Klebsiella Drug Resistance: ESBL, CRE, and Carbapenem Resistance
Drug resistance in Klebsiella pneumoniae is one of the most urgent public health crises of the 21st century. This bacteria has developed the ability to destroy almost every class of antibiotic doctors have — including carbapenems, which were once considered the last reliable option. Understanding what these resistance mechanisms are, how they spread, and what limited treatment options remain is critical for patients, families, and anyone who might face a hospital stay. This article breaks down the science in plain language so you can understand what you or a loved one may be up against.
- What Are ESBLs?
- How Carbapenem Resistance Develops
- Last-Resort Antibiotics for CRE
- Polymyxins: Colistin and Polymyxin B
- Combination Therapy for CRE
- How Drug Resistance Spreads
- CRE as a WHO Critical Priority Pathogen
- Phage Therapy and Future Treatments
- Key Research Papers
- Connections
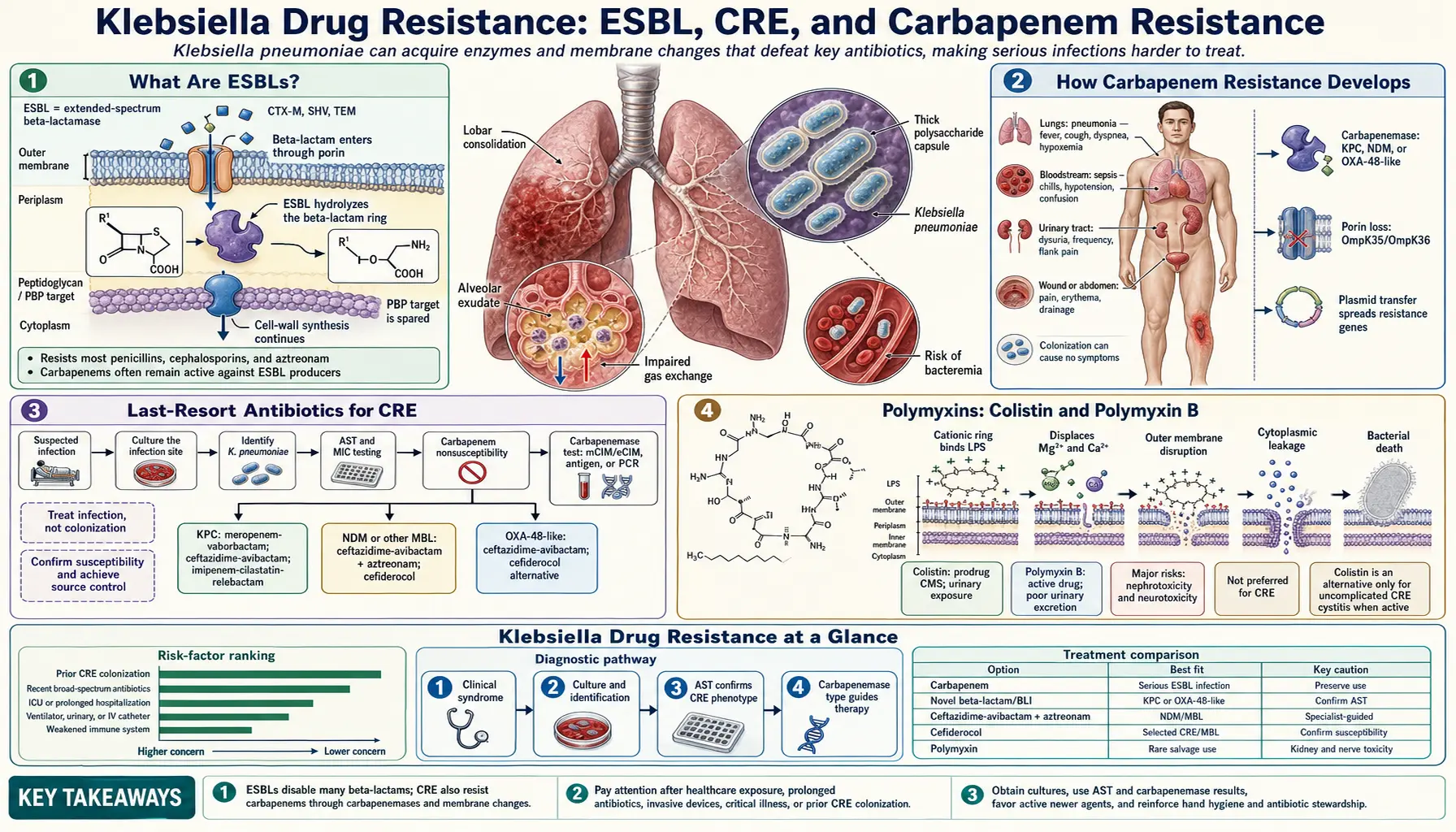
What Are ESBLs?
