Klebsiella Liver Abscess and Severe Infections
Most bacteria pick on the weak. Hypervirulent Klebsiella pneumoniae is different — it can strike a completely healthy 40-year-old, destroy their liver, and send pus tracking into their eye socket within days. Understanding what makes this strain so dangerous, and what to do if you think you have it, could save your sight or your life.
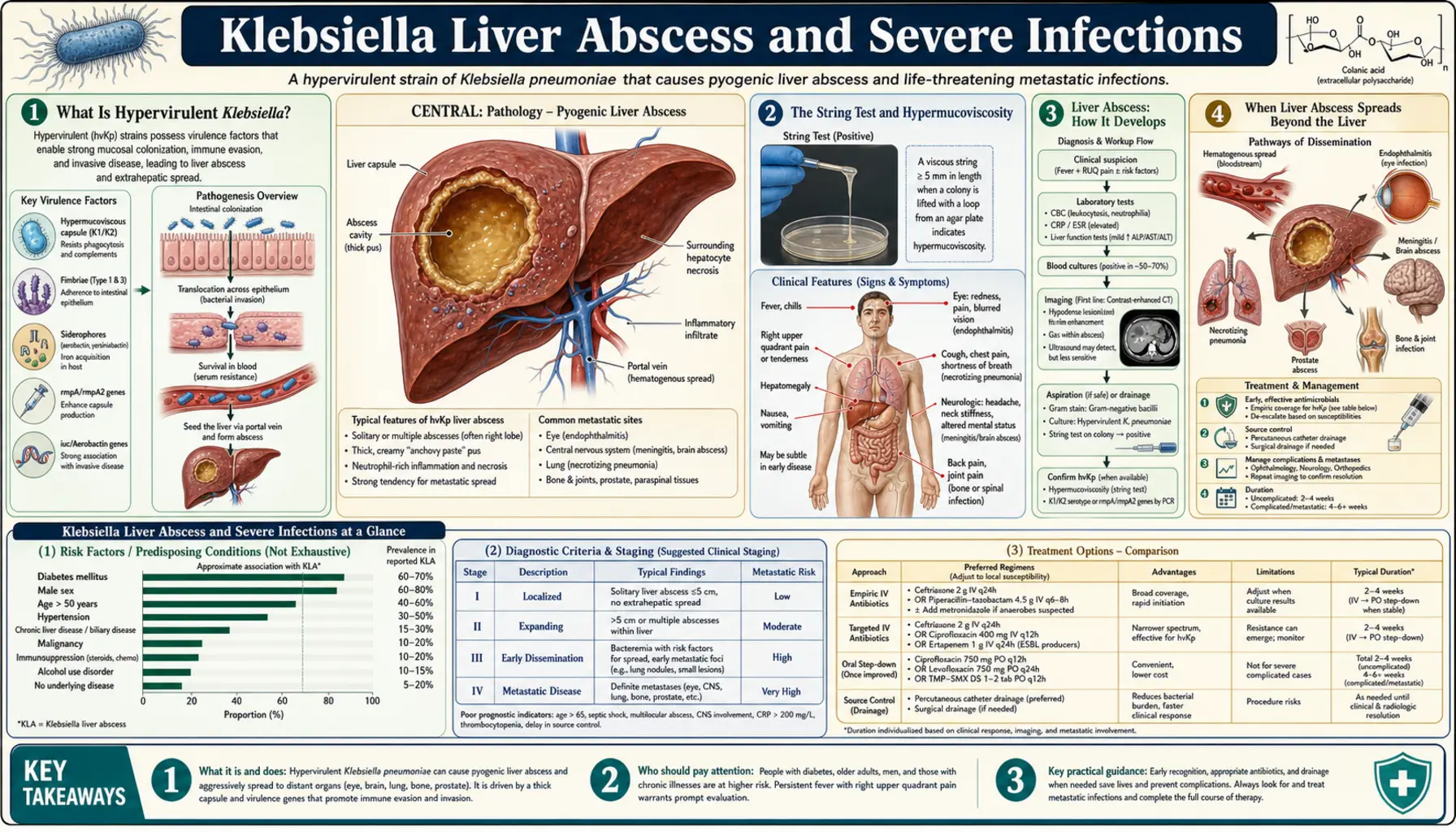
What Is Hypervirulent Klebsiella?
