First-Line TB Treatment: The HRZE Regimen
The HRZE regimen — four precisely chosen drugs, taken daily for six months — stands as one of medicine's great success stories. When taken properly and completed in full, this combination cures more than 95% of drug-sensitive tuberculosis cases worldwide. Its design reflects decades of clinical trials, understanding of how Mycobacterium tuberculosis hides inside the body, and the biological necessity of killing every last dormant bacterium to prevent relapse. Understanding how each drug works and why the regimen is structured as it is helps patients and caregivers recognize why completing the full course matters just as much as starting it.
Table of Contents
- The Four First-Line Drugs — What Each One Does
- The 2HRZE/4HR Standard Regimen
- Weight-Based Dosing
- Monitoring Parameters During HRZE Treatment
- Managing Hepatotoxicity — When to Hold and Rechallenge
- Pyridoxine and Neuropathy Prevention
- Special Populations — HIV and Rifampicin Drug Interactions
- TB Treatment in Pregnancy and Breastfeeding
- Research Papers
- Connections
- Featured Videos
The Four First-Line Drugs — What Each One Does
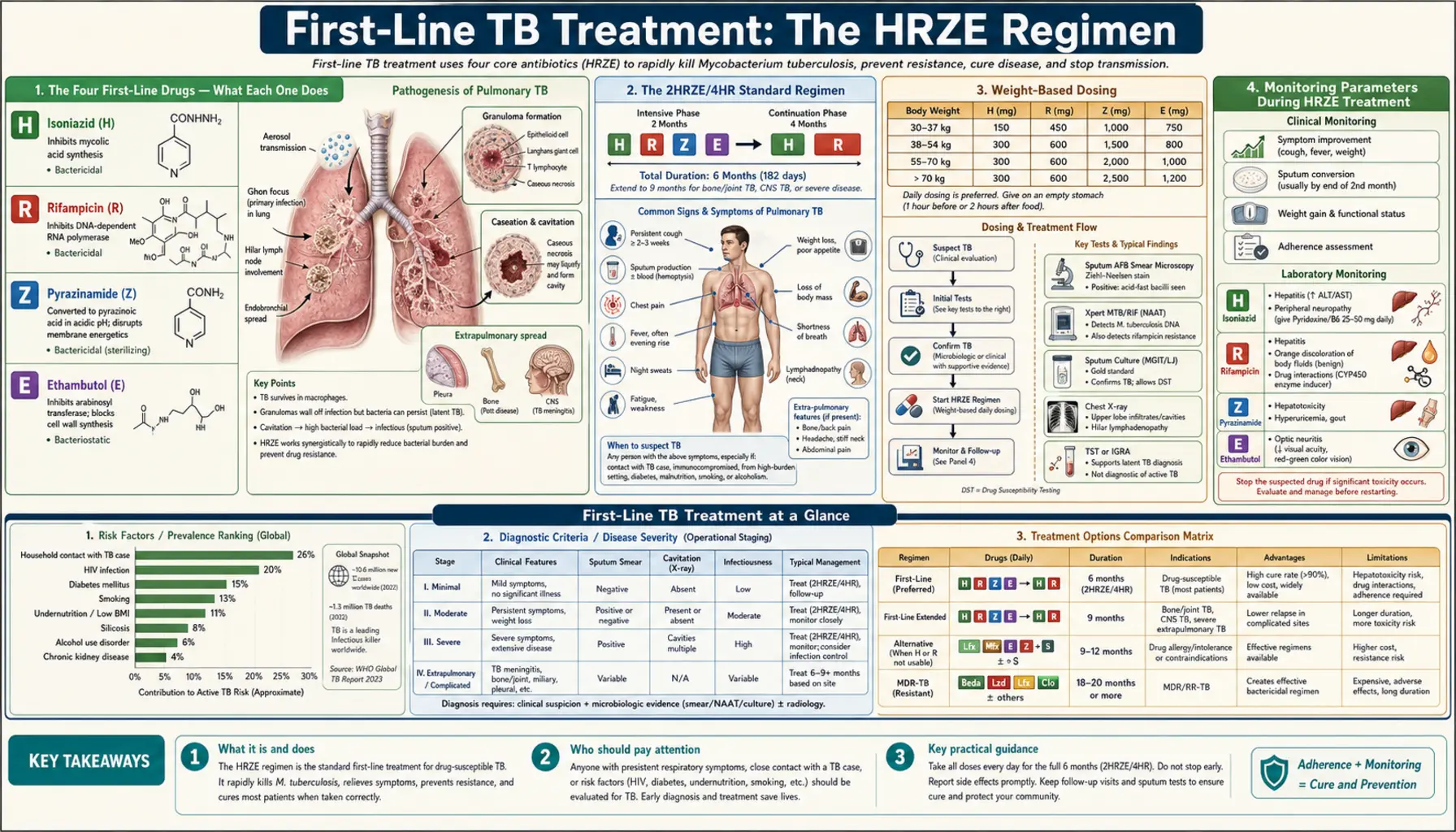
The letters H, R, Z, and E stand for isoniazid, rifampicin, pyrazinamide, and ethambutol — four drugs with different mechanisms, different targets, and complementary roles. Together they hit the bacterium from multiple angles simultaneously, dramatically reducing the chance that any resistant mutants survive.
Isoniazid (H)
Isoniazid is the most potent bactericidal drug in the regimen and kills rapidly dividing bacteria within hours of the first dose. It targets the waxy outer coat that makes tuberculosis so difficult to kill — a lipid-rich cell wall built largely from long-chain fatty acids called mycolic acids. Isoniazid is actually a prodrug: it must first be activated inside the bacterium by an enzyme called KatG (a catalase-peroxidase). Once activated, it forms a covalent adduct that inhibits InhA, the enoyl-ACP reductase responsible for the last step of mycolic acid synthesis. Without new mycolic acids, the cell wall cannot be maintained and the bacterium dies rapidly. Discovered in 1952, isoniazid is specific to mycobacteria — it has no effect on other bacteria — and remains among the cheapest and most effective antimycobacterial drugs ever developed. Its main toxicities are liver inflammation and peripheral neuropathy (see the pyridoxine section below).