ESBL stands for Extended-Spectrum Beta-Lactamase. To understand what that means, you need to know one thing: most common antibiotics — penicillins, cephalosporins, and related drugs — work by attacking a specific part of a bacterial cell wall. They all belong to a family called beta-lactam antibiotics, named after a chemical ring structure at their core.
Bacteria like Klebsiella pneumoniae have learned to make enzymes — biological scissors — that cut open that ring structure and render the antibiotic harmless. These enzymes are called beta-lactamases. Old-generation beta-lactamases could only destroy a narrow range of antibiotics. Extended-spectrum beta-lactamases (ESBLs), by contrast, can destroy a much wider range, including most penicillins and nearly all oral and injectable cephalosporins.
The three most clinically important ESBL families in Klebsiella are:
- CTX-M enzymes — now the dominant ESBL type worldwide, named for their ability to destroy the antibiotic cefotaxime. CTX-M-15 is the single most common variant globally and has spread explosively since the early 2000s.
- SHV enzymes — the original "natural" beta-lactamase of K. pneumoniae, which mutated over time to gain extended-spectrum activity. SHV-2 and SHV-12 are common hospital isolates.
- TEM enzymes — originally identified in E. coli, TEM-family ESBLs crossed into Klebsiella via horizontal gene transfer and now circulate widely in hospital settings.
What makes ESBLs especially dangerous is how they spread. These enzymes are not encoded in the bacterium's main chromosome — they live on plasmids, which are small, independent rings of DNA that bacteria can share with each other like passing a note. One bacterium carrying an ESBL plasmid can transfer it to dozens of neighboring bacteria in hours, including different species entirely. A patient with an ESBL-producing Klebsiella infection who also carries E. coli in their gut may end up with ESBL-resistant E. coli as well — a double problem.
When a lab report says a patient's Klebsiella is "ESBL-positive," it means standard oral antibiotics are almost certainly useless, and even many IV cephalosporins cannot be trusted even if they appear susceptible on the lab printout (a well-documented phenomenon called inoculum effect). Treatment typically requires carbapenems — at least until those stop working too.
How Carbapenem Resistance Develops
Carbapenems (drugs like meropenem, imipenem, and ertapenem) were once the gold standard for treating serious ESBL infections. They belong to the beta-lactam family but have a modified ring structure that older enzymes cannot cut. For years, they were considered essentially untouchable by bacterial resistance. That era is over.
Carbapenem-Resistant Enterobacterales (CRE) is the clinical term for bacteria of the Enterobacteriaceae family — which includes Klebsiella — that have developed resistance to carbapenems. When CRE affects Klebsiella pneumoniae specifically, it is called CRKP (Carbapenem-Resistant Klebsiella pneumoniae).