Klebsiella pneumoniae comes in two very different forms that look identical under a microscope but behave completely differently in a human body.
Classical Klebsiella pneumoniae (cKp) is the hospital strain most people think of — a common cause of ventilator-associated pneumonia, catheter-related urinary tract infections, and bloodstream infections in patients who are already sick, elderly, or immunocompromised. It is an opportunist. Given a healthy immune system, it rarely gets a foothold.
Hypervirulent Klebsiella pneumoniae (hvKp) is a different beast entirely. It was first described in Taiwan in the 1980s when doctors noticed otherwise healthy adults showing up with liver abscesses — a type of infection that almost exclusively affects people with liver disease or immune problems. These patients had none of those risk factors. The bacterium was killing tissue in organs that classical Klebsiella could never reach.
The key difference is that hvKp carries extra virulence genes — most of them on a mobile genetic element called a plasmid — that supercharge its ability to:
- Steal iron from the body (iron is essential for bacterial growth)
- Evade destruction by white blood cells
- Form a thick, sticky capsule that repels immune attack
- Spread from one organ to multiple organs through the bloodstream
The result is an infection that moves faster, hits harder, and can devastate previously healthy people in a matter of days.
The String Test and Hypermucoviscosity
The most distinctive feature of hypervirulent Klebsiella is its capsule — an extraordinarily thick, gel-like coating of polysaccharides that surrounds the bacterium like a force field.
This capsule is so thick and sticky that lab technicians can actually demonstrate it with a simple trick called the string test. When you touch an inoculation loop to a colony of hvKp on an agar plate and pull the loop away, the mucus stretches into a string longer than 5 millimeters — a property called hypermucoviscosity. Classical Klebsiella stays put. The string test is not perfectly specific, but it is a rapid bedside clue that the strain in front of you may be hypervirulent.
The two capsular serotypes most strongly linked to hypervirulence are K1 and K2. These polysaccharide capsule types are associated with the most serious infections, including liver abscess, endophthalmitis (eye infection), and meningitis. K1 strains account for roughly 50–70% of hvKp liver abscess cases in East Asian studies.
Behind the capsule is the gene rmpA (regulator of mucoid phenotype A), which switches on the capsule-overproduction machinery. When rmpA is present on a plasmid, it can travel between bacterial strains, potentially transforming a less dangerous bacterium into a hypervirulent one. This is one of the reasons researchers are alarmed: the traits that make hvKp dangerous are mobile and can spread.
Liver Abscess: How It Develops
The liver is the most common primary target of hypervirulent Klebsiella, and understanding why requires a brief look at how bacteria get there.
The liver receives blood from two directions: the hepatic artery (carrying oxygenated blood from the heart) and the portal vein (carrying nutrient-rich blood drained from the intestines). The portal vein means that anything living in your gut — including bacteria that briefly cross the intestinal wall — drains directly into the liver. This is called portal seeding.
In most people, the liver's immune cells (Kupffer cells) catch and destroy any bacteria arriving this way. In hvKp infection, the bacterium's thick capsule and iron-stealing machinery help it evade those defenses. The bacteria multiply inside the liver, triggering an immune response that walls off the infection into a pus-filled cavity — a liver abscess.
The role of diabetes: Diabetes is the single strongest risk factor for hvKp liver abscess. Elevated blood sugar impairs neutrophil (white blood cell) function, reduces the liver's ability to clear bacteria, and may alter gut bacteria in ways that allow Klebsiella to flourish. In Taiwan case series, diabetes is present in 50–75% of hvKp liver abscess patients. Critically, some of these patients did not know they had diabetes until their abscess brought them to the hospital.
Symptoms of Klebsiella liver abscess typically develop over days to a few weeks and include:
- Fever and chills — often the first sign, sometimes high-grade (39–40°C / 102–104°F)
- Right upper quadrant pain — dull, constant ache under the right ribs where the liver sits
- Nausea and loss of appetite
- Fatigue and general malaise
- Less commonly: jaundice (yellowing of the skin/eyes), if the abscess is large or compresses bile ducts
Blood tests typically show elevated white blood cell count, elevated C-reactive protein (CRP), and abnormal liver enzymes. CT scan of the abdomen confirms the diagnosis, showing a fluid-filled cavity in the liver.