Rifampicin (R)
Rifampicin kills both rapidly and slowly dividing bacteria, including semi-dormant populations that isoniazid alone cannot reach, making it the essential sterilizing backbone of the regimen. It works by binding directly to the beta subunit of bacterial RNA polymerase (encoded by the rpoB gene), physically blocking the elongation of RNA chains and halting transcription. Without new messenger RNA, the bacterium cannot produce proteins and dies. Discovered in 1957 from a soil bacterium, rifampicin is also active against dormant bacteria in necrotic (caseous) lesions — a critical property for preventing late relapse. Its most conspicuous side effect is harmless but alarming: it turns urine, tears, sweat, and saliva orange-red, and permanently stains soft contact lenses. More clinically significant is its role as a potent inducer of cytochrome P450 enzymes (especially CYP3A4 and CYP2C9), dramatically reducing the blood levels of dozens of co-administered drugs including HIV antiretrovirals, oral contraceptives, warfarin, and transplant immunosuppressants.
Pyrazinamide (Z)
Pyrazinamide is the key sterilizing drug that allowed the TB regimen to be shortened from nine months to six. Its unique value lies in where it works: it is most active in acidic environments — inside the oxygen-poor phagosome of macrophages, and inside necrotic caseous foci where pH drops below 6. In these environments, it is converted by pyrazinamidase to pyrazinoic acid, which disrupts membrane energy metabolism and fatty acid synthesis through mechanisms that are still not fully understood at the molecular level. Pyrazinamide reaches the bacterial populations hiding in these hostile niches that other drugs cannot efficiently penetrate. Its main toxicity is hepatotoxicity (the most liver-damaging of the four first-line drugs) and elevated uric acid (it blocks renal tubular secretion of urate), which can cause or worsen gout. It is used only in the initial two-month intensive phase because resistance to pyrazinamide develops if it is continued into the continuation phase without isoniazid and rifampicin both present.