Three main enzyme families drive carbapenem resistance:
KPC — Klebsiella pneumoniae Carbapenemase
KPC was first identified in a clinical isolate from North Carolina in 1996 and published in 2001. It belongs to a class called serine carbapenemases — the enzyme uses a serine amino acid at its active site to chemically hydrolyze (break apart) the carbapenem ring. KPC rapidly spread across the United States, then globally. By 2010 it had reached over 40 countries. The ST258 clone of K. pneumoniae carrying KPC became one of the most successful hospital pathogens ever identified. Today, KPC is the predominant carbapenem resistance mechanism in the U.S., much of Europe, and South America. Critically, KPC can be inhibited by certain new drugs (avibactam, vaborbactam), which is why those newer antibiotics have clinical value.
NDM-1 — New Delhi Metallo-Beta-Lactamase
NDM-1 was first described in 2008 in a Swedish patient who had been hospitalized in New Delhi, India — hence the name. Unlike KPC, NDM belongs to the metallo-beta-lactamase class: instead of serine, it uses a zinc ion to destroy carbapenem molecules. This matters enormously for treatment because metallo-beta-lactamases are not inhibited by avibactam or vaborbactam. NDM has spread across South Asia, Africa, the Middle East, and is increasingly found worldwide. It can also destroy aztreonam, which is one reason treating NDM infections is so difficult.
OXA-48
OXA-48 is an oxacillinase-type carbapenemase common in Turkey, North Africa, the Middle East, and now increasingly in Southern Europe. OXA-48 hydrolyzes carbapenems relatively slowly compared to KPC or NDM — sometimes strains appear borderline susceptible or intermediate — but clinical failures still occur. OXA-48 is also not inhibited by avibactam alone, though the combination of aztreonam plus avibactam is active against it. Many OXA-48 producers co-carry ESBL genes, making them resistant to virtually all beta-lactam antibiotics.
These three enzyme types work by completely different chemical mechanisms, which is why no single antibiotic or combination works universally against all CRE — the doctor and the lab must identify which type of resistance is present before choosing treatment.
Last-Resort Antibiotics for CRE
When a patient has CRKP, treating physicians face a grim calculus: the standard antibiotic toolkit is empty. The drugs below represent the current last-resort options, each with important limitations based on which type of carbapenemase the bacteria carries.
Ceftazidime-Avibactam (Avycaz)
Approved in 2015, this drug pairs an older cephalosporin (ceftazidime) with a new non-beta-lactam beta-lactamase inhibitor (avibactam). Avibactam blocks KPC and OXA-48-type enzymes, restoring the ceftazidime's killing power. In clinical trials and real-world data, it significantly outperformed colistin-based regimens for KPC-producing Klebsiella infections, with lower mortality and far less kidney damage. Critical limitation: avibactam does not inhibit metallo-beta-lactamases like NDM-1. Using it against NDM strains invites rapid resistance development.
Meropenem-Vaborbactam (Vabomere)
Approved in 2017, this combines meropenem with vaborbactam, a boronic acid inhibitor with potent activity against KPC. Clinical data show excellent efficacy against KPC-producing CRE. Like ceftazidime-avibactam, it has no activity against NDM or OXA-48. It is generally used as an alternative to ceftazidime-avibactam when KPC is confirmed and the patient has had prior exposure or resistance emergence on the other agent.
Cefiderocol (Fetroja)
Cefiderocol is a structurally unique drug approved in 2019. It is a siderophore cephalosporin — it disguises itself as iron, which bacteria actively import. Once inside the bacterial cell, it attacks penicillin-binding proteins. This Trojan-horse mechanism allows it to evade most known resistance enzymes, including NDM, KPC, OXA-48, and even some porin-loss mechanisms. Clinical trial data suggest activity against NDM-producing strains when other options have failed. However, resistance can emerge during therapy, and clinical outcome data remain more limited than for ceftazidime-avibactam. In the CREDIBLE-CR trial, cefiderocol showed non-inferior mortality against best available therapy for CRE, though a higher all-cause mortality signal in a subset of patients requires careful consideration.
