independently), and poor nutritional status.
Healthcare workers in TB-endemic settings — prisons, homeless shelters, high-burden clinics, hospital TB wards — face occupational exposure risk and should be on structured surveillance programs: annual IGRA or TST testing, prompt evaluation of conversions, N95 respirator use (not surgical masks, which are inadequate for airborne precautions) when caring for suspected or confirmed TB patients, and negative-pressure isolation rooms for infectious patients. Nosocomial TB transmission in healthcare settings — including TB transmitted to hospital patients from infectious patients in other wards — remains a documented problem in high-burden countries.
Contact investigation — the systematic identification, testing, and treatment of all close contacts of a newly identified infectious TB case — is the cornerstone of outbreak control in congregate settings. All household members, cellmates, shelter co-residents, and workplace contacts who shared air with an infectious case for extended periods should be tested. Those with latent TB infection identified through contact investigation should be offered and strongly encouraged to complete preventive therapy.
Diabetes and TB — A Bidirectional Risk
The relationship between diabetes and tuberculosis is bidirectional and increasingly important as the global diabetes epidemic expands into the same low- and middle-income countries where TB remains endemic. Diabetes approximately triples the risk of developing active TB after infection. In countries like India, Mexico, and Indonesia, where both diseases are prevalent, diabetes now accounts for an estimated 15–20% of all active TB cases — making it one of the most significant TB risk factors in the modern era.
The mechanisms by which diabetes impairs TB immunity are multiple. Chronic hyperglycemia directly impairs the function of neutrophils and macrophages — the front-line immune cells that first encounter TB bacteria after inhalation. Macrophage killing of TB bacteria is less efficient in high-glucose environments. Vitamin D levels are frequently lower in diabetic patients, which matters because vitamin D activates macrophages to produce cathelicidin, an antimicrobial peptide that directly kills TB bacteria. Higher glucose concentrations in alveolar fluid may also theoretically provide better growth conditions for bacteria. The result is slower bacterial clearance, higher bacterial loads, and a greater probability that infection progresses to active disease.
The relationship also runs in reverse: active TB worsens diabetic control. The systemic inflammatory response to active TB infection drives stress hyperglycemia through cortisol and cytokine-mediated insulin resistance, making blood glucose management harder during treatment. Poorly controlled diabetes during TB treatment is associated with slower sputum conversion, higher relapse rates, and worse survival — creating a vicious cycle where each disease amplifies the other.
Drug interactions complicate management. Rifampicin's potent CYP enzyme induction accelerates the metabolism of some oral diabetes medications. Sulfonylureas (glipizide, glibenclamide) are partially metabolized via CYP2C9, and rifampicin can reduce their blood levels and effectiveness. Fluoroquinolones — used as second-line TB drugs (levofloxacin, moxifloxacin) — cause significant glucose dysregulation in both directions: hypoglycemia and hyperglycemia have both been reported, requiring careful blood sugar monitoring when these agents are used. Metformin is generally preferred as the diabetes drug least affected by these interactions.
Clinical management during TB treatment in a diabetic patient requires: more frequent blood glucose monitoring (aiming for HbA1c below 7–8%), adjustment of diabetes medication doses if rifampicin is started, nutritional support, and closer follow-up for treatment response. TB treatment outcomes in diabetics — particularly sputum conversion and relapse rates — are worse than in non-diabetics, underscoring the need for intensified monitoring rather than just standard protocol.
Malnutrition and TB — The Oldest Partnership
The link between malnutrition and tuberculosis predates modern medicine by centuries. TB was called "consumption" because it consumed its victims — but the causal arrow ran both ways: malnourished individuals were more likely to develop active disease, and active TB consumed the body's nutritional reserves in a downward spiral. The great TB epidemics of the 18th and 19th centuries in Europe coincided with poverty, urbanization, and widespread nutritional deprivation. Modern data from high-burden countries confirms what historical observers documented: undernutrition remains one of the most powerful population-level risk factors for TB, responsible for an estimated 20% of the global TB burden.
Vitamin D occupies a central mechanistic role. When macrophages successfully engulf TB bacteria, vitamin D receptor activation is required to trigger the production of cathelicidin (LL-37), an antimicrobial peptide that directly disrupts the bacterial cell membrane. Vitamin D deficiency — extremely common in high-burden TB populations, especially those with limited sun exposure, high-melanin skin, or diets low in vitamin D-rich foods — impairs this killing step, allowing bacteria to survive inside macrophages that should be eliminating them.