Ethambutol (E)
Ethambutol is the only bacteriostatic drug in the first-line regimen — it slows bacterial growth rather than killing bacteria directly. It inhibits arabinosyltransferases (the EmbA/B/C enzymes), blocking synthesis of arabinogalactan, a polysaccharide that forms the scaffold of the mycobacterial cell wall linking mycolic acids to the underlying peptidoglycan. Its primary role in HRZE is protective: by slowing bacterial replication, it gives the other three drugs time to kill bacteria before resistant mutants can emerge and proliferate. Its most important toxicity is optic neuritis — inflammation of the optic nerve that causes blurred vision and loss of red-green color discrimination. This is dose-dependent and typically reversible if caught early, which is why monthly monitoring of visual acuity and color vision is standard while patients are on ethambutol. Doses must be reduced in renal impairment as ethambutol is renally cleared.
The 2HRZE/4HR Standard Regimen
The standard notation for TB treatment is 2HRZE/4HR. This shorthand encodes the entire regimen: the number before the letters indicates how many months those drugs are used, and the letters name the drugs. Translated: two months of all four drugs (the intensive phase), followed by four months of isoniazid and rifampicin only (the continuation phase), for a total of six months.
The two-phase structure reflects the biology of the infection. In the first two months — the intensive phase — all four drugs together kill more than 99% of the bacterial population rapidly. Sputum cultures typically convert from positive to negative within eight weeks in drug-sensitive TB. Patients become non-infectious to others within the first two to three weeks of effective treatment. The continuation phase, with just isoniazid and rifampicin, is not about killing the bulk of bacteria (that work is done). It is about eliminating the last slow-growing, semi-dormant bacterial population hiding in granulomas and caseous tissue — the bacteria that would cause relapse months or years later if allowed to survive. Without the continuation phase, relapse rates climb to 20% or higher even when sputum cultures are negative at two months.
This precise six-month structure emerged from a series of landmark British Medical Research Council trials conducted primarily in the 1970s and 1980s. Before pyrazinamide was added to first-line therapy, regimens required 12-18 months. The 1980 trials established that adding pyrazinamide during the intensive phase allowed the regimen to be shortened to six months without increased relapse, a finding that transformed global TB control. Fixed-dose combination (FDC) tablets that put all four drugs in one or two pills improve adherence and reduce the risk of patients taking only some of the drugs (which drives resistance).
Daily dosing is the preferred standard. Some older guidelines allowed three-times-weekly dosing under direct observation (DOT), but contemporary WHO guidance recommends daily dosing as it produces better outcomes. A newer four-month regimen — 2MHRZ/2MHR, substituting moxifloxacin for ethambutol — was evaluated in the TBTC Study 31/ACTG A5349 trial published in 2021 and shown to be non-inferior to the standard six-month regimen in drug-sensitive pulmonary TB. This represents the first successfully shortened regimen in 40 years, though it has not yet replaced the six-month standard everywhere.
Weight-Based Dosing
All four TB drugs are dosed by body weight. This matters because blood drug concentrations vary significantly between a 45 kg adult and a 90 kg adult if flat milligram doses are used, and inadequate drug levels are a direct driver of treatment failure and resistance development. For this reason, most guidelines provide weight-band dosing tables rather than single fixed doses.
Standard approximate adult daily doses:
- Isoniazid (H): 5 mg/kg, maximum 300 mg/day. In practice, 300 mg is used for most adults over 50 kg as a fixed dose. Higher doses (10 mg/kg) are sometimes used in patients with very high bacterial loads.
- Rifampicin (R): 10 mg/kg, maximum 600 mg/day. Most adults over 50 kg receive 600 mg. Smaller adults (below 50 kg) receive 450 mg to avoid over-exposure.
- Pyrazinamide (Z): 25 mg/kg (range 20-30 mg/kg), maximum 2 g/day. Weight bands: 40-55 kg = 1,000 mg; 56-75 kg = 1,500 mg; 76-90 kg = 2,000 mg.