Aztreonam-Avibactam
This combination is not yet FDA-approved as a fixed formulation in the United States as of 2024 (aztreonam plus separately administered avibactam or ceftazidime-avibactam is used off-label). It is specifically important for NDM-1 infections: aztreonam is the only beta-lactam that metallo-beta-lactamases cannot destroy, but many NDM strains also carry ESBL enzymes that destroy aztreonam — avibactam blocks those ESBLs, allowing aztreonam to work. This aztreonam-avibactam combination has become the recommended approach for serious infections caused by NDM-producing Klebsiella in expert guidelines.
The key takeaway for patients: treatment of CRE is not a simple prescription. It requires knowing exactly which resistance gene the bacteria carries, which lab a specialized reference laboratory must identify. This is why sending cultures from critically ill patients to reference labs and saving isolates is important.
Polymyxins: Colistin and Polymyxin B
Before the newer agents above were available, and still in settings where they are unavailable or unaffordable, physicians turned to an antibiotic class from the 1940s and 1950s: the polymyxins. These include colistin (also called polymyxin E) and polymyxin B.
How Polymyxins Work
Polymyxins work on a completely different principle from beta-lactams. Instead of attacking the cell wall, they act like a detergent on the outer membrane of gram-negative bacteria. They insert into the bacterial membrane, disrupt its structure, and cause the cell to leak and die. Because this mechanism does not involve the beta-lactam ring at all, ESBL and carbapenemase enzymes cannot inactivate them. This is why polymyxins remained active against bacteria that had become resistant to every other antibiotic class.
The Problem: Severe Kidney Toxicity
Polymyxins were largely abandoned in the 1970s precisely because of their toxicity. Kidney damage (nephrotoxicity) occurs in 20 to 60% of patients receiving colistin at therapeutic doses. The exact rate depends on the patient's baseline kidney function, dose, duration, and concomitant medications. This toxicity is dose-dependent and sometimes irreversible. Patients with already-compromised kidneys — common in ICU patients with CRKP — are at highest risk. Dosing colistin correctly is also notoriously difficult, requiring specialized pharmacokinetic calculations because the drug is given as an inactive prodrug (colistimethate sodium) that converts to active colistin in the bloodstream at variable rates.
Polymyxin B has a somewhat more predictable pharmacokinetic profile and may cause slightly less nephrotoxicity than colistin in comparative studies, though both carry serious risk.
The mcr-1 Resistance Gene
In 2015, Chinese researchers reported the mcr-1 gene — a colistin resistance gene carried on a mobile plasmid, found in bacteria from food animals and humans in China. The mcr-1 gene modifies the bacterial outer membrane so polymyxins can no longer insert properly. Strains carrying both mcr-1 and KPC or NDM are essentially resistant to all available antibiotics. While mcr-1 has not yet spread at epidemic scale in most hospital settings, its presence in food animals and its transferability via plasmids make it a concerning surveillance target. Detection of colistin resistance in a CRKP isolate should prompt immediate reference laboratory testing to identify mcr genes.
Combination Therapy for CRE: Why Two Antibiotics Are Better Than One
Treating serious CRKP infections with a single antibiotic — even a novel one — is often insufficient. Infectious disease specialists frequently use two or more agents simultaneously, a strategy called combination therapy. There are solid scientific reasons for this approach.
The Synergy Rationale
When two antibiotics attack the same bacterial cell through different mechanisms simultaneously, their combined effect can be greater than the sum of their individual effects — this is called synergy. For example, when a polymyxin disrupts the outer membrane, it can actually allow other antibiotics that would otherwise be blocked to penetrate into the bacterial cell. This is why colistin plus rifampin, or colistin plus a carbapenem (even in resistant strains), sometimes shows activity in laboratory tests and some clinical scenarios even when each drug alone appears inactive.