Zinc deficiency impairs T-cell proliferation and differentiation, weakens NK cell activity, and reduces the capacity for Th1 immune responses — the type most critical for TB containment. Protein-energy malnutrition reduces immune competence across nearly every measurable dimension: lower lymphocyte counts, reduced antibody production, impaired phagocyte function, weakened mucosal immunity. A BMI below 18.5 kg/m² is an independent predictor of TB treatment failure, relapse after successful completion, and death — independent of other risk factors.
Malnutrition also impairs drug handling. Malnourished patients have reduced plasma protein binding (drugs circulate free and may be eliminated faster), altered gastric motility affecting absorption, and reduced liver enzyme function affecting metabolism. Drug toxicity risk increases — malnourished patients on isoniazid have lower pyridoxine reserves and are more prone to peripheral neuropathy; pyrazinamide hepatotoxicity may be more frequent in severely malnourished patients.
Nutritional support during TB treatment measurably improves outcomes. Studies in high-burden countries have shown that food supplementation programs reduce early mortality, speed bacterial clearance, and improve treatment completion rates — particularly in severely malnourished patients. Specific micronutrient supplementation as adjunctive TB therapy has been investigated in several trials:
- Vitamin D: Randomized controlled trials have shown modest acceleration of sputum conversion in vitamin D-deficient patients receiving high-dose supplementation, with the largest effect in patients with certain vitamin D receptor gene variants. Not yet standard of care but increasingly incorporated into clinical guidance.
- Zinc: Evidence is less consistent, but some trials suggest benefit in immune recovery, particularly in children.
- Multi-micronutrient supplementation: Several trials show improvement in weight gain and immunological markers; effect on definitive TB outcomes (relapse, mortality) is less clear.
Practically speaking, every TB patient should have their nutritional status assessed at diagnosis, receive dietary counseling, and be connected with food support programs where available. Correcting severe malnutrition is not ancillary to TB treatment — it is part of it.
Research Papers
- Search PubMed — Landmark Lancet paper establishing that TB is the leading cause of AIDS deaths globally and defining the scope of the HIV-TB co-epidemic, with risk quantification and management recommendations.
- Kwan CK & Ernst JD, 2011 (PMID 21338485) — Comprehensive Clinical Microbiology Reviews analysis of HIV-TB co-infection, covering pathogenesis, immune mechanisms of granuloma failure, IRIS, and drug interactions between rifampicin and antiretrovirals.
- Search PubMed — Classic description of the natural history and spectrum of childhood TB, explaining why children under five present with primary complex patterns, paucibacillary disease, and disproportionate rates of miliary and meningeal TB.
- Search PubMed — Review of TB in pregnancy covering epidemiology, risks of vertical transmission, safety of standard regimens, management of drug interactions, and postpartum care of mother-infant pairs.
- Search PubMed — NEJM review of latent TB infection management across all vulnerable groups, covering indications for treatment, choice of regimen, and monitoring requirements in immunosuppressed patients.
- Search PubMed — European Respiratory Journal consensus statement on TB in high-risk populations including prison settings, healthcare workers, and migrants, with guidance on contact investigation and preventive therapy.
- Search PubMed — Nature Reviews Disease Primers comprehensive overview of TB globally, including epidemiology in vulnerable groups, pathogenesis of reactivation, and the impact of immunosuppression across multiple medical contexts.
- Search PubMed — Lancet analysis of social determinants of TB, quantifying the contributions of diabetes, smoking, alcohol use, malnutrition, and indoor air pollution to the global TB burden, with prevention implications.
- Search PubMed — Lancet review of advances in TB, including an in-depth treatment of the diabetes-TB bidirectional relationship, mechanisms of mutual worsening, and treatment outcome data.
- Search PubMed — Lancet seminal overview of TB as a global disease, with detailed analysis of co-morbidities, immunosuppressed populations, and the nutritional deficiency–TB relationship across historical and contemporary settings.
Connections
- Mycobacterium Tuberculosis — Main Hub
- TB Symptoms & Diagnosis Hub
- HIV — Disease Overview
- Prevention, BCG Vaccine, and Screening
- Infectious Disease Category
- All Bacteria — Category Index