- Ethambutol (E): 15-20 mg/kg, maximum 1.6 g/day. Must be reduced in renal impairment — in patients with creatinine clearance below 30 mL/min, extend dosing interval to every 48 hours or reduce dose significantly. Monitor drug levels if possible in renal failure.
Children metabolize TB drugs faster than adults and require higher mg/kg doses: isoniazid 10 mg/kg (max 300 mg), rifampicin 15 mg/kg (max 600 mg), pyrazinamide 35 mg/kg (max 2 g), ethambutol 20 mg/kg (max 1.2 g). Weight must be monitored throughout treatment because patients typically gain weight as they recover — dose adjustments should be made if weight changes significantly.
All four drugs should ideally be taken together once daily, on an empty stomach when possible (food slows and reduces absorption of rifampicin in particular). If nausea is a significant problem, taking with a small amount of food is preferable to patients taking drugs irregularly. Do not take antacids within two hours of taking TB drugs.
Monitoring Parameters During HRZE Treatment
Careful monitoring during TB treatment serves two purposes: catching drug toxicity early before it becomes serious, and verifying that the treatment is working. The following monitoring schedule reflects standard clinical guidelines.
Baseline Assessment Before Starting
Before the first dose of TB drugs, obtain: liver function tests (ALT, AST, total bilirubin, alkaline phosphatase), serum creatinine and estimated GFR, complete blood count, visual acuity test and red-green color vision (Ishihara color plates), serum uric acid, body weight, and an HIV test (if status unknown). Baseline LFTs are essential because pre-existing liver disease dramatically increases the risk of hepatotoxicity and changes the monitoring frequency required.
Ongoing Monitoring During Treatment
Monthly at every clinic visit: body weight (adjust drug doses if significant change), symptom review focusing on nausea, jaundice, visual symptoms, tingling/numbness in extremities, joint pain, and adherence assessment (count remaining pills, discuss challenges). Visual acuity and red-green color vision: monthly while on ethambutol (intensive phase); sooner if any visual complaints arise. Liver function tests: repeat at two weeks and then monthly in high-risk patients (pre-existing liver disease, heavy alcohol use, HIV, older age, malnutrition); in low-risk patients, recheck only if symptoms develop. Sputum smear and culture: at end of the intensive phase (two months) — a positive culture at month two is a prognostic marker for relapse risk; at end of treatment (six months) to confirm cure.
Warning Signs Requiring Urgent Evaluation
- Jaundice, right upper quadrant pain, unexplained fatigue, or confusion: possible hepatotoxicity — stop all TB drugs immediately and check LFTs
- Blurred vision, decreased visual acuity, loss of red-green color discrimination: possible ethambutol optic neuritis — stop ethambutol immediately, refer to ophthalmology
- Severe joint pain, especially in big toe, ankles, knees: possible gout from pyrazinamide-induced hyperuricemia — check uric acid, consider holding pyrazinamide
- Tingling, burning, or numbness in hands or feet: possible isoniazid peripheral neuropathy — ensure patient is on pyridoxine; check B6 supplementation
- Orange-red urine, tears, sweat: normal rifampicin effect — warn patients before starting, reassure that this is expected and harmless
- Skin rash: can indicate drug hypersensitivity; if severe, systemic, or accompanied by fever, hold all drugs and evaluate
Managing Hepatotoxicity — When to Hold and Rechallenge
Drug-induced liver injury (DILI) is the most serious and most common significant toxicity of the HRZE regimen, occurring in approximately 2-5% of patients on standard dosing. All three of the core drugs — isoniazid, rifampicin, and pyrazinamide — can cause liver injury, with pyrazinamide carrying the highest risk when it causes DILI. Early recognition and proper management prevents progression to liver failure.