Ceftazidime-Avibactam Plus Aztreonam for NDM Strains
For NDM-producing strains, the combination of ceftazidime-avibactam plus aztreonam has become a critically important strategy. Here is the logic: NDM destroys carbapenems and ceftazidime but cannot touch aztreonam. However, most NDM strains also carry ESBLs that can destroy aztreonam. Avibactam (in the ceftazidime-avibactam formulation) blocks the ESBLs that would otherwise destroy aztreonam. So avibactam protects aztreonam, and aztreonam kills the bacteria — even though ceftazidime itself may be hydrolyzed by NDM. This kind of "chessboard" combination rationale represents the frontier of CRE treatment strategy.
Double Carbapenem Therapy
For certain KPC-producing strains, an experimental approach called double carbapenem therapy (typically ertapenem plus meropenem) has been reported in case series and small studies, particularly from Italy and other settings before newer beta-lactamase inhibitors were available. The rationale is that ertapenem "soaks up" KPC enzyme and is preferentially hydrolyzed, allowing meropenem to exert some antibacterial effect. This approach is now largely replaced by ceftazidime-avibactam where available, but it remains a consideration in resource-limited settings. Clinical evidence quality is low — it should only be used when nothing else is available.
What This Means for Patients
If a family member is in an ICU with CRKP and the doctor proposes using two or three antibiotics simultaneously, this reflects the complexity of the infection rather than medical uncertainty or error. Ask the treating team: "Do you know which carbapenemase gene this bacteria has?" That single piece of information dramatically changes which combination makes sense.
How Drug Resistance Spreads: Plasmids and Horizontal Gene Transfer
To understand why drug resistance in Klebsiella has spread so explosively — from a single North Carolina hospital in 1996 to a global pandemic of CRE within 20 years — you need to understand a biological process called horizontal gene transfer.
What Horizontal Gene Transfer Means
Normally when we think of genes being passed on, we think of parents to children — vertical transfer through reproduction. Bacteria can do that too, but they have an additional trick: they can share genetic material sideways between bacteria that are completely unrelated, even between different species. This is horizontal gene transfer.
The most important vehicle for this in Klebsiella is the plasmid — a small, circular piece of DNA separate from the main bacterial chromosome. Resistance genes like KPC, NDM, and CTX-M all commonly reside on plasmids. When two bacteria come into physical contact, one can transfer a copy of its plasmid to the other through a bridge-like structure called a pilus — a process called conjugation. This can happen within minutes. A KPC-positive Klebsiella sitting in a patient's gut next to non-resistant E. coli or other bacteria can share its resistance plasmid with those neighbors, suddenly making them resistant too.
Mobile Genetic Elements
The resistance genes themselves are often embedded in transposons and integrons — mobile genetic elements that can jump between different plasmids and even between plasmids and chromosomes. This is why the same KPC gene can appear in dozens of different bacterial species across multiple continents: the gene itself is mobile within mobile elements on mobile plasmids. It is resistance that travels.
The Global ST258 Clone
Beyond gene transfer, one specific lineage of Klebsiella pneumoniae has been especially successful at spreading: Sequence Type 258 (ST258). This is a clone — a single ancestral bacterial strain that has replicated and spread globally. ST258 carries KPC on a particularly stable, transferable plasmid and has a surface structure that appears to help it evade the immune system and persist in hospital environments. Studies using whole-genome sequencing have traced the international spread of ST258 from the United States to Europe, Israel, South America, and beyond. When clinicians in different countries speak of a "CRE outbreak," they are often dealing with the same clone arriving via patients transferred internationally or via international travelers.
CRE as a WHO Critical Priority Pathogen
In 2017, the World Health Organization published its first-ever list of antibiotic-resistant bacteria for which new treatments are most urgently needed. Carbapenem-resistant Klebsiella pneumoniae was placed in Priority 1: CRITICAL — the highest category — alongside carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa. This was not a bureaucratic designation; it reflected mortality data that alarmed researchers worldwide.
