Klebsiella Diagnosis: Blood Cultures and Imaging
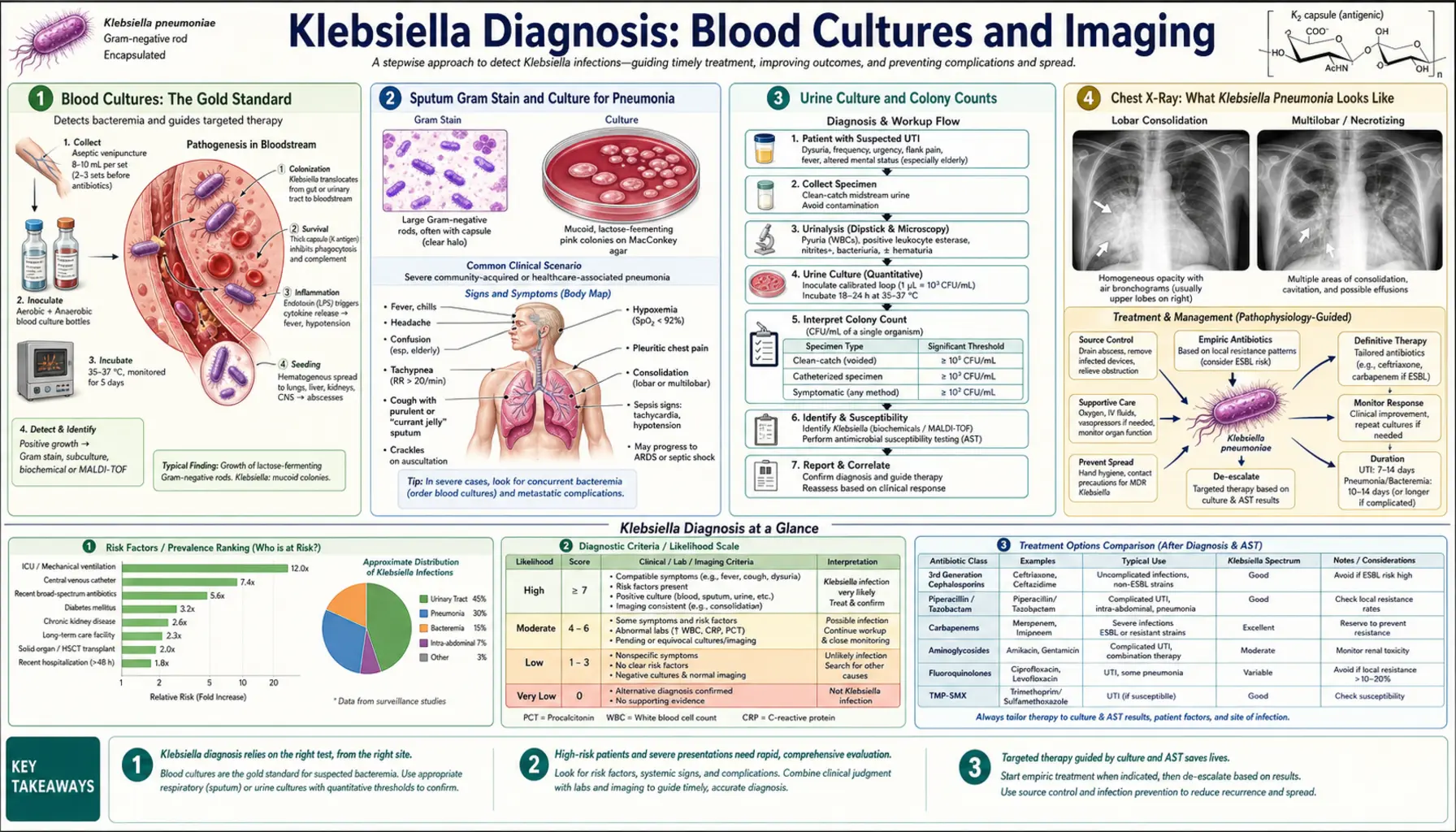
Table of Contents
- Blood Cultures: The Gold Standard
- Sputum Gram Stain and Culture
- Urine Culture and Colony Counts
- Chest X-Ray: What Klebsiella Looks Like
- CT Abdomen for Liver Abscess
- ESBL Phenotypic Screening
- Carbapenem MIC Testing and Carbapenemase ID
- Whole-Genome Sequencing for Outbreak Investigation
- Key Research Papers
- Connections
- Featured Videos
Blood Cultures: The Gold Standard
When doctors suspect a serious Klebsiella pneumoniae infection — especially one that has spread into the bloodstream — the first and most important test is a blood culture. This is considered the gold standard for diagnosing bacteremia (bacteria in the blood), which can quickly become life-threatening sepsis if not caught early.