When to Stop All TB Drugs
Stop all four TB drugs immediately if any of the following occur:
- ALT or AST rises to more than 5 times the upper limit of normal (ULN), regardless of whether symptoms are present
- ALT or AST rises to more than 3 times ULN with symptoms (nausea, vomiting, abdominal pain, jaundice, malaise)
- Any jaundice (visible yellowing of skin or whites of eyes) combined with any liver enzyme elevation
- Signs of acute liver failure: coagulopathy, encephalopathy, rapidly rising bilirubin
What to Do While Waiting for Liver Recovery
If the patient still has active, infectious TB while liver enzymes recover, a non-hepatotoxic bridge regimen is sometimes used: streptomycin (intramuscular aminoglycoside) plus ethambutol plus a fluoroquinolone (such as levofloxacin or moxifloxacin). This provides reasonable bactericidal activity without the three hepatotoxic drugs. Liver enzymes typically return to below 2 times ULN within two to four weeks after stopping the offending drugs.
Sequential Rechallenge to Identify the Culprit Drug
Once LFTs have returned to below 2 times ULN, reintroduce drugs sequentially — one at a time, three to seven days apart — to identify which drug caused the reaction:
- Start rifampicin first (least hepatotoxic of the three, most important to retain) at full dose. Monitor LFTs after three to seven days.
- If tolerated, add isoniazid at full dose. Monitor LFTs again after three to seven days.
- If both tolerated, add pyrazinamide last (most hepatotoxic). Monitor LFTs closely.
If pyrazinamide triggers the reaction: omit pyrazinamide permanently and extend the total regimen to nine months — 2HRE/7HR — to compensate for losing pyrazinamide's sterilizing activity. If isoniazid is the culprit: use a rifampicin-based regimen without isoniazid for 9-12 months (more complex, requires specialist guidance). In all cases where the standard regimen cannot be completed, drug susceptibility testing and specialist TB physician involvement are essential.
Pyridoxine and Neuropathy Prevention
Isoniazid causes peripheral neuropathy by interfering with vitamin B6 (pyridoxine) metabolism, and this complication is both predictable and almost entirely preventable with a simple, cheap supplement.
The Mechanism
Isoniazid is structurally similar to pyridoxine. It competes with pyridoxine for binding to pyridoxal kinase — the enzyme that converts pyridoxine to its active form, pyridoxal-5-phosphate (P5P). Isoniazid also directly reacts with P5P, forming an inactive hydrazone complex. The result is depletion of the active vitamin B6 needed by dozens of enzymes in nerve cells, including those producing the neurotransmitters GABA and dopamine, and those maintaining the myelin sheath of peripheral nerves. Without adequate P5P, peripheral nerves deteriorate, causing the characteristic tingling, burning, and numbness of isoniazid neuropathy — starting in the feet and moving upward.
Who Is Most at Risk
The risk is significantly higher in slow acetylators — people whose genetic makeup causes them to metabolize isoniazid more slowly, resulting in higher blood levels for longer periods. Slow acetylation is more common in certain populations including people from North Africa, the Middle East, and some European backgrounds; fast acetylation is more common in East Asian and Indigenous American populations. Without pyridoxine supplementation, neuropathy incidence at standard doses is approximately 0.2% in fast acetylators but can reach 40% in slow acetylators on prolonged treatment.
Groups Who Must Receive Pyridoxine
- HIV-positive patients (increased vulnerability due to HIV neuropathy)
- Malnutrition or food insecurity
- Diabetes mellitus
- Renal failure (B6 cleared renally; levels drop in renal disease)
- Heavy alcohol use (depletes B6)
- Pregnancy and breastfeeding (increased B6 requirements)
- Seizure disorders (B6 involved in GABA synthesis)
- Elderly patients
The standard supplemental dose is 25-50 mg of pyridoxine daily, taken alongside isoniazid. This dose fully prevents neuropathy in virtually all cases. The supplement is inexpensive, safe at these doses, and widely available. Many TB programs give pyridoxine to all patients on isoniazid regardless of risk category, because the cost of prevention is so much lower than the cost of treating established neuropathy. If neuropathy symptoms develop despite supplementation, the dose of pyridoxine can be increased to 100-200 mg/day.
Special Populations — HIV and Rifampicin Drug Interactions
HIV-TB co-infection is one of the most challenging management scenarios in infectious disease, primarily because rifampicin — the most essential drug in TB treatment — dramatically reduces the blood levels of most HIV antiretroviral drugs through potent induction of cytochrome P450 enzymes.