Mortality Data
CRKP bacteremia (bacteria in the bloodstream) carries a mortality rate of 40 to 70% in published clinical series, depending on the severity of illness, timing of appropriate treatment, and whether any active antibiotic options remain. Even with optimal treatment using the best available agents, mortality regularly exceeds 30%. By comparison, bloodstream infections with antibiotic-susceptible Klebsiella have mortality around 15-20% — still serious, but dramatically better. The mortality gap between susceptible and resistant infection directly measures the cost of resistance in human lives.
Global Surveillance Data
The ECDC (European Centre for Disease Prevention and Control) tracks CRE across European countries. As of recent surveillance reports, carbapenem resistance rates in Klebsiella bloodstream isolates range from under 1% in Nordic countries (Netherlands, Sweden, Denmark) to over 60% in Greece and over 30% in Italy, Romania, and Bulgaria. In South Asia — particularly India, Pakistan, and Bangladesh — NDM prevalence in hospital-acquired infections is extremely high, with rates in some centers exceeding 70%. The United States CDC tracks CRE nationally through the Antibiotic Resistance Patient Safety Atlas; rates in U.S. hospitals vary by region and institution but have generally been rising, with healthcare-associated CRE now endemic in many urban medical centers.
The Economic Burden
Beyond mortality, CRKP infections cause dramatically prolonged hospital stays — 20 to 40 additional days compared to susceptible infections in matched studies — along with the costs of isolation precautions, extended ICU care, and consultations. A single patient with CRKP bacteremia may generate $100,000 or more in additional hospital costs. For families, this often means weeks of anxiety, delayed recovery, and in many cases loss of a family member to an infection that would have been treatable a generation ago.
Phage Therapy and Future Treatments
When no antibiotic works, researchers are turning to solutions that predate antibiotics themselves. The science of what comes next for CRKP is genuinely exciting, though most options remain years from routine clinical use.
Bacteriophage Therapy
Bacteriophages (phages for short) are viruses that infect and kill bacteria. They have been used in Eastern Europe — particularly Georgia and Poland — for decades, but were largely abandoned in the West when antibiotics arrived. With CRE making antibiotics obsolete, phage therapy is experiencing a serious scientific revival. Phages can be engineered or selected to target specific bacterial strains; some have anti-biofilm activity that antibiotics lack. Case reports of compassionate-use phage therapy for otherwise-untreatable CRKP infections have appeared in peer-reviewed literature, including cases where patients in extremis recovered after phage infusion. A 2017 case at UC San Diego — a professor cured of multidrug-resistant Acinetobacter bacteremia using phage — drew worldwide attention. Clinical trials of phage therapy for CRE are now underway in multiple countries. Challenges include the narrow host range of individual phages (you need the right phage for the specific bacterial strain), the regulatory pathway for biologic treatments that evolve, and the need for rapid phage banks or on-demand manufacturing.
Novel Siderophore-Antibiotic Conjugates
Cefiderocol's success as a siderophore-conjugate has inspired research into other molecules that use the same Trojan-horse iron-uptake strategy to penetrate resistant bacteria. Several research groups and biotechnology companies are developing next-generation siderophore conjugates paired with antibiotic payloads different from cephalosporins, with the goal of hitting bacteria that have developed resistance to cefiderocol itself.
Vaccine Research
Klebsiella pneumoniae vaccines remain in relatively early development compared to vaccines for organisms like Streptococcus pneumoniae. The main challenge is the enormous diversity of Klebsiella capsular types — more than 130 distinct K-types — which makes a broadly protective vaccine difficult to design. Several companies are pursuing protein-based or conjugate vaccines targeting conserved surface antigens (rather than capsule) that might offer broader protection across strains. If successful, vaccines would be most valuable for preventing hospital-acquired CRKP in high-risk patients (the immunocompromised, patients with prolonged ICU stays, transplant recipients).