Here is how blood cultures work in plain terms: A nurse or technician draws blood from a vein — typically two separate sets, taken from two different puncture sites on your body, usually 10 to 20 minutes apart. Each set consists of two bottles: one that grows bacteria that need oxygen (aerobic) and one that grows bacteria that thrive without it (anaerobic). Using two sites is important because it reduces the chance that any bacteria found came from a brief contamination of the skin rather than your actual bloodstream.
The blood bottles are placed in an automated incubator that monitors them continuously, usually for up to five days. If bacteria are growing, the machine detects a rise in carbon dioxide produced by the microbes and alerts lab staff, often within 24 to 48 hours for Klebsiella. At that point, technicians do a Gram stain directly from the bottle — a quick dye test that reveals the shape and staining behavior of the bacteria — and begin growing the organism on special plates so it can be identified precisely and tested against antibiotics.
Timing matters enormously. Blood cultures should be collected before antibiotics are started whenever possible. Once antibiotics are in your system, they can suppress the bacteria to the point where cultures come back falsely negative, leaving doctors without the information they need to choose the right drug. In septic shock, however, antibiotics should not be delayed more than one hour — in that scenario, cultures are drawn rapidly and antibiotics begin immediately after.
A positive blood culture for Klebsiella confirms that the infection is systemic and directs the entire treatment strategy, including which antibiotics to use and for how long.
Sputum Gram Stain and Culture for Pneumonia
When Klebsiella pneumoniae infects the lungs, the bacteria travel into the airways and mix with the fluid and debris that form sputum — the thick material you cough up from deep in your chest. Examining this sputum in the laboratory is a key step in diagnosing Klebsiella pneumonia and distinguishing it from other causes of lung infection.
The first step is a Gram stain, a rapid dye test that takes under an hour and can be done while the culture is still growing. Under the microscope, Klebsiella appears as Gram-negative rods — short, plump, rod-shaped bacteria that stain pink or red rather than purple. What makes Klebsiella particularly distinctive is its large polysaccharide capsule, a thick sugar coat that surrounds the cell and makes it look almost "fat" or encapsulated compared to other Gram-negative rods. This capsule is also a key virulence factor — it helps the bacteria evade your immune system.
The next step is plating the sputum on MacConkey agar, a selective growth medium that favors Gram-negative bacteria and suppresses Gram-positive ones. On MacConkey plates, Klebsiella produces characteristic large, mucoid (sticky, shiny) colonies because of that thick capsule. The mucoidy is visible to the naked eye and is one of the first clues that a lab technician sees before formal identification is even complete.
For sputum to be a reliable sample, it must come from deep in the chest, not just saliva from your mouth. Lab staff evaluate the quality of a sputum sample under the microscope — a good sample shows many white blood cells and few squamous (mouth) cells. Poor-quality samples are rejected and a repeat collection is requested, because an inadequate sample can produce misleading results.
Once colonies grow, the organism is identified using automated biochemical systems, and susceptibility testing determines which antibiotics will work against it.
Urine Culture and Colony Counts
Klebsiella pneumoniae is one of the most common causes of urinary tract infections (UTIs), particularly in hospitalized patients, people with urinary catheters, and those who have recently taken antibiotics. Diagnosing a Klebsiella UTI requires a urine culture — growing the bacteria from a urine sample in the lab to identify them and test antibiotic susceptibility.
The key number in a urine culture report is the colony count, expressed as colony-forming units per milliliter (CFU/mL). The traditional threshold for diagnosing a true UTI is 100,000 CFU/mL (10⁵ CFU/mL) or greater from a midstream clean-catch sample. This cutoff was established because it helps distinguish a genuine infection — where bacteria are actively multiplying in the bladder — from the small numbers of bacteria that commonly contaminate a urine sample during collection.
However, context matters. In a catheterized patient, counts as low as 1,000 CFU/mL may be clinically significant. Women with acute symptoms of a lower UTI (burning, urgency, frequency) are often treated even with counts below 100,000 if Klebsiella is the only organism identified. The lab report should always be interpreted alongside symptoms, not in isolation.
A reliable urine sample also shows pyuria — the presence of white blood cells in the urine — which is a sign that your immune system is responding to an infection. Pyuria is detected either by urinalysis (dipstick or microscopy) before the culture grows. When pyuria is absent and a high colony count is found, it may suggest colonization rather than infection, particularly in catheterized patients.
For catheter-associated specimens, the sample is collected directly from the catheter port using sterile technique, not from the drainage bag, because the bag can harbor bacteria from hours of standing urine. Proper collection technique is critical to getting a result you can trust.
Chest X-Ray: What Klebsiella Pneumonia Looks Like
When a patient arrives with fever, severe cough, and difficulty breathing, one of the first tests ordered is a chest X-ray. In Klebsiella pneumoniae pneumonia, the X-ray often shows a distinctive and alarming pattern that experienced clinicians recognize quickly.
The hallmark finding is dense lobar consolidation — a solid, white opacity filling one or more lobes of the lung. Unlike the patchy, scattered infiltrates of many other pneumonias, Klebsiella tends to fill an entire lobe completely, turning what should be an air-filled, black-looking space on X-ray into a dense, white solid. This consolidation happens because the bacteria trigger massive inflammation and fluid accumulation throughout the lobe.
A particularly distinctive sign is the bulging fissure sign: the horizontal or oblique fissures (natural boundaries between lung lobes) bow outward, away from the consolidation, because the inflammatory exudate is so voluminous that it expands the lobe beyond its normal size. This "bulging" appearance, while not unique to Klebsiella, is strongly associated with it and signals a severe, rapidly progressing infection.
Klebsiella pneumonia also has a predilection for the upper lobes, particularly the right upper lobe — a distribution more commonly seen with Klebsiella and tuberculosis than with other bacterial pneumonias, which tend to settle in lower lobes under gravity. This upper-lobe preference reflects the bacteria's ability to produce virulent infection independent of aspiration.
Chest X-ray findings in Klebsiella pneumonia can evolve rapidly — consolidation can expand over hours, and complications like lung abscesses (cavities within the lung) or empyema (pus in the pleural space around the lung) can appear. Follow-up imaging is often needed to track whether the infection is improving or worsening on treatment.
CT Abdomen for Liver Abscess
One of the most feared and increasingly recognized complications of Klebsiella pneumoniae infection is a liver abscess — a pocket of pus inside the liver. This can occur even without any obvious source of infection elsewhere in the body, a pattern called "primary" or "cryptogenic" Klebsiella liver abscess (KLA). When doctors suspect this diagnosis, a CT scan of the abdomen with intravenous contrast is the imaging test of choice.
On a contrast-enhanced CT scan, a Klebsiella liver abscess typically appears as a hypodense lesion — a dark, fluid-filled area within the liver that does not enhance (light up) with contrast the way normal liver tissue does. The surrounding rim of the abscess may enhance, creating a recognizable "ring" appearance.
Abscesses can be classified as unilocular (a single, simple cavity) or multilocular (multiple compartments divided by internal walls called septations). Multilocular abscesses are harder to drain completely with a single needle or catheter and may require more aggressive intervention or surgery. CT images provide exact measurements and mapping of the abscess that surgeons and interventional radiologists need for planning drainage procedures.
CT also evaluates for adjacent hepatic vein involvement — a dangerous complication in which the infection erodes into major veins draining the liver, allowing bacteria and clots to spread through the bloodstream. This hepatic vein thrombosis can cause further septic emboli to travel to the lungs, eyes, or brain. Identifying vascular involvement on CT changes management significantly and signals a more guarded prognosis.
MRI of the abdomen is sometimes used when CT is inconclusive or when radiation exposure is a concern, but CT remains the first-line imaging modality because it is faster, more widely available, and highly accurate for abscess detection.
ESBL Phenotypic Screening
One of the most important questions the laboratory must answer about a Klebsiella isolate is whether it produces Extended-Spectrum Beta-Lactamases (ESBLs) — enzymes that break down and inactivate a wide range of common penicillin and cephalosporin antibiotics. ESBL-producing strains are much harder to treat and limit the antibiotic options available to your doctor.
The standard method for detecting ESBLs is the double-disk diffusion test (also called the combination disk test). In this test, the laboratory places disks containing antibiotics called cephalosporins on a plate seeded with the Klebsiella isolate. Some disks contain the antibiotic alone; paired disks add clavulanate, a molecule that inhibits beta-lactamase enzymes. If the organism produces an ESBL, the zone of bacterial inhibition around the cephalosporin disk is noticeably larger when clavulanate is added — a phenomenon called "clavulanate synergy" or the "keyhole effect." The expanding zone confirms that an ESBL enzyme was being neutralized by the clavulanate, revealing its presence.
Why does this matter for treatment? ESBL-producing Klebsiella strains are resistant to most penicillins and cephalosporins — including drugs often used as first-line treatments for common infections. Using an ineffective antibiotic risks treatment failure, clinical deterioration, and the spread of resistant bacteria to other patients. When an ESBL is confirmed, doctors typically need to escalate to a different class of antibiotics, most often carbapenems, to achieve a cure.
ESBL phenotypic screening is now standard practice in most clinical microbiology laboratories whenever a Klebsiella isolate is identified from a serious infection. The result is typically reported alongside the full antibiotic susceptibility panel, giving clinicians a complete picture of their treatment options.
Carbapenem MIC Testing and Carbapenemase Identification
If a Klebsiella pneumoniae strain is resistant even to carbapenems — the antibiotics often used as the "last resort" for ESBL-producing strains — the situation becomes critically serious. Carbapenem-resistant Klebsiella pneumoniae (CRKP) infections have mortality rates exceeding 40–50% in some studies. Identifying these strains accurately and quickly is essential for patient survival and for preventing hospital outbreaks.
The first step is measuring the minimum inhibitory concentration (MIC) — the lowest concentration of a carbapenem antibiotic needed to stop bacterial growth. This is determined using automated susceptibility testing systems or manual broth microdilution. A strain with a carbapenem MIC above the clinical breakpoints established by national standards (such as CLSI or EUCAST) is flagged as resistant, triggering further investigation.
The next question is why the strain is resistant — and the answer has major implications for treatment. The most clinically important mechanism is the production of carbapenemase enzymes that directly destroy carbapenem molecules. Several rapid tests can identify carbapenemase production:
- Carba NP test: A colorimetric test performed directly on a bacterial colony. If a carbapenemase is present, it hydrolyzes (breaks down) a carbapenem substrate in the test tube, causing a color change from orange to yellow within two hours. This test is fast and inexpensive but does not identify which specific enzyme is responsible.
- Modified Carbapenem Inactivation Method (mCIM): A disk-based test in which a carbapenem disk is pre-incubated with the test organism, then placed on a plate seeded with a susceptible indicator strain. If the organism produces a carbapenemase, the enzyme degrades the antibiotic, allowing the indicator strain to grow around the disk — a visible "halo" that confirms carbapenemase activity.
- Molecular PCR testing: The most precise method, PCR (polymerase chain reaction) detects the actual genes encoding specific carbapenemases. The major types found in Klebsiella include KPC (Klebsiella pneumoniae carbapenemase, most common in the US), NDM (New Delhi metallo-beta-lactamase), and OXA-48 (common in Europe and the Middle East). Each type responds differently to available treatment agents — for example, NDM-type enzymes are not inhibited by most commercial beta-lactamase inhibitors, while KPC-type may respond to newer combination drugs like ceftazidime-avibactam.
Knowing the exact carbapenemase type allows infectious disease specialists to select the most effective salvage therapy from an increasingly limited arsenal of drugs approved for these difficult infections.
Whole-Genome Sequencing for Outbreak Investigation
When multiple patients in a hospital unit develop Klebsiella pneumoniae infections within a short time frame, infection control teams need to determine whether these are isolated cases or part of a connected outbreak — meaning the same bacterial strain is spreading from patient to patient. The gold standard tool for answering this question is whole-genome sequencing (WGS).
WGS reads the complete DNA sequence of each bacterial isolate — all several million base pairs — and compares it to isolates from other patients, environmental samples (such as sink drains or contaminated equipment), and a global database of known Klebsiella strains. Traditional typing methods like PFGE (pulsed-field gel electrophoresis) could only compare broad DNA fingerprints; WGS resolves differences down to single nucleotide changes, making it vastly more accurate for tracing transmission chains.
A key output of WGS is the sequence type (ST) — a classification system based on the allelic profiles of seven housekeeping genes (MLST, or multilocus sequence typing). The globally dominant carbapenem-resistant Klebsiella outbreak strain is ST258, which has spread across hospitals in more than 40 countries and is responsible for the majority of KPC-producing Klebsiella outbreaks in North America. Identifying ST258 immediately alerts infection control teams to heightened vigilance, since this clone is particularly adept at acquiring and transmitting resistance genes.
WGS also identifies plasmids — circular rings of DNA, separate from the main chromosome, that carry resistance genes and can transfer between bacterial cells even of different species. Tracking plasmid signatures reveals whether resistance is spreading through direct patient-to-patient transmission of a single clone, or through plasmid transfer between different bacterial strains circulating in the ward — each scenario requires different containment measures.
For patients, the practical meaning of outbreak investigation is that it can identify the source of infection (a contaminated healthcare worker's hands, a contaminated ventilator, a shared IV preparation area), lead to targeted decontamination, and ultimately prevent the next patient from being harmed. WGS has become a standard tool in tertiary-care hospital infection control programs precisely because of its power to catch and stop outbreaks before they become catastrophic.
Key Research Papers
The following peer-reviewed studies underpin current diagnostic practices for Klebsiella pneumoniae infections. Each is linked to its PubMed record for full-text access or abstract review.
-
Blood culture diagnostic standards and sepsis management
Search PubMed — Clinical practice guidelines for blood culture collection timing and volume requirements in suspected bacteremia and sepsis. -
Klebsiella liver abscess: clinical features and imaging characteristics
Search PubMed — CT imaging patterns, complication rates, and outcomes in primary pyogenic Klebsiella liver abscess with metastatic spread. -
ESBL detection: phenotypic methods and clinical implications
Search PubMed — Comparison of double-disk synergy and combination disk tests for ESBL detection in Enterobacteriaceae including Klebsiella pneumoniae. -
Carbapenemase identification: Carba NP and mCIM validation
Search PubMed — Performance evaluation of rapid carbapenemase detection tests including Carba NP and modified carbapenem inactivation method across multiple carbapenemase types (KPC, NDM, OXA-48). -
Whole-genome sequencing for hospital outbreak investigation
Search PubMed — WGS-based reconstruction of transmission chains in a carbapenem-resistant Klebsiella outbreak in an ICU setting, comparing resolution vs. traditional typing. -
ST258 global clone: genomics and resistance mechanisms
Search PubMed — Genomic epidemiology of the ST258 Klebsiella pneumoniae clone, its plasmid landscape, and intercontinental spread of KPC carbapenem resistance. -
Chest radiographic findings in Klebsiella pneumoniae pneumonia
Search PubMed — Systematic analysis of radiographic features including lobar consolidation, bulging fissure sign, and cavitation in community-acquired and hospital-acquired Klebsiella pneumonia. -
Urine culture interpretation thresholds and catheter-associated UTI
Search PubMed — Evidence review of colony count thresholds and pyuria criteria for diagnosing Klebsiella urinary tract infections including catheter-associated cases. -
Sputum Gram stain utility in Gram-negative pneumonia
Search PubMed — Prospective study of Gram stain performance for guiding early empiric therapy in hospital-acquired pneumonia caused by Klebsiella and other Gram-negative pathogens. -
Molecular PCR for carbapenemase gene detection: clinical accuracy
Search PubMed — Multicenter evaluation of multiplex PCR panels for rapid identification of KPC, NDM, OXA-48, and other clinically important carbapenemase genes in Klebsiella pneumoniae isolates.
Connections
- All Bacteria
- Klebsiella Pneumoniae Overview
- Klebsiella Symptoms Hub
- Hospital-Acquired Pneumonia and UTI
- Liver Abscess and Severe Infections
- Lab Tests
- ESBL, CRE, and Carbapenem Resistance
- Klebsiella Treatments Hub
- Pneumonia