The Rifampicin-CYP Interaction
Rifampicin is among the most potent known inducers of CYP3A4, CYP2C9, CYP2C19, and P-glycoprotein. It upregulates these enzymes so dramatically that it can reduce plasma concentrations of co-administered drugs by 50-90%. For HIV drugs metabolized by CYP3A4, this means blood levels fall below therapeutic thresholds, rendering antiretroviral therapy effectively non-functional. This is not a minor pharmacokinetic adjustment — it is near-complete pharmacological elimination of certain drug classes.
Antiretroviral Compatibility With Rifampicin
- Protease inhibitors (lopinavir/r, atazanavir/r, darunavir/r): reduced by 75-90% by rifampicin. Even ritonavir-boosted regimens become subtherapeutic. Do NOT use protease inhibitors with rifampicin. If a protease inhibitor is needed, substitute rifabutin for rifampicin (rifabutin is a much weaker CYP inducer).
- Efavirenz (NNRTI): compatible with rifampicin, but blood levels are reduced approximately 25-30%. In patients over 60 kg, dose should be increased from 600 mg to 800 mg daily. At 600 mg, some guidelines accept the interaction as manageable for patients under 60 kg. Efavirenz remains a viable option for HIV-TB co-treatment.
- Dolutegravir (integrase inhibitor): rifampicin reduces dolutegravir levels by approximately 75%. Overcome by doubling the dose: 50 mg twice daily (instead of 50 mg once daily). This doubled-dose dolutegravir regimen with rifampicin-based TB treatment is now the preferred approach in most settings where dolutegravir is available.
- Bictegravir: NOT compatible with rifampicin — no dose adjustment has been shown to overcome the interaction.
- Rilpivirine: NOT compatible with rifampicin — levels drop to sub-therapeutic concentrations.
When to Start HIV Treatment During TB Therapy
For patients newly diagnosed with HIV when starting TB treatment, the timing of antiretroviral initiation matters:
- CD4 count below 50 cells/mm³: Start ART within two weeks of starting TB treatment. The mortality benefit of early ART outweighs the risk of immune reconstitution inflammatory syndrome (IRIS) at this level of immunosuppression.
- CD4 count 50-500 cells/mm³: Start ART within eight weeks of TB treatment initiation. Delaying to eight weeks reduces IRIS risk (which can cause dramatic worsening of TB symptoms due to immune recovery) while still improving survival significantly.
- CD4 count above 500 cells/mm³: ART can be deferred for up to eight weeks; the mortality benefit of immediate ART is smaller in this group.
Transplant Recipients
Rifampicin dramatically reduces tacrolimus levels (by approximately 80-90%) and cyclosporine levels. Patients on these immunosuppressants who develop active TB face an acute dilemma: using rifampicin may cause allograft rejection due to calcineurin inhibitor sub-therapeutic levels, while dose adjustments of 3-10 fold may be required. Rifabutin is the preferred alternative in transplant recipients when possible. Frequent therapeutic drug monitoring of tacrolimus is essential if rifampicin must be used.
TB Treatment in Pregnancy and Breastfeeding
Untreated active tuberculosis during pregnancy poses serious risks to both mother and infant: maternal morbidity and mortality, premature labor, low birth weight, congenital TB, and perinatal mortality. These risks are substantially greater than the risks from the drugs used to treat TB. The message from all major guidelines is clear: do not delay treatment in a pregnant woman with active TB.
Drug-by-Drug Safety in Pregnancy
- Isoniazid (H): Safe throughout pregnancy. Has been used for decades without evidence of fetal harm. Pyridoxine (B6) supplementation at 25-50 mg daily is mandatory in pregnancy, as pregnancy itself depletes B6.
- Rifampicin (R): Safe. Long track record of use in pregnancy without teratogenicity. One concern: rifampicin may cross the placenta in sufficient concentration to cause neonatal vitamin K deficiency and bleeding at delivery. Standard precaution is to administer vitamin K to the newborn at birth.