What Patients and Families Should Know
If a family member is diagnosed with an untreatable CRKP infection and conventional antibiotics have failed, it is reasonable to ask the treating team about compassionate use options. Academic medical centers with active infectious disease research programs — particularly those affiliated with phage therapy research programs (UC San Diego, Yale, NIH's Clinical Center, several European centers) — may have access to expanded options not available at community hospitals. The NIH ClinicalTrials.gov registry lists ongoing trials for CRE treatments and can be searched for eligibility. Being an informed advocate is not being difficult — it is often the only way to access emerging options in time.
Key Research Papers
The following peer-reviewed publications underpin the information in this article. All are indexed in PubMed, the U.S. National Library of Medicine's database of biomedical literature.
-
Zhanel et al. (2018) — Ceftazidime-Avibactam for CRE
A comprehensive review of ceftazidime-avibactam's mechanism, spectrum, clinical trial results, and resistance emergence in KPC-producing Enterobacteriaceae.
Search PubMed -
Tumbarello et al. (2016) — Mortality of KPC-Producing Klebsiella
A landmark multicenter Italian study examining risk factors for mortality in patients with KPC-producing Klebsiella pneumoniae bloodstream infections, with outcomes stratified by treatment regimen.
Search PubMed -
van Duin & Doi (2017) — Global Epidemiology of CRE
An authoritative review of the global spread of carbapenem-resistant Enterobacteriaceae, covering surveillance data, molecular epidemiology, and the ST258 clone.
Search PubMed -
Shields et al. (2020) — Ceftazidime-Avibactam vs. Colistin for KPC
A multicenter retrospective study demonstrating superior outcomes with ceftazidime-avibactam compared to colistin-based regimens for KPC-producing Klebsiella bacteremia, with significantly lower mortality and nephrotoxicity.
Search PubMed -
Aitken et al. (2017) — Aztreonam Plus Ceftazidime-Avibactam for NDM
Reporting early clinical cases and in vitro data supporting the aztreonam plus ceftazidime-avibactam combination strategy for NDM-1-producing Enterobacteriaceae where ceftazidime-avibactam alone would be ineffective.
Search PubMed -
Karlowsky et al. (2018) — Cefiderocol Activity Against CRE
In vitro surveillance data demonstrating cefiderocol's broad activity against carbapenem-resistant Enterobacteriaceae including strains harboring NDM, KPC, and OXA-48.
Search PubMed -
Liu et al. (2016) — MCR-1 Plasmid-Mediated Colistin Resistance
The original publication identifying the mcr-1 gene conferring transferable colistin resistance in livestock and human isolates in China, with implications for the last lines of CRE therapy.
Search PubMed -
Wittebole et al. (2014) / Phage Therapy Review
A historical perspective and current clinical evidence review for bacteriophage therapy as an alternative or adjunct to antibiotics for treatment of drug-resistant gram-negative infections, including CRE.
Search PubMed -
Cassini et al. (2016) — WHO Priority Pathogen List Development
The research process and scoring methodology behind the WHO's 2017 Priority Pathogen List, explaining why CRKP was placed in the Critical tier above hundreds of other resistant organisms.
Search PubMed -
Bassetti et al. (2020) — Cefiderocol CREDIBLE-CR Trial
Results of the CREDIBLE-CR phase 3 clinical trial evaluating cefiderocol against best available therapy for CRE, carbapenem-resistant Acinetobacter, and Pseudomonas infections, with analysis of the all-cause mortality signal.
Search PubMed
Connections
- All Bacteria
- Klebsiella Pneumoniae — Overview
- Klebsiella Treatments Hub
- Beta-Lactam and Aminoglycoside Treatment
- Hospital Infection Control and Prevention
- Diagnosis: Blood Cultures and Imaging
- Hospital-Acquired Pneumonia and UTI
- Escherichia coli (E. coli)
- Pseudomonas Aeruginosa