When Liver Abscess Spreads Beyond the Liver
What makes hvKp liver abscess uniquely terrifying — and distinct from liver abscesses caused by other bacteria — is its ability to seed distant organs through the bloodstream. This is called metastatic spread, and it happens in roughly 10–15% of hvKp liver abscess cases.
Endophthalmitis: Infection Inside the Eye
The most dramatic and devastating complication is endophthalmitis — bacterial infection inside the eyeball. Bacteria travel from the liver through the bloodstream, cross the blood-eye barrier (which hvKp's capsule helps it breach), and establish an infection in the vitreous humor (the gel filling the eye). Within 24–72 hours, patients can go from blurry vision to complete, permanent blindness in the affected eye. This complication is almost unheard of with other causes of liver abscess. In hvKp patients, it can occur even before the liver abscess is diagnosed — some patients present to an ophthalmologist first.
What this means practically: Any patient with a Klebsiella liver abscess who develops sudden visual changes — floaters, decreased vision, eye pain, or redness — needs emergency ophthalmology consultation within hours. Vitrectomy (surgical removal of infected vitreous) combined with intravitreal antibiotics may save some vision if performed early.
Meningitis and Brain Abscess
Bacteria can cross the blood-brain barrier and cause bacterial meningitis (infection of the membranes surrounding the brain and spinal cord) or, less commonly, brain abscesses. Symptoms include severe headache, stiff neck, photophobia, and altered consciousness. Klebsiella meningitis carries high mortality and significant neurological sequelae in survivors.
Lung Abscess
Hematogenous (bloodborne) spread to the lungs causes pulmonary abscesses — pockets of pus in the lung tissue. Patients develop productive cough, chest pain, and worsening shortness of breath. On chest CT, these appear as cavitating lesions with air-fluid levels.
Necrotizing Fasciitis
In rare cases, hvKp causes necrotizing fasciitis — a rapidly spreading infection that destroys the soft tissue beneath the skin. This is a surgical emergency requiring immediate debridement (removal of dead tissue). It is associated with extremely high mortality when diagnosis is delayed.
Septic Shock
Bacteria entering the bloodstream in large numbers trigger the systemic inflammatory response known as sepsis, which can progress to septic shock — dangerously low blood pressure, organ failure, and death. Klebsiella bloodstream infections carry mortality rates of 20–40% in hospitalized patients, higher in those with multi-organ involvement.
Who Gets Hypervirulent Klebsiella?
The epidemiology of hvKp liver abscess has shifted significantly since it was first described, and understanding who is at risk may save lives.
The East Asian Origin and Global Spread
hvKp liver abscess was first recognized as a distinct clinical syndrome in Taiwan in the 1980s and was initially considered a regional disease. Subsequent decades brought reports from South Korea, China, Singapore, and other East Asian countries, where it became a major cause of community-acquired liver abscess in otherwise healthy adults. For years, Western physicians rarely saw it.
That changed. Since the 2000s, hvKp liver abscess has been reported in North America, Europe, Australia, and Africa — in patients who had never traveled to Asia. The syndrome is now genuinely global.
Diabetes Is the Dominant Risk Factor
Across all populations studied, diabetes mellitus (especially type 2 diabetes) is present in the majority of hvKp liver abscess patients. The risk is so strong that some infectious disease specialists recommend testing blood sugar in every patient admitted with a liver abscess — some discover their diabetes at the same admission.
Healthy People Are Not Immune
Unlike classical Klebsiella, which almost exclusively attacks immunocompromised hosts, hvKp can infect immunocompetent individuals with no chronic illness. This is the defining feature that makes it clinically distinct. A healthy 35-year-old athlete without diabetes can develop a Klebsiella liver abscess from hvKp. The thick capsule is simply too much for a normal immune response to handle.
Other Contributing Factors
- Heavy alcohol use — impairs liver immune defenses
- Biliary tract abnormalities — gallstones, bile duct strictures
- Recent abdominal procedures — endoscopy, surgery
- Corticosteroid use — suppresses immune response
- Iron overload conditions — hemochromatosis (iron fuels bacterial growth)
The Virulence Plasmid: Why hvKp Is So Dangerous
The extraordinary danger of hypervirulent Klebsiella comes from a collection of genes, many of them carried on a mobile genetic element called the virulence plasmid (commonly called pLVPK or similar designations). Think of a plasmid as a bonus chromosome — a small circular piece of DNA that carries extra instructions and can be copied and passed between bacteria.
rmpA — The Capsule Amplifier
The gene rmpA (regulator of mucoid phenotype A) massively upregulates production of the polysaccharide capsule. More capsule means better evasion of neutrophils and complement (the immune system's molecular attack proteins). rmpA is the molecular switch that turns a normal-looking Klebsiella into the hypermucoviscous phenotype you can demonstrate with the string test.
Aerobactin — Stealing Iron
Bacteria need iron to grow, but the human body keeps most of its iron tightly bound to proteins (transferrin, lactoferrin) to starve pathogens. hvKp produces aerobactin, a high-affinity iron-scavenging molecule (called a siderophore) that outcompetes the body's iron-binding proteins. Aerobactin lets hvKp grow rapidly in tissues where classical Klebsiella cannot, because it can steal iron more efficiently. This is one reason hvKp thrives in iron-rich environments like the liver.
Salmochelin — A Second Iron Weapon
Salmochelin is a second siderophore, originally described in Salmonella but also found in hvKp. It has a critical advantage: it is modified to resist being sequestered by a human immune defense protein called lipocalin-2. Classical Klebsiella strains typically lack salmochelin. With two iron-stealing systems — aerobactin AND salmochelin — hvKp can sustain rapid growth even when the immune system is actively trying to starve it.
Colibactin — A Genotoxin
Some hvKp strains also carry the colibactin gene cluster (the pks island). Colibactin is a genotoxin — it damages the DNA of human cells, causing double-strand breaks. This may promote inflammation and tissue destruction and has been linked to an increased risk of colorectal cancer in strains that carry it chronically in the gut. In acute hvKp infections, colibactin likely contributes to tissue damage and may help the bacterium evade cell-based immunity.
Together, these virulence factors explain why hvKp can infect healthy tissue, multiply faster than the immune system can respond, spread through the bloodstream, and damage organs in ways that classical Klebsiella never could.
Convergent Resistance: When hvKp Meets Drug Resistance
For most of hvKp's history, there was one piece of moderately good news: hypervirulent strains were generally susceptible to antibiotics. Unlike classical Klebsiella, which has been acquiring multi-drug resistance genes for decades, hvKp strains were typically treatable with standard antibiotics. That is changing.
The Emerging Nightmare: CR-hvKp
Starting around 2016, reports emerged — primarily from China — of Klebsiella strains that carried both the hypervirulence plasmid and carbapenem-resistance genes (particularly KPC, NDM, and OXA-type carbapenemases). These convergent strains (CR-hvKp) combine the worst features of both worlds:
- The ability to infect healthy people outside hospitals (from hvKp)
- Resistance to nearly all antibiotics, including last-resort carbapenems (from drug-resistant cKp)
There are now documented cases of CR-hvKp in China, the United States, Italy, and other countries. Mortality in these infections is extremely high — some series report 40–60% case fatality rates — because there are very few effective antibiotics left to use.
How Convergence Happens
Because both the virulence genes and resistance genes are carried on mobile plasmids, they can come together in a single bacterium through horizontal gene transfer — essentially bacteria swapping genetic material. A drug-resistant classical Klebsiella can acquire the hvKp virulence plasmid, or vice versa. Once this happens, the resulting strain is extremely difficult to treat and highly dangerous even to healthy individuals.
Why Global Surveillance Matters
Public health agencies and infectious disease researchers are tracking CR-hvKp as a high-priority emerging pathogen. Early detection — through whole-genome sequencing of isolates — is critical for containing outbreaks. If you are treated for a Klebsiella infection, your care team should send isolates for resistance testing. This data feeds into national and global surveillance systems that track whether CR-hvKp is spreading in your region.
What to Do If You Suspect Klebsiella Liver Abscess
Klebsiella liver abscess is a medical emergency. Early treatment dramatically reduces the risk of metastatic complications like endophthalmitis and meningitis. Here is what you need to know.
Go to the Emergency Room — Do Not Wait
If you or someone you know has fever with right upper quadrant abdominal pain, especially in the setting of diabetes, go to the emergency department immediately. Do not take acetaminophen or ibuprofen and hope the fever breaks on its own. Do not wait for a primary care appointment. This infection can progress from a contained liver abscess to a blinding eye infection within 48 hours.
What to Tell the ER Doctor
The more information you give, the faster the diagnosis. Tell the doctor:
- You have fever and pain in your upper right abdomen
- Whether you have diabetes (or any blood sugar abnormalities you have noticed)
- Whether you have traveled to or have family connections to East Asia
- Any visual changes — even subtle blurriness or floaters
- Any recent dental procedures, abdominal surgery, or colonoscopy
- Any recent antibiotic use (important for resistance testing)
Ask specifically: "Could this be a liver abscess? Should I have a CT scan of my abdomen with contrast?" CT scan is the gold standard for diagnosing liver abscess.
Treatment: Drainage and Antibiotics
Standard treatment combines percutaneous needle drainage (a radiologist inserts a needle through the skin into the abscess cavity under CT or ultrasound guidance to drain the pus) with intravenous antibiotics. Treatment typically lasts 4–6 weeks. Most patients respond well when treatment begins early.
Large abscesses or those that do not respond to needle drainage may require surgical drainage. Your team will also culture the drained pus to identify the specific Klebsiella strain and test its antibiotic sensitivities — this is critical for choosing the right antibiotic.
Monitor Your Eyes Throughout Treatment
Report any visual changes immediately to your care team, even after you are in the hospital on antibiotics. Endophthalmitis can occur or worsen even after treatment begins. Some infectious disease specialists recommend routine ophthalmology evaluation for all patients hospitalized with hvKp liver abscess.
Blood Sugar Control During Recovery
If you have diabetes, tight blood sugar control during and after your hospitalization improves immune function and reduces the risk of complications and relapse. Work with your endocrinologist to optimize your regimen.
Key Research Papers
The following peer-reviewed studies form the core evidence base for hypervirulent Klebsiella pneumoniae and liver abscess syndrome.
-
Pneumonia-associated liver abscess and the hypervirulent phenotype — foundational case series establishing the clinical syndrome and K1 serotype dominance.
Search PubMed -
Global emergence of hypervirulent Klebsiella pneumoniae — systematic review documenting spread beyond East Asia to Western countries and the role of virulence plasmids.
Search PubMed -
Hypervirulent Klebsiella and convergent antimicrobial resistance — landmark study documenting the emergence of CR-hvKp strains combining hypervirulence and carbapenem resistance.
Search PubMed -
The rmpA gene and hypermucoviscosity — molecular characterization of rmpA as the key regulator of the hypermucoviscous phenotype and its role in tissue invasion.
Search PubMed -
Aerobactin and salmochelin siderophores in hvKp virulence — mechanistic study of iron acquisition systems enabling growth in iron-restricted host environments.
Search PubMed -
Endophthalmitis complicating Klebsiella liver abscess — clinical series documenting the frequency, timing, and outcomes of eye involvement in hvKp liver abscess.
Search PubMed -
Colibactin genotoxin in hvKp strains — identification of the pks genomic island in hypervirulent isolates and implications for tissue damage and oncogenicity.
Search PubMed -
Diabetes mellitus as the dominant risk factor for hvKp liver abscess — meta-analysis quantifying the association between diabetes and primary pyogenic liver abscess caused by Klebsiella.
Search PubMed -
Capsular serotype K1 and metastatic infection — prospective cohort study linking K1 capsular type to higher rates of metastatic complications including meningitis and endophthalmitis.
Search PubMed -
Percutaneous drainage outcomes in Klebsiella liver abscess — largest published series on percutaneous versus surgical drainage approaches and predictors of clinical failure.
Search PubMed
Connections
- All Bacteria
- Klebsiella Pneumoniae — Overview
- Klebsiella Symptoms Hub
- Hospital-Acquired Pneumonia and UTI
- Diagnosis: Blood Cultures and Imaging
- Sepsis
- Diabetes
- Klebsiella Treatments Hub
- Meningitis