- Pyrazinamide (Z): Current WHO guidance supports use in pregnancy, and it is included in standard HRZE regimens for pregnant women. Some older guidelines expressed caution due to limited data, but contemporary evidence and systematic reviews support its safety, and the clinical benefit of including pyrazinamide (shorter regimen, better sterilizing activity) outweighs theoretical concerns.
- Ethambutol (E): Safe. No evidence of teratogenicity or fetal ocular toxicity at standard doses. Can be used throughout pregnancy.
Drugs to Avoid in Pregnancy
- Streptomycin and all injectable aminoglycosides (amikacin, kanamycin, capreomycin): Cause fetal ototoxicity — irreversible hearing loss in the developing infant. Absolutely contraindicated in pregnancy.
- Fluoroquinolones (levofloxacin, moxifloxacin): Generally avoided in pregnancy. Animal studies showed cartilage damage at high doses. Human data are limited but not reassuring enough to justify routine use. Used only when absolutely necessary and no alternative exists for drug-resistant TB.
Breastfeeding During TB Treatment
Breastfeeding is safe during standard HRZE treatment. All four drugs pass into breast milk in small concentrations — enough to occasionally produce mild side effects in the infant but not enough to treat TB in the infant. The nutritional and immunological benefits of breastfeeding outweigh the minimal drug exposure. However, if the mother has smear-positive pulmonary TB (actively infectious), she should be physically separated from the infant for the first two weeks of treatment until she is no longer infectious. The infant should receive six months of isoniazid preventive therapy (IPT) and then receive BCG vaccination after IPT is completed. This sequence — IPT first, BCG after — is used because BCG is a live vaccine that isoniazid would inhibit.
Managing Neonatal Risk
Infants born to mothers with active TB at the time of delivery need careful management: test for congenital TB, provide isoniazid preventive therapy for six months, and then vaccinate with BCG. The placenta partially protects against congenital TB, but congenital infection does occur when maternal bacteremia is present. Optimize maternal nutrition throughout pregnancy, as malnutrition worsens both TB disease severity and treatment outcomes.
Research Papers
- Search PubMed — Official ATS/CDC/IDSA guidelines for treatment of drug-susceptible TB; provides evidence-based recommendations for dosing, monitoring, and management of complications including DILI.
- Search PubMed — Comprehensive review of tuberculosis pathophysiology, epidemiology, and treatment principles including the rationale for the two-phase HRZE regimen structure.
- Search PubMed — TBTC Study 31/ACTG A5349 trial demonstrating non-inferiority of a 4-month moxifloxacin-containing regimen (2MHRZ/2MHR) versus the standard 6-month regimen in drug-sensitive pulmonary TB.
- Search PubMed — ATS statement on hepatotoxicity of antituberculosis therapy; defines the threshold criteria for stopping drugs and the sequential rechallenge protocol.
- Search PubMed — Authoritative primer on tuberculosis covering microbiology, immunopathology, diagnosis, and treatment including drug mechanisms and the global impact of the standard HRZE regimen.
- Search PubMed — Assessment of two shortened TB treatment regimens in HIV-negative patients, contributing to the evidence base for potential shortening of the continuation phase.
- Search PubMed — Review of advances in TB treatment covering the history of the HRZE regimen, drug mechanisms, and ongoing efforts to further shorten regimens with new drug combinations.
- Search PubMed — Latent TB infection management review that contextualizes the difference between preventive isoniazid monotherapy and curative HRZE regimens, with key pharmacological comparisons.
- Search PubMed — What we know about the mechanism of pyrazinamide's sterilizing activity and why it is essential for allowing the six-month regimen rather than longer therapy.
- Search PubMed — Seminal review of tuberculosis covering epidemiology, clinical management, the structure and rationale of the HRZE regimen, and challenges in HIV-TB co-treatment including rifampicin drug interactions.
Connections
- All Bacteria
- Mycobacterium Tuberculosis Overview
- TB Treatment & Prevention Hub
- Multidrug-Resistant TB (MDR-TB)
- TB Diagnosis: TST, IGRA, Imaging & Culture
